
Abstract
Introduction
The increasing number of women with breast cancer undergoing chemotherapy may result in long-lasting, adverse physical side effects and reduced quality of life.
Objective
This study aimed to develop and assess the feasibility and preliminary effects of the Phone-Based Support Program for women with breast cancer undergoing chemotherapy. The primary outcome was self-care self-efficacy; secondary outcomes were symptom distress and quality of life.
Methods
This pilot study was conducted at a tertiary hospital in Jiangsu province, China, from February to March 2023. The Phone-Based Support Program was delivered to 20 participants through the smartphone application WeChat, consisting of learning, discussion, ask-the-expert, and personal stories components. Outcome measures were assessed at three time points: preintervention, postintervention, and follow-up.
Results
The Phone-Based Support Program was feasible and could improve self-care self-efficacy, decrease symptom distress, and promote quality of life. The program was well-accepted, and participants engaged actively in the online discussion and sought expert advice.
Conclusions
The Phone-Based Support Program showed feasibility and effectiveness in improving self-care self-efficacy, reducing symptom distress, and enhancing quality of life.
Keywords
Introduction
Breast cancer is the most common and deadly cancer among women worldwide (Sung et al., 2021). In 2020, breast cancer accounted for approximately 11.7% of total cancer cases globally, with an incidence rate of 47.8 per 100,000 and a mortality rate of 13.6 per 100,000 (Bashar & Begam, 2022). In China, it is the leading cancer among women aged 30 to 54 (Cao et al., 2021). The diagnosis of breast cancer has significant consequential effects on all aspects of women's lives. The primary treatment for breast cancer is surgery, usually followed by 8 months to a year of radiotherapy, chemotherapy, and hormonal therapy (Cornette et al., 2016; Wang et al., 2019).
Chemotherapy, while critical for treatment, is known for its significant side effects. Patients often experience a range of physical and psychological disturbances, such as pain, insomnia, nausea, loss of appetite, fatigue, hair loss, depression, anxiety, and worry (Ariza-Garcia et al., 2019; Bao et al., 2018). These side effects can substantially impact patients’ well-being, necessitating interventions to manage them effectively and improve the quality of life (QOL) during treatment. The stress and symptom burden associated with breast cancer diagnosis and subsequent therapies like chemotherapy are well-documented. The side effects related to treatments, however temporary, can influence women's QOL (Andreu et al., 2022; Hassen et al., 2019), potentially compromising it (Park et al., 2020).
Given the challenges confronting women being treated for breast cancer, there is a pressing need for supportive interventions that can aid women in coping with the side effects of chemotherapy to enhance their overall well-being. This study aimed to develop and assess the feasibility and preliminary impact of a Phone-Based Support Program (PBSP) for women undergoing chemotherapy for breast cancer. The program's objective was to improve self-care self-efficacy (SCSE) as a primary outcome, reduce symptom distress, and enhance QOL as a secondary outcome.
Review of Literature
Patients with newly diagnosed breast cancer who are undergoing chemotherapy may have low self-efficacy in performing tasks for themselves (Oh et al., 2020). Low self-efficacy negatively impacts patients’ psychological well-being, leading to increased symptom distress and decreased QOL (Chovanec et al., 2021). Self-efficacy, particularly in the context of self-care, plays a pivotal role in how patients manage their treatment and cope with the side effects of breast cancer therapies like chemotherapy. Self-efficacy theory posits that an individual's belief in their ability to execute actions is crucial in their psychological adjustment to chronic illnesses (Bandura, 1997). Self-efficacy attributes include direct mastery experiences, vicarious experiences, verbal persuasion, and arousal state. Higher levels of SCSE have been linked to better symptom management, reduced psychological distress, and improved QOL in cancer patients (Kirca & Kutlutürkan, 2021). For instance, interventions aimed at enhancing SCSE in patients undergoing hemodialysis have demonstrated significant improvements in depression and QOL (Gibbons et al., 2020). This underscores the importance of SCSE in fostering effective self-care practices, especially in managing the adverse effects of chemotherapy.
