
Abstract
Background
In cancer, quality of life (QoL) is an important patient-reported metric; evaluating how patients feel physically and emotionally while fighting the disease could lead to better treatment. Despite its therapeutic effects, chemotherapy treatment causes a plethora of side effects that can affect QoL. Factors affecting the QoL of cancer patients undergoing chemotherapy treatment in Ethiopia have not been thoroughly investigated. As a result, this study assesses QoL and associated characteristics among adult cancer patients receiving chemotherapy at Amhara Region, Ethiopia in 2021.
Martials and Methods
From February 15 to May 15, 2021, an institutional based cross-sectional study was done in Amhara region. Three hundred fourteen patients were included in the study. The data was gathered using Amharic version of European organization for research and treatment of cancer quality of life questionnaire (EORTC QLQ C-30) through a face-to-face interview. Epi Data 4.6 was used to enter the data, which was then exported to SPSS version 23 for statistical analysis. Multivariable logistic regression analysis was used to determine the relationship between independent and dependent variables. The statistical significance was determined by a p-value of less than .05.
Result
Cancer patients in Amhara Region had a 44.32 average QoL. Emotional functioning AOR 1.01 (1.0–1.04), social functioning AOR 1.02 (1.01–1.03), nausea and vomiting AOR 0.95 (0.93–0.98), pain AOR 0.95 (0.93–0.98), financial difficulty 0.97 (0.95–0.99), education AOR 4.3 (1.49–12.32), underweight AOR 0.45 (0.24–0.84), > 5th cycle of chemotherapy AOR 4 (1.78–9.11), stage IV cancer AOR 0.21 (0.06–0.71), comorbidity AOR 0.28 (0.14–0.57), anxiety AOR 0.32 (0.12–0.84), and depression AOR 0.29 (0.13–0.63) were all significantly associated with QoL in multivariable logistic regression.
Conclusion
Adult cancer patients receiving chemotherapy in the Amhara region had a poor QoL. Emotional functioning, social functioning, nausea and vomiting, pain, financial difficulty, education, body mass index, cancer stage, chemotherapy cycle, comorbidity, anxiety, and depression all had association with QoL. To improve the QoL of cancer patients, QoL assessments, proper symptom management, nutritional support, and integration of psycho-oncology treatment should be considered.
Introduction
Cancer is one of the most common chronic diseases in both industrialized and developing countries, and it has an impact on every part of the patient's life (Ferlay et al., 2020).
It is the world's second biggest cause of death. Globally, the incident and mortality of cancer was 19.3 million and 9.9 million respectively in the year 2020 (Ferlay et al., 2020). By 2040, the number of new cancer cases and death is predicted to reach 27.5 million and 16.3 million, respectively (Ferlay et al., 2020). Annually, around 74,000 new cancer cases and 52,000 deaths were reported in Ethiopia in 2020. The number of new cancer cases and death is predicted to reach 151,000 and 102,000 respectively in the year 2040 (Ferlay et al., 2020). The overall case fatality from cancer is estimated to be 75% in low-income countries, compared with 46% in high-income countries (Parkin et al., 2020). In Ethiopia, cancer belongs to the second most common non-communicable disease only next to cardiovascular disorders (Federal Democratic Republic of Ethiopia Ministry of Health, 2016).
Being diagnosed with cancer is tremendously stressful event that has a far-reaching implication for the majority of people who have gone through it (Uwamahoro, 2017). Patients with cancer may face a variety of physical, emotional, and economical problem (Chagani et al., 2017; Machuki Ogoncho, 2015; Uwamahoro, 2017). In addition it impaired the family and social roles, which can lead to feelings of ineptitude and lack of confidence (Chagani et al., 2017). Due to its multitude effect cancer has become the century's greatest health problem (Ferlay et al., 2020).
The concept quality of life (QoL) came to focus after World War II and there have been many attempts at the definition of the concept (Poradzisz & Florczak, 2013). The World health organization (WHO) definition of QoL is the most widely used definition and this study adopts it. “Quality of life (QoL) as an individual's perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns”(WHO, 2016). It is a subjective and broad notion that evaluates people holistically and is measured by their health or personal functioning (Ramasubbu et al., 2020; Sema Ustundag, 2015). It is influenced by physiological side effects (hair loss, pain, fatigue, nausea, vomiting), psychological problems (stress, anxiety, depression), social problems (social isolation, role, and function loss), sociodemographic characteristics, diseases and treatment-related factors (stage of cancer, distance metastasis, and treatment modalities) (Chan & Ismail, 2014; Machuki Ogoncho, 2015).