Symptom distress is the amount of suffering that occurs as a response to the presence of symptoms (Carrozzino et al., 2023). It may be psychological, emotional, social, or spiritual and can interfere with how patients cope or manage their symptoms (Toledo et al., 2021). Women with breast cancer who have yet to undergo surgery or other treatments can have patterns of significant symptom distress and burden related to mood and sleep disturbances, fatigue, pain, and changes in cognitive functioning (Matthys et al., 2021). Symptom distress can persist postsurgery, during chemotherapy, and into survivorship (Madison et al., 2021).
The Internet and mobile technologies have transformed patient self-care, offering new information dissemination and support avenues. Internet-based interventions can significantly facilitate patient–healthcare professional interactions and provide a platform for effectively transmitting health information (Usak et al., 2020). Mobile phone applications, in particular, have effectively improved self-care behaviors in various patient populations (Son et al., 2020). In the context of breast cancer, mobile applications have been instrumental in reducing symptom distress, enhancing social support, and promoting SCSE among patients (Sohrabei & Atashi, 2021; Zhu et al., 2018). This evidence highlights the potential of mobile health interventions in augmenting traditional care methods and empowering patients in self-management.
The PBSP, a novel intervention created for this study, aimed to integrate the principles of self-efficacy with the accessibility and convenience of mobile technology. The program was designed to offer structured support and resources through a mobile platform, focusing on improving SCSE, reducing symptom distress, and enhancing the QOL among women undergoing chemotherapy for breast cancer. The PBSP incorporated interactive components to strengthen women's self-efficacy in managing their treatment and its side effects.
Methods
Design
For this pilot study, a one-group pretest–posttest design was adopted to assess the feasibility and preliminary effects of the PBSP for women with breast cancer undergoing chemotherapy. The primary outcome was SCSE, and the secondary outcomes were symptom distress and QOL. The outcomes were assessed at three time points: preintervention (T1, week 0), postintervention (T2, week 3), and follow-up (T3, week 7). The hypotheses were that the study's participants would report increased SCSE, decreased symptom distress, and enhanced QOL after completing the PBSP (T2 and T3).
Participants and Setting
A convenience sample of women newly diagnosed with breast cancer undergoing chemotherapy was recruited by the primary investigator (PI) at a tertiary hospital's oncology department in Jiangsu province, China. The inclusion criteria included: (a) females at least 18 years of age, (b) newly diagnosed with nonmetastatic breast cancer (stage II or lower) within the past 3–8 weeks, (c) received chemotherapy after surgery, (d) able to access the Internet with a smartphone, (e) contactable via the smartphone for follow-up, and (f) able to communicate in Mandarin Chinese. The exclusion criteria were: (a) having a concurrent major or advanced chronic physical illness/injuries with the potential for lifelong disability (including recent surgery other than for breast cancer), profound coma, permanent paralysis, or severe brain injury; (b) having a chronic mental health problem diagnosed by a psychiatrist; or (c) unable to complete all sessions of the PBSP implementation.
Ethical Consideration
Two institutional review boards approved the study protocol and research instruments: at Burapha University in Thailand (#G-H103/2565) and the site hospital in China (#2022-K-103). The PI informed potential participants about the research objectives, the data collection method, the potential risks and benefits, and the right to discontinue involvement in the study without any consequences affecting treatments. The PI explained how confidentiality would be maintained throughout the study. Those who volunteered to participate signed a written consent form. To ensure confidentiality in matching pre- and postintervention questionnaires, each participant was assigned a unique numerical identifier rather than using personal names. These numbers were securely stored and only accessible to the PI.
Recruitment Procedures
This pilot study was conducted between February and March 2023 after obtaining approval from the ethics committees. Three of the 25 eligible participants were excluded because they joined another research project, and two refused to participate due to severe stress and unwillingness to complete the questionnaires. A sample size of 20 participants is sufficient for pilot studies in healthcare research to assess intervention feasibility and outcome variability (Julious, 2005). The 20 participants completed the PBSP intervention without attrition.