Chemotherapy is a type of systemic chemical therapy that is used to kill rapidly developing cells in the body (Harding, 2020). It is one of the most popular and widely used cancer treatment (Chagani et al., 2017). Unlike other therapies, chemotherapy exhibits systemic side effects that can negatively impact a person's QoL (Chagani et al., 2017). The side effects of chemotherapy affect a person's capacity to work and impair their daily function (Akkuzu et al., 2014). Furthermore, the treatment demands a lengthy course of treatment and frequent hospitalization in order to obtain the desired results, putting a financial strain on patients and reducing their overall QoL (Chagani et al., 2017).
Assessment of patients’ symptoms, functioning, and QoL in everyday oncology practice, has a number of advantages, including the ability to provide clinicians and patients with accurate expectations about the likely impact of treatments on wellbeing and functioning, the ability to identify common problems that will need to be addressed, and the ability to identify therapies and interventions that are effective in solving these problems (Wintner et al., 2016).
Ethiopia is the second most populous country in Africa, after Nigeria with an estimated population of more than 100 million, and is expected to become the ninth most populous country in the world by 2050 (Woldeamanuel et al., 2013). The prevalence of cancer will rise as a result of the changing lifestyles and the expanding population. Oncology treatment services are completely insufficient; with only one radiotherapy treatment center in the country; with a small number of oncologist and nurses, struggles to serve the entire nation (Woldeamanuel et al., 2013).
Studies that evaluate QoL and associated factors are limited, despite the rising frequency of cancer and its debilitating effect on QoL (Araya et al., 2020; Tadele, 2015). The previous studies were conducted at Addis Ababa (Capital city of Ethiopia) with all sorts of treatment methods (Araya et al., 2020; Tadele, 2015). Therefore, they were unable to show the specific burden of chemotherapy treatment can have on the patients QoL. Furthermore, there are key aspects that affect cancer patients’ QoL that have yet to be addressed, particularly in the Ethiopian context, such as body mass index (BMI) (de Carvalho Pazzini Maia et al., 2020), anxiety, depression (Akhtari-Zavare et al., 2018), and functional performance (Pandey et al., 2015). As a result, the goal of this study was to evaluate the QoL and associated characteristics among adult cancer patients undertaking chemotherapy treatment in Amhara National Regional State, Ethiopia.
Literature Review
QoL of Cancer Patients Undergoing Chemotherapy
A study on the QoL cancer patients in Nepal, India, and Pakistan found that participants had a QoL mean score of 85.5, 61.9, and 57.4 respectively indicating good QoL (Chagani et al., 2017; Pandey et al., 2015; Ramasubbu et al., 2020). A study in Tanzania and Rwanda revealed that, the overall QoL mean score was below average with a mean of 49.5 and 28.76 respectively indicating poor QoL (Masika et al., 2012; Uwamahoro, 2017). A study comparing the level of QoL of Ethiopian cancer patients with German cancer patients found that the Ethiopian patients had lower QoL (Wondie & Hinz, 2020).
The Symptoms Experienced by Cancer Patients Undergoing Chemotherapy
A study conducted in Brazil, Malaysia, and Pakistan discovered that nausea/vomiting are highly associated with QoL which affected their ability for self and family care (Akhtari-Zavare et al., 2018; Chagani et al., 2017; De Souza et al., 2015). A study on the prevalence of chemo-induced nausea and vomiting, and its impact on QoL at Addis Ababa, in Ethiopia, showed 76.8% and 64.1% of patient experienced chemotherapy-induced nausea and vomiting respectively, and it was associated with poor QoL (Negusu, 2015). Another study in Ethiopia at Gondar found that the most bothersome symptoms were nausea and vomiting and correlated with QoL (Abegaz et al., 2018). A study in Nepal and Rwanda revealed among pain was highly negatively correlated with QoL (Pandey et al., 2015; Uwamahoro, 2017).
Factors Associated With Quality of Life
Sociodemographic characteristics
The impact of sociodemographic characteristics on the QoL is inconsistent and variable. A facility-based cross-sectional study in Greece, Egypt, and Ethiopia showed that there is no correlation between QoL and age, sex, marital status, occupational status (Abou El Azayiem Bayumi & Shehata Mohamed, 2016; Tadele, 2015; Vrettos et al., 2012). A study in Malaysia and Jordan showed age, religion, educational level, and working status were significantly associated with all QoL (Akhtari-Zavare et al., 2018; Mosleh, 2018).