Participants completed two questionnaires using either a scanned QR code to fill out online or a paper copy with a pen (T1, week 0). They were encouraged to seek assistance or clarification from the PI. The PI checked the questionnaires for completeness of the responses and expressed gratitude for their participation.
The Intervention and Implementation
The PI developed the PBSP intervention based on self-efficacy theory (Bandura, 1997) and a modification of the Breast Cancer e-Support program (Zhu et al., 2018). The minimum recommended number of cycles or standard treatment regimen for intravenous chemotherapy is four cycles, with 3 weeks for each cycle. The PBSP was implemented with the participants for the first cycle only, from the first day of the first cycle to the end of the 3 weeks of the first cycle. The outcomes were measured at the end of the first cycle (T2) and follow-up (T3) at the beginning of the third cycle of chemotherapy.
The PBSP was installed on participants’ smartphones using the social media messaging application Weixin, also known as “WeChat” (Tencent Holding Ltd., Shenzhen, China), which is Android or iOS compatible. The PBSP consisted of four sessions over 3 weeks. It contained four interactive components: (a) a learning group, (b) a discussion group, (c) an ask-the-expert group, and (d) a personal stories group. Week-long interactive groups online were combinations of scheduled synchronous communication and asynchronous texting sessions. The PI acted as the moderator for group discussions and provided expert advice if requested.
In Session 1 (Building relationships) at the hospital department site, the PI provided orientation about the PBSP and WeChat participation, prepared participants for the subsequent three online sessions, and collected demographic data and pretest outcome measures (T1, week 0). The PI provided a recording sheet where participants could take notes from watching videos at home.
Session 2 (Touching PBSP: Learning group) was implemented online on the day after session 1. The PI sent 10 video clips (5–7 min each) on breast cancer knowledge and symptom management strategies to address the women's direct mastery experiences. All knowledge was evidence-based and validated by multidisciplinary Chinese oncology professionals. Participants were to watch each video clip within a week prior to the next session and record comments, problems, or unclear issues.
One week after the last session, Session 3 (Coming into your world) began. In this session, the ask-the-expert and discussion groups online offered opportunities for the participants to interact with one another and a healthcare professional where verbal persuasion and modification of the participants’ perceptions of arousal states occurred. An oncologist joined the PBSP in the ask-the-expert and discussion groups to answer the participants’ questions and discuss about what they had viewed in the videos.
In Session 4 (Together for a Share Future: Personal story group), a week later, the PI sent three video-recorded personal stories via the WeChat group and asked the participants to watch them at that time. The stories included encouraging narratives and personal experiences that the participants could relate to. With the participants’ permission, some critical questions and answers, which might have interested others, were added for discussion. Participants reflected on all prior videos and session activities.
Upon completion of the PBSP, posttest measures were obtained (T2, week 3). Telephone follow-up measures were delivered after the second cycle of drug infusion on the first day of week 7 (T3, week 7). The average time to complete all questionnaires was 20.2 min on site (16–28 min), and the average time to collect data by telephone was 6 min (4–13 min). The flowchart of the implementation sessions is presented in Figure 1.

Flowchart description of the intervention process.
Participants’ Characteristics and Outcome Measures
Prior to the intervention, participants completed a demographic and clinical characteristics questionnaire eliciting their age, marital status, education level, employment status, monthly family income, breast cancer stage, comorbidities, the cycle of chemotherapy, surgery style (treatment with radiotherapy or chemotherapy before surgery), and chemotherapy regimen.
Primary Outcome: Self-Efficacy
Riegel et al. (2018) developed the Self-Care Self-Efficacy Scale (SCSES), a 10-item self-report instrument to measure SCSE behaviors in adults with chronic illness. The domain of self-efficacy includes self-care maintenance (action to maintain physiologic stability; four items), self-care monitoring (actions to track behavior and detect and interpret changes in signs and symptoms; three items), and self-care management (actions to recognize a change in health and address the process to reverse an illness exacerbation; three items). Each item begins with the stem, “How confident are you that you can ….” The phrase “how confident” captures the strength of the belief, while the adjunctive clause refers to an affirmation of the capability of a particular self-care action. Each item is rated on an ordinal scale from 1 to 5 rating scale, with a higher score representing a higher level of self-efficacy. Summed scores are standardized mathematically to range from 0 to 100. The scale has been translated and used with Chinese women (Yu et al., 2021). The content was validated by an expert panel with a content validity index of 0.91; Cronbach's alpha coefficient of the single factor was reported as 0.89 (Yu et al., 2021). In the current pilot study, Cronbach's alpha reliability coefficient (Chinese version) was 0.72.
Secondary Outcomes
Symptom Distress
Cleeland et al. (2000) reported on the development of the MD Anderson Symptom Inventory (MDASI) to measure the severity of symptoms in patients with cancer and the impact of symptoms on daily living. The MDASI assesses 13 symptoms: pain, fatigue (tiredness), nausea, disturbed sleep, being distressed, shortness of breath, difficulty remembering, lack of appetite, feeling drowsy, dry mouth, feeling sad, vomiting, and numbness or tingling. In addition, six items assess symptom interference. Self-reports of symptoms and interference items are rated from 0 (not present) to 10 (as bad as you can imagine). Summed scores can range from 0 to 130, with higher scores indicating increased distress from symptoms. Zhang et al. (2021) translated the MDASI into Chinese. They reported Cronbach's alpha reliability coefficients of 0.74 and 0.88 for the subscales of symptom and interference, respectively. In our study, Cronbach's alpha reliability coefficient was 0.74.
Quality of Life
The European Organisation for Research and Treatment of Cancer (EORTC) undertook the development of a scale to measure QOL in people living with cancer (QLQ-C30). The current version 3 is a 30-item cancer-specific scale with four subscales: (a) functional subscale (15 items) includes physical functioning (items 1–5), role functioning (items 6–7), emotional functioning (items 21–24), cognitive functioning (items 20–25), and social functioning (items 26–27); (b) the symptom subscale (7 items) includes fatigue (items 10, 12, 18), pain (items 9 and 19), and nausea/vomiting (items 14 and 15); (c) the side effects subscale (6 items) includes dyspnea (item 8), appetite loss (item 13), sleep disturbance (item 11), constipation (item 16), diarrhea (item 17), and financial impact (item 28); and (d) the global QOL subscale has two items (items 29–30). Items are rated on a four-point ordinal scale from 1 (not at all) to 4 (very much). Items 29 and 30 in the global QOL subscale are scored on a modified seven-point linear analog scale (Fayers et al., 2001). Higher scores indicate better health for the functioning and global QOL scales. For the symptom subscales, higher scores indicate an increased symptom burden. Scoring of the QLQ-C30 is the sum of [physical, role, emotional, cognitive, and social functioning, (100-fatigue), (100-nausea/vomiting), (100-pain), (100-dyspnea), (100-appetite loss), (100-sleep disturbance), (100-constipation, (100-diarrhea)] divided by 13.
All subscales and individual item scores are transformed to a 0–100 scale, with higher values indicating a higher QOL. The EORTC QLQ-C30 was developed for English-speaking cultures and then translated into Chinese and validated to measure the QOL of Chinese people living with cancer (Wan et al., 2008; Zhao & Kanda, 2000). Wan et al. (2008) reported that the test–retest reliability for most domains was above 0.80 except for appetite loss (0.77) and diarrhea (0.75). In our study, the Chinese version had a Cronbach's alpha reliability coefficient of 0.71.
Statistical Analysis
Data analyses were performed using the IBM SPSS statistical software, version 26.0; the alpha significance level was set at p < .05. Means, standard deviations, and percentages were used to describe the participants’ demographic and clinical characteristics and outcome variables. One-way repeated measure ANOVA was used to test the research hypotheses. Bonferroni post hoc pairwise comparisons between time periods were calculated to analyze the differences in outcomes.
Results
The mean age of participants was 51.4 years (SD = 8.9) (Table 1). Most of them were married (85%), were employed (60%), had an education below high school or diploma (60%), and had a monthly income of less than 500 USD (90%). Table 2 presents the participants’ clinical characteristics using the tumor–node–metastases (TNM) staging system; 65% were in T2N1M0 (a small cancer spread to the lymph nodes but nowhere else), and the rest were in T2N0M0 (a small cancer with no spread). All of them had no comorbidity, received surgery (45% mastectomy and 55% lumpectomy), and received eight cycles of chemotherapy (except one who received four cycles of chemotherapy).