A study in Pakistan showed that the magnitude of cancer-related financial difficulty was a more significant predictor of QoL than age, education, and marital status (Chagani et al., 2017). A study in Tanzania, Rwanda, Addis Ababa, and Gondar reported, patients have high financial difficulties and associated with poor QoL (Abegaz et al., 2018; Masika et al., 2012; Tadele, 2015; Uwamahoro, 2017). This illustrates that the financial burden of cancer patients in developing countries is considerably high and this factor is relevant for QoL of cancer patients in developing countries (Uwamahoro, 2017).
Psychological factors
A cancer diagnosis is a traumatic event that has a significant impact on the patients and their families and may cause responses of shock, uncertainty, hopelessness, anxiety, and depression (Şahin & Tan, 2012). A study in Malaysia, Jordan, Lebanon, and Ghana showed both anxiety and depression were significantly correlated with worse QoL score (Akel et al., 2017; Akhtari-Zavare et al., 2018; Kugbey et al., 2019; Mosleh, 2018).
Clinical characteristics
Cancer and its treatment affect the nutritional status of patients by altering their metabolic function and reducing their food intake (Hébuterne et al., 2014). A systematic review on the relationship between nutritional status and QoL in cancer patients showed better nutritional status was associated with a better QoL (Lis et al., 2012). A study in Mexico showed that the mean QoL of patients having weight loss of 10% was 48.8, which is lower compared to 62.8 among patients without weight loss and significantly associated with QoL (Sánchez-Lara et al., 2013). A study in Brazil and Oman reported that malnutrition is significantly associated with increased morbidity and mortality, diminished chances of survival, and worse QoL (Cepeda Marte et al., 2019; Salvetti et al., 2020).
A study in Nepal and Malaysia showed advanced stage of cancer associated with poor QoL (Akhtari-Zavare et al., 2018; Pandey et al., 2015). A Study in Ethiopia at Addis Ababa and Gondar revealed that there was a significant decline in QoL of patients having Stage IV tumors compared with stage II and III (Abegaz et al., 2018; Araya et al., 2020). On the contrary, a study conducted in Jordan and Ethiopia at TASH shows the stage of cancer was not significantly correlated with QoL (Al Qadire & Al Khalaileh, 2014; Tadele, 2015). A facility-based cross-sectional study in China and Iran showed patients with one or more comorbid conditions scored significantly worse global QoL, compared to patients without comorbidity (Hekmatpou & Mehrabi, 2018; Wang et al., 2015).
Methods
Design
From February 15 to May 15, 2021, a cross-sectional study was conducted using simple random sampling technique at Felege Hiwot Comprehensive Specialized Hospital (FHCSH) and University of Gondar Specialized Hospital (UGSH), Amhara Region, Ethiopia.
Research Questions
What is the status of QoL cancer patients undergoing chemotherapy treatment in Amhara region, Ethiopia?
Which factors affect the QoL cancer patients undergoing chemotherapy in Amhara region, Ethiopia??
Sample
The sample size was calculated using a single population proportion with a 5% margin of error (d), a 95% confidence interval (alpha = 0.05), and the proportion of poor QoL at UGSH was 52.7% (p = .527) (Abegaz et al., 2018).
ni = initial sample size.
Zα/2 = 1.96 (Z = score corresponds to 95% confidence level).
P = proportion of poor QoL of cancer patients.
q = proportion of good QoL of cancer patients.
d2 = margin of error (0.05)


Inclusion/Exclusion Criteria
The study included cancer patients who were at least 18 years old and available at the time of data collection, those who had received at least one round of chemotherapy treatment, regardless of the cancer type. Patients with hearing or communication problems were excluded from the study.
Measurements
The data were collected through an interview at FHCSH and UoGSH oncology treatment center during their chemotherapy visit. Patients who fulfilled the eligibility criteria were interviewed in the study. Each participant was individually interviewed after explaining the purpose of the study and obtaining an informed consent for participation in the study. Adequate training and supervision was provided for the data collectors. The filled questionnaire was checked for completeness by data collector and supervisor every day. Computer frequencies and data sorting used to check for missed variables, outliers, or other errors during data entry.
After evaluating the literature, the authors constructed questionnaires to collect socio-demographic and clinical data about cancer and chemotherapy. The clinical data was extracted from the medical chart.