Participants’ Demographic Characteristics (N = 20).

Participants’ Clinical Characteristics (N = 20).
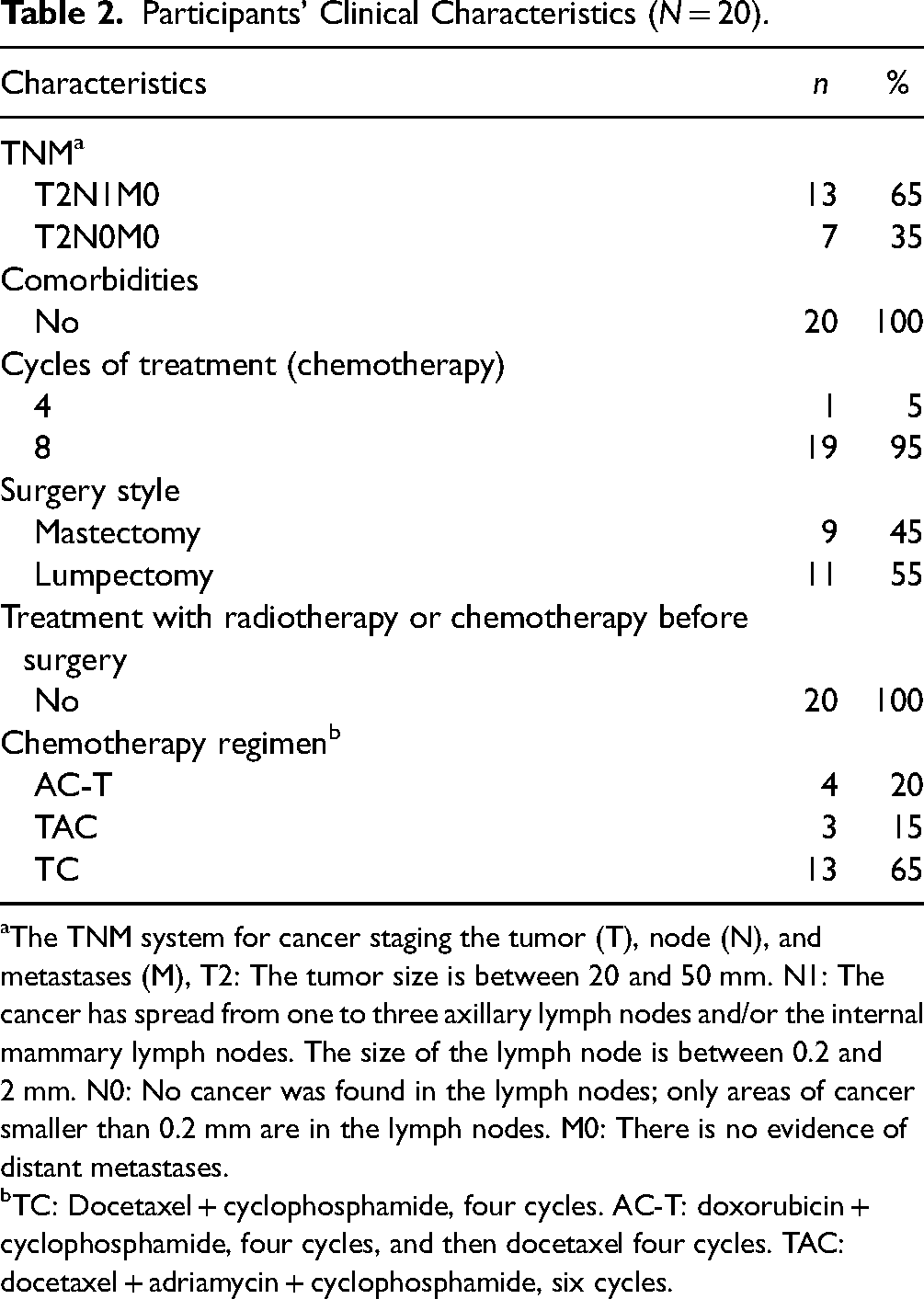
The TNM system for cancer staging the tumor (T), node (N), and metastases (M), T2: The tumor size is between 20 and 50 mm. N1: The cancer has spread from one to three axillary lymph nodes and/or the internal mammary lymph nodes. The size of the lymph node is between 0.2 and 2 mm. N0: No cancer was found in the lymph nodes; only areas of cancer smaller than 0.2 mm are in the lymph nodes. M0: There is no evidence of distant metastases.