The Amharic version of the EORTC QLQ-C30 (European Organization for Research and Treatment of Cancer quality of life) questionnaire was used to assess QoL. It is the primary questionnaire used to assess cancer patients’ QoL. The questionnaire includes both multi-item scales and single-item measures. The instrument contains 30 items among which five functional scales (physical, role, cognitive, emotional, and social functioning), three symptom scales (fatigue, pain, and nausea or vomiting), a two-item global health/QoL scale, and six single items (financial difficulties and other symptoms dyspnea, appetite loss, insomnia, constipation, diarrhea) make up the 30 items. The global health status (QoL) scale was used to assess the overall QoL state of the patient. It comprises of two questions: “How would you evaluate your overall health over the past week?” and “How would you rate your overall quality of life over the past week?” On a 7-point numerical rating scale, 1 represents “Very Poor” and 7 represents “Excellent.” This metric has been shown to be effective and trustworthy in assessing patients’ self-perceived overall QoL (Smith et al., 2014).
In all cases, the scoring principle of EORTC QLQ-C30 is the same. First to estimate the average of the items that share to the scale (raw score) and standardize the raw score using a linear transformation to 100 score. A higher score represents a better level of functioning, or worse level of symptoms (Fayers et al., 2001). The Amharic version of the tool is valid and reliable to use in cancer patients in Ethiopia (Ayana et al., 2018). The tool demonstrated a reliability with Cronbach's α coefficient of 0.87 (Ayana et al., 2018).
A Wealth index questionnaire was used to analyze the wealth status of patients (ICF, 2019). It consists of 19 questions that used to measure housing conditions and household characteristics. Principal component analysis was used to compute and minimize the number of variables (PCA). Then, using an Ethiopian demographic health survey, they were divided into five quintiles (ICF, 2019).
The Amharic version of the Eastern Cooperative Oncology Group Performance Status (ECOG-PS) questionnaire was used to measure the patient's ability to undertake activities of daily living (Azam et al., 2019). It is widely used to determine how the condition affects the patient's capacity to perform daily tasks, which are graded on a scale of 0 (totally active) to 4 (bedridden) and were given a score of 0–1 for good status, and 2–4 for bad status (Araya et al., 2020). Higher scores indicate poor function (Araya et al., 2020; Azam et al., 2019). The tool is valid and reliable in Ethiopia (Ayana et al., 2018).
The Hospital Anxiety and Depression (HAD) Questionnaire was used to assess the patient's anxiety and depression levels. It is a valid and reliable questionnaire that was developed to measure mental problems (such as anxiety and depression) in general medical settings (Akhtari-Zavare et al., 2018; Wondie et al., 2020). The HAD is made up of 14 items separated into two subscales (anxiety and depression), each with seven items, and is scored on a four-point Likert scale ranging from 0 to 3, with 0 being the most favorable response and 3 being the least pleasant. Each subscale's score is calculated, and values of 11 or greater are deemed to indicate a depression or anxiety illness. Scores of 7 or less indicate that the person should not be regarded a case, while scores of 8 to 10 are deemed borderline findings (Wondie et al., 2020). The psychometric properties of Amharic version of HADS Questionnaire in cancer patient had a good reliability with Cronbach's α coefficients of 0.91 (total scale), 0.86 (anxiety scale), and 0.85 (depression scale) (Wondie et al., 2020).
BMI is calculated by dividing weight in kilogram by height in meter squared. The weight is rounded up to the nearest 0.5 kg, while the height is rounded down to the nearest 0.5 cm. Underweight is defined as a BMI of less than 18.5 kg/
Operational Definitions
When the mean score of global health status (QoL) is 50 and above, it is considered good QoL (Araya et al., 2020; Hassen et al., 2019).
Comorbidity: Any chronic clinical entity that exists alongside with cancer (Sarfati et al., 2016).
Statistical Analysis
Data was entered into Epi-data 4.2, and then exported to SPSS Version 23 for analysis. Simple binary regression analyses were used to investigate the first connection between each independent variable and dependent variable. Then, to account for cofounders and discover predictors of QoL, those independent variables with a p-value of less than .25 were sent to multivariable logistic regression. The statistical significance was determined by a p-value of < .05, and the strength of the link was determined by an AOR with a 95% confidence range. The Hosmer and Lemeshow goodness of fit test was used to assess model fitness.
Results
Sample Characteristics
Socio demographic and clinical characteristics of the respondents
Out of 314 respondents intended to be included in the study, a total of 310 patients participated and gave a response rate of 98.7%. Of the respondents, 219 (69.7%) were female, 175 (57.8%) were below the age group of 50 with a mean (SD) age of 45.81 years (10.98). More than half of the participants, 66 (54.2%), have no formal education. About 219 (70.6%) were married.
Breast cancer was the leading type of cancer which accounts for 25.5%. The mean length of time since their diagnosis was 14.95 months. The majority of the participants, 175 (56.5%), had a normal BMI. Seventy-one (22.9%) of participants had comorbid diseases. One hundred thirty-two (42.6%) of participants were at stage III of cancer. The mean (SD) of anxiety and depression subscale scores was 8.83 (3.287), and 9.29 (4.177), respectively (Table 1).
Socio-Demographic and Clinical Characteristics of Adult Cancer Patients Under Chemotherapy Treatment at FHCSH and UGSH, Ethiopia 2021.

n = 310.
Student, pension, daily laborer.
Colorectal, gastric, esophageal.
Cervical, ovarian, GTD.
Asthma, HIV/AIDS.
Research Question Results
Status of quality of life of the respondents
The mean QoL of the study participants was 47.63 with a standard deviation of 10.068 and 43.23% of the participants had good QoL.
Functional and symptom scale scores of EORTC QLQ C-30
The functional scale of study participants ranged from a mean (SD) of 44.48 (21.29) for emotional functioning to cognitive functioning 61.07 (21.44). The most affected functional scale was emotional functioning, with 189 (61%) participants scored poor QoL, whereas the cognitive functioning state was the least affected functional scale with majority 238 (76.8%) of participants scored good QoL. From symptoms, appetite loss was the most affected, 239 (77.1%), of participant's scored Poor QoL (Table 2).
Functional and Symptom Scale Score Among Adult Cancer Patient Undertaking Chemotherapy Treatment at FHCSH and UGSH, Ethiopia, 2021.
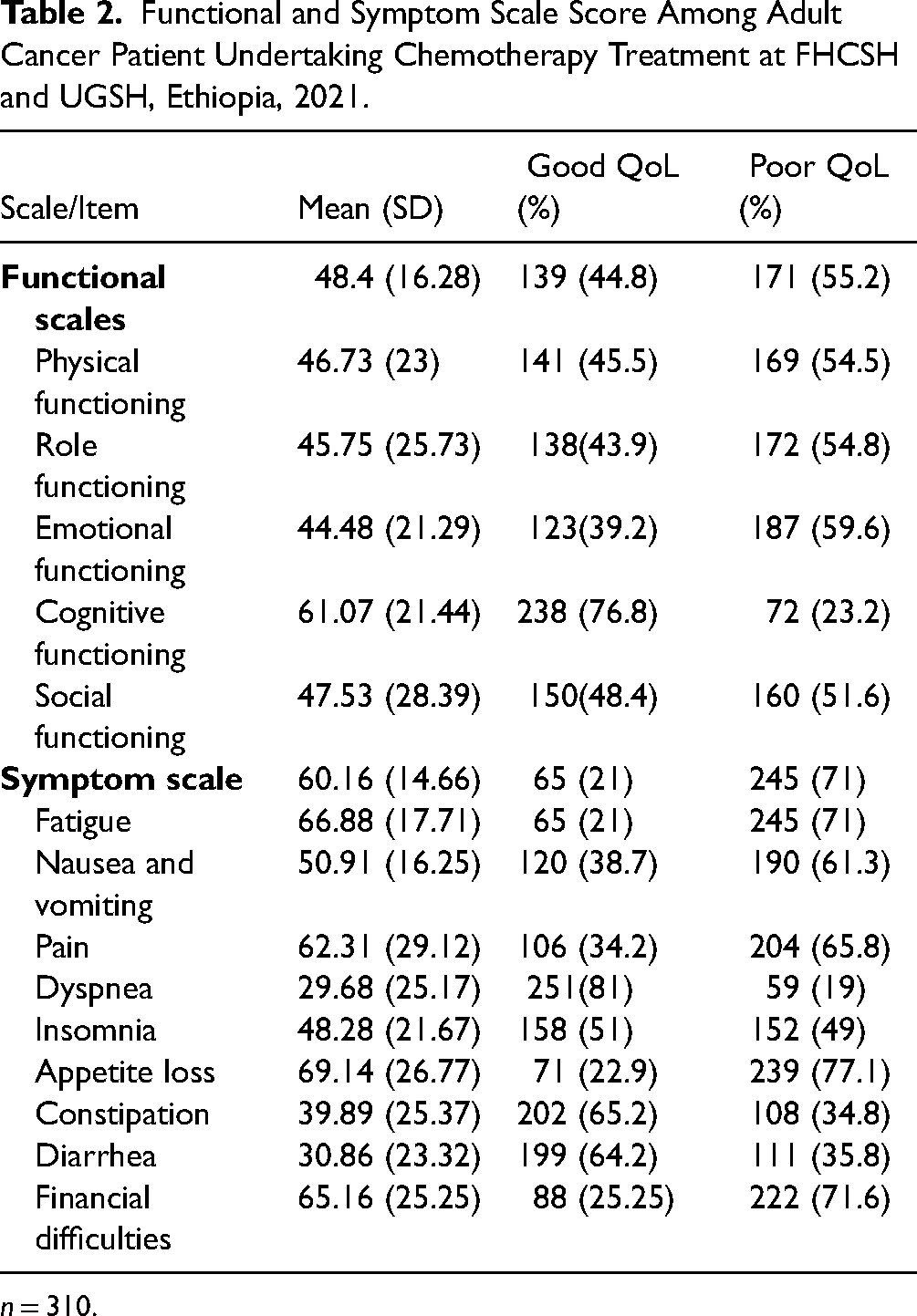
n = 310.