TC: Docetaxel + cyclophosphamide, four cycles. AC-T: doxorubicin + cyclophosphamide, four cycles, and then docetaxel four cycles. TAC: docetaxel + adriamycin + cyclophosphamide, six cycles.
Significant changes in outcome measures were observed before and after the intervention and during the follow-up period (Table 3). The one-way repeated measure ANOVA revealed significant differences for the three outcomes across different time points. The F-statistics with p < .05 were 44.5 (partial η2 = 0.832), 44.8 (partial η2 = 0.833), and 52.2 (partial η2 = 0.853) for SCSE, MDASI, and QLQ-C30, respectively, indicating a substantial effect of the intervention on these measures. The SCSE scores showed a notable increase from T1 (M = 74.8, SD = 26.7) to T2 (M = 113.3, SD = 27.1) and T3 (M = 144.8, SD = 26.7), with significant differences between T1 and T2, T1 and T3, and T2 and T3 (Mdiff = −38.5, p < .001; Mdiff = −70.0, p < .001; and Mdiff = −31.5, p < .01, respectively), indicating an improvement in participants’ perceived ability to engage in self-care activities. Similarly, the MDASI scores decreased significantly from T1 (M = 82.6, SD = 8.1) to T2 (M = 68.0, SD = 19.1) and T3 (M = 56.7, SD = 12.2), with significant differences between T1 and T2, T1 and T3, and T2 and T3 (Mdiff = 14.6, p < .05; Mdiff = 25.9, p < .001; and Mdiff = 11.3, p < .01), suggesting a reduction in symptom severity following the intervention. Furthermore, the QLQ-C30 scores showed improvement from T1 (M = 51.1, SD = 6.8) to T2 (M = 63.1, SD = 10.2) and T3 (M = 74.2, SD = 9.6), with significant differences between T1 and T2, T1 and T3, and T2 and T3 (Mdiff = −12.0, p < .01; Mdiff = −23.1, p < .001; and Mdiff = −11.1, p < .05), suggesting a positive impact on participants’ overall QOL after the intervention. This indicates that the intervention positively affected both perceived abilities to engage in self-care activities and overall QOL.
Change Over Time of Total Scores of Self-Care Self-Efficacy, Symptom Distress, and Quality of Life (N = 20).

Note. T1 = preintervention; T2 = postintervention; T3 = follow-up; partial η2 = partial eta square.
Discussion
The PBSP exemplifies a significant advancement in supporting women with breast cancer undergoing chemotherapy, extending traditional patient care models. Using a smartphone application as a form of telenursing helps to enhance self-care SCSE, mitigate symptom distress, and elevate the QOL of the women. Its alignment with emerging trends in technology-based healthcare interventions, as highlighted in studies by Zhu et al. (2018), reflects a paradigm shift toward more accessible and patient-centric cancer care.
The marked increase in SCSE from the PBSP intervention is congruent with the outcomes of Zhang et al. (2018), who demonstrated the importance and impact of nurse-led, technology-enabled interventions in bolstering self-management capabilities among colorectal cancer patients. This evidence underscores the adaptability and efficacy of smartphone applications for telenursing across diverse cancer types and treatment regimes. Moreover, the impact of using smartphone applications in enhancing SCSE extends to other chronic conditions, as evidenced by Hudiyawati et al. (2023), suggesting telenursing's broad applicability and potential in healthcare.