Factors associated with quality of life
This study shows multiple factors associated with QoL. The bivariable logistic regression analysis shows, all functional items, symptoms except dyspnea and diarrhea, educational status, marital status, occupational status, BMI, type of cancer, cycles of chemotherapy, stage of cancer, ECOG performance status, comorbidity, anxiety, and depression were associated with QoL at p < .25 and entered for multivariable analysis.
In the multivariable analysis, emotional functioning, social functioning, financial difficulty, pain, nausea and vomiting, educational status, BMI, stage of cancer, comorbidity, anxiety, depression, and the cycle of chemotherapy treatment had significant association with QoL. The multivariable analysis showed that adult cancer patients with good emotional and social functioning had 1.03 and 1.02 times more likely to have good QoL with AOR 1.02 (1.01–1.03) and 1.02 (1.01–1.03), respectively.
Patients with nausea and vomiting, pain, and financial difficulty had 5% AOR 0.95 (0.93–0.98), 5% AOR 0.95 (0.93–0.98), and 3% AOR 0.97 (0.95–0.99) less likely to have good QoL, respectively (Table 3).
Association Between EORTC QLQ-C30 Functioning and Symptom Scales With QoL of Adult Cancer Patients Undertaking Chemotherapy Treatment at ANRS, Ethiopia, 2021.

n = 310.
**Significant level at p < .01; *significant level at p < .05; / indicates not included in the model.
Patients with educational level of college and above had 4.3 times more likely to have good QoL AOR 4.3 (1.49–12.32) as compared to patients who had no formal education.
Besides, patients whose BMI < 18.5 is 55% less likely to have good QoL compared with normal weight participants with AOR 0.45 (0.24–0.84). Similarly, patients who are at an advanced stage of cancer (stage IV) were 79% less likely to have good QoL than patients with an early stage of cancer (stage I) with AOR 0.21 (0.06–0.71). Those who had comorbid diseases were 72% less likely to have good QoL as compared with those who had no comorbid diseases AOR 0.28 (0.14–0.57).
Anxiety and depression affect the QoL of cancer patients. This study shows patients with anxiety 68% less likely to have good QoL than normal individuals AOR 0.32 (0.12–0.84) and patients with depression, 71% less likely to have good QoL than normal individuals AOR 0.29 (0.13–0.63).
QoL improves with chemotherapy treatment. Patients who took five and above cycles of chemotherapy treatment had four times more likely to have good QoL AOR 4 (1.78–9.11) than those who took two cycles of chemotherapy treatment (Table 4).
Bivariable and Multivariable Logistic Regression of Determinant Factors With QoL of Adult Cancer Patients Under Chemotherapy at ANRS, Ethiopia, 2021.

n = 310.
**Significant level at p < .01; *Significant level at p < .05; / indicates not included in the model.
Discussion
Cancer and its treatment strategies substantially affect the QoL of patients. Estimation of QoL of patients living with cancer helps to evaluate the effectiveness of treatment. In Ethiopia, QoL measurement is not performed in cancer patients routinely. This is an institution-based cross-sectional study aimed to assess the QoL, and associated factors among adult cancer patients undergoing chemotherapy treatment at Amhara National Regional State, Ethiopia, 2021.
This study has shown that the mean score of QoL was found to be 44.32. This finding is lower than studies conducted in Nepal 85.54 (Pandey et al., 2015), India 61.93 (Ramasubbu et al., 2020), and Pakistan 57.37 (Chagani et al., 2017). A low level of QoL in this study could be explained by less availability of screening program for cancer patients in Ethiopia, patients usually admitted once they are at an advanced stage, which may necessitate for frequent hospital visits, this in turn may cause psychological and economic stress, resulting in poor QoL (Hassen et al., 2019). Economic hardship, long waiting time to get the treatment, and the relative lack of well-resourced cancer treatment center in the study setting has also an influence in the QoL (Abegaz et al., 2018; Hassen et al., 2019).
In this study, emotional functioning, social functioning, nausea and vomiting, pain, financial difficulty, educational status, BMI, stage of cancer, cycle of chemotherapy treatment, comorbidity, anxiety and depressions were found to be significantly associated with QoL.
According to the results of this study, from functional status scale both emotional and social functioning are associated with QoL which is consistent with studies conducted in Brazil, Turkish, and Pakistan (Chagani et al., 2017; Lobo et al., 2014; Sema Ustundag, 2015). A reduced emotional and social functioning might be due to the fact that most of the cancer patients in this study have an advanced stage of cancer, when they become ill, they have a disruption in their usual role at home, work, and social stigma related to cancer diagnosis (Bekele, 2016). Furthermore, worry about their children's future also affects their emotion that leads to poor QoL (Bekele, 2016; Hassen et al., 2019).
Despite the use of health insurances in Ethiopia, financial difficulties significantly correlated with QoL. This finding is consistent with a study conducted in Addis Ababa, Gondar, and Rwanda (Abegaz et al., 2018; Hassen et al., 2019; Uwamahoro, 2017). Cancer patients in developing countries face a significantly higher financial challenge because chemotherapy is a lengthy and expensive treatment that creates a financial burden for cancer patients (Uwamahoro, 2017). In addition, two-third of the patients in this study came from countryside so they have a transport fees while travelling from their home to the hospital, and since the study groups are adult population, it affects their work life that have an overall effect on the family's economy; all these factors magnify their financial difficulties. This is contrary to studies in the USA and German (Carrera et al., 2018; Hinz et al., 2014). This discrepancy might be due to financial difficulty, poor coverage of health insurances, and inaccessibility of cancer treatment facilities in the Ethiopian setting (Ayana et al., 2018; Wondie & Hinz, 2020).
This study shows that nausea and vomiting significantly affect QoL of cancer patients. This finding was in line with studies conducted in Pakistan and Malaysia (Akhtari-Zavare et al., 2018; Chagani et al., 2017). This may be due to nausea/vomiting was found to affect routine activities of patients including household activities, feeding style, and daily function that it can affect the QoL of patients (Bekele, 2016).
Patients with cancer frequently experience pain as a result of their disease or treatment strategies. This study shows pain is one of the most distressing symptoms of cancer that affects their QoL. This finding was consistent with the study in Iran, Nepal, and Addis Ababa (Abdollahzadeh et al., 2012; Pandey et al., 2015; Tadele, 2015). This could be due to pain causes worry and emotional anguish, obstruct functional capacity, and makes it more difficult to carry out one's duties in the family, society, and at work (Abegaz et al., 2018; Hassen et al., 2019).
In this study, educational status of college and above had 4.3 times more likely to have good QoL as compared to patients who had no formal education. This finding is in line with previous studies conducted in Addis Ababa, Kenya, and Jordan (Hassen et al., 2019; Machuki Ogoncho, 2015; Mosleh, 2018). Education is one of the important factors that help in promoting QoL. This could be due to patients with higher educational status have better knowledge than illiterate patients in terms of diagnosis and follow-up care which ultimately improves their overall QoL (Hassen et al., 2019; Machuki Ogoncho, 2015).
BMI was also another variable which was significantly associated with poor QoL. Participants with BMI < 18.5 kg/m2 is 55% less likely to have good QoL compared with participants who have normal BMI. This was consistent with studies conducted in Mexico, Brazil, and Korea (Bjelic-Radisic et al., 2012; Nho et al., 2014; Sánchez-Lara et al., 2013). This could be due to malnutrition is linked to a decline in the functional ability, increase the number and duration of hospital admissions, experienced worse symptoms, anxiety and depression; all of which can lead to poor QoL (de Carvalho Pazzini Maia et al., 2020).
Respondents with stage IV cancer were 79% less likely to have a better QoL than patients with an early stage of cancer (stage I). This finding was consistent with studies conducted in Addis Ababa, Gondar, and Jordan (Abegaz et al., 2018; Araya et al., 2020; Mosleh, 2018). This could be due to in this study more than 70% of participants are at stage III and above which are linked with more symptoms, anxiety, depression, poor physical and emotional functioning that affect their overall QoL. As the disease progresses, it will bring more discomforting symptoms, impairment in physical functioning, and they have more stress, anxiety, and depression that are more likely to affect their QoL (Mosleh, 2018; Ramasubbu et al., 2020).
Cycle of chemotherapy treatment was also another variable which had a significant association with patients’ QoL. Patients who took five and above cycles of chemotherapy treatment had four times more likely to have good QoL than those who took two cycles of chemotherapy treatment. These results are consistent with studies conducted in Egypt and Iran (Abdollahzadeh et al., 2012; Abou El Azayiem Bayumi & Shehata Mohamed, 2016). This could be due to chemotherapy very often induces acute side-effects that usually develop at the end of the first cycle and beyond that worsen the QoL of patients. Later an improvement in their health condition and subsidization of symptoms improve their QoL (Akhtari-Zavare et al., 2018; Hassen et al., 2019).
This study also showed that cancer patients with comorbidity diseases were 72% less likely to have good QoL as compared with those who had no comorbid diseases. The finding of this study is consistent with previous researches done in China and Iran study (Hekmatpou & Mehrabi, 2018; Wang et al., 2015). This could be due to that comorbid disease can compromise the QoL through increasing symptoms, impairment on functional wellbeing, and anxiety that can affect their overall QoL (Fu et al., 2015).
Anxiety and depressions are also other variables which had significant associations with poor QoL. Patients with anxiety and depression were 68% and 71% less likely to have good QoL than normal individuals, respectively. This finding was consistent with Gahanna, Jordan, Lebanon, and Malaysia studies (Akel et al., 2017; Akhtari-Zavare et al., 2018; Kugbey et al., 2019; Mosleh, 2018). This could be because of treatment side-effect, uncertainty related to prognosis, and the treatment modality in this setting are mostly disease-centered and the patients’ psychosocial well-being is largely undermined.
Strengths and Limitations
The potential limitations of this study are: first, the QoL data was collected by interview and it is subjected to social desirability bias. Second, the BMI is used for assessing nutritional status owing to its own limitations; therefore, a comprehensive nutritional assessment was not done. Third, for the sake of interpretation the outcome variable has been dichotomized into two. This might result in underestimating the extent of variation in the outcome between groups, such as the association of some events, and considerable variability may be subsumed within each group. Despite its limitations, this study was the first attempt to determine QoL and associated factors of cancer patients in Amhara region. It uses standardized, validated, and reliable tool to measure QoL.
Implication for Practices
The finding of this study has implication for health-care professionals, cancer institutions, non-governmental funding agencies, and to the Ministry of Health. This study underlines the significance of addressing the QoL in cancer patients. The findings from this study can be used to integrate QoL as a routine assessment for people with cancer in Ethiopia. Hence, this study underlines the need to give economic support, psychological support, proper pain and vomiting management should be included to improve the QoL of cancer patients.
Conclusion
Adult cancer patients receiving chemotherapy in the Amhara region had a poor QoL. Emotional functioning, social functioning, nausea and vomiting, pain, financial difficulty, education, BMI, cancer stage, chemotherapy cycle, comorbidity, anxiety, and depression all had a substantial impact on QoL. To improve the QoL of cancer patients undergoing chemotherapy, QoL assessments, proper symptom management, nutritional support, and integration of psycho-oncology treatment should be considered.
Footnotes
Abbreviations
Acknowledgements
We are thankful to Bahir Dar University, Amhara region referral hospital leaders, study participants, data collectors, and supervisors for the support of the overall process of the study.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Data Availability Statement
The data of this study can’t be shared publicly due to presence of sensitive (confidential) participants’ information.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Informed Consent
Ethical clearance was obtained from the institutional review board of Bahir Dar University, College of Medicine and Health Science to conduct the research with a protocol No 051/2021. A formal letter was submitted to FHCSH and UGSH, informed verbal consents were obtained from the study participants after clearly introducing the purpose of the study. The respondents’ right to refuse or withdraw from participating in the interview at any time was fully respected and the information provided by each respondent was kept confidential by making each questionnaire coded and not sharing personal information of any patient to the third party.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.