In reducing symptom distress, the PBSP results align with those of Rezaee et al. (2022), reinforcing the pivotal role of technology-driven, patient-centered approaches in contemporary cancer care. These approaches holistically address patients’ multifaceted challenges, encompassing physical and psychological aspects. Furthermore, the postintervention improvements in QOL from the PBSP echo the findings of Aminuddin et al. (2021) and Barham et al. (2019). They highlight the critical role of telemedicine interventions in enhancing patients’ overall well-being. The PBSP replaces conventional feedback mechanisms by offering dynamic support and engagement through a smartphone application, thus facilitating a comprehensive approach to patient care during and after cancer treatment. The application of PBSP underscores the growing body of evidence supporting telenursing interventions in cancer care, especially relevant in today's healthcare, which increasingly relies on telehealth and remote patient support systems. This relevance is amplified by the ongoing challenges of limited healthcare access and the necessity for effective, remote patient support mechanisms.
Previous research suggests a complex interplay between demographic and clinical factors in caring for women with breast cancer, highlighting the need for tailored interventions (Paranjpe et al., 2019; Stalsberg et al., 2022). Factors like age, family income, and employment status significantly impact patients’ psychological and social experiences (Mols et al., 2020), while clinical aspects, such as cancer stage and treatment type, further influence these experiences (Lovelace et al., 2019). For instance, women with advanced-stage cancer or undergoing aggressive chemotherapy regimens might experience greater psychological distress. These factors are crucial for holistic support and effective patient care delivered by the PBSP, as supported by recent literature advocating for personalized care strategies (Pashayan et al., 2020). It is vital for addressing the unique needs of women with breast cancer and enhancing treatment outcomes for overall well-being.
The PBSP not only advances SCSE, symptom management, and QOL among women with breast cancer but also serves as another example of the transformative potential of telenursing within the broader spectrum of telemedicine. Our pilot study highlights the unique role of smartphone healthcare applications in enhancing patient care across various settings. Future research should not only explore the scalability of such programs but also rigorously investigate their long-term impacts on diverse patient populations, thereby expanding the scope and reach of telenursing in global healthcare delivery.
Strengths and Limitations
While yielding promising results, this pilot study has notable limitations that must be addressed. The small sample size and the lack of a control group limit the generalizability of its findings. To overcome these constraints, subsequent studies should employ a larger and more diverse sample, incorporating a randomized controlled trial design with a comparison or control group. This approach will enhance the validity and applicability of the results.
The study's reliance on convenience sampling and its focus on a specific patient demographic may introduce selection bias, potentially affecting the representativeness of the results. Future research must expand its scope to include a broader range of patient demographics and cancer types. This expansion is essential, as managing postchemotherapy complications is a critical aspect of cancer care across different cancer types. Additionally, the long-term nature of breast cancer therapy necessitates a study design that allows for extended follow-up periods. This will ensure a more comprehensive understanding of the intervention's effectiveness over time and provide insights into the long-term impacts on patient self-efficacy and well-being.
Implications for Nursing Practice
Nurses play a crucial role in supporting women with breast cancer throughout their treatment journey. They can incorporate technology-based interventions to further enhance their ability to provide comprehensive care. Using smartphone applications, nurses can provide patients access to valuable health information, self-care strategies, and social support. The interactive nature of these applications allows for ongoing communication and guidance, even when face-to-face interactions are limited. Phone-based interventions can help empower patients, improve their self-efficacy, and ultimately improve patient outcomes and well-being. The use of the PBSP showed promise in improving SCSE, symptom distress, and QOL for women with breast cancer undergoing chemotherapy. The results of this study have important implications for nursing practice in the context of breast cancer care. Nurses can facilitate discussions, address concerns, and provide expert advice through online platforms, thus extending their reach and support beyond traditional care settings.
Conclusions
The results of the pilot research support that a technology-based intervention can enhance nursing care for women with breast cancer undergoing chemotherapy. The use of a smartphone application can facilitate the delivery of educational materials, encourage social interaction, and provide access to expert advice. The PBSP was feasible and effective for this population, as evidenced by the improved SCSE, decreased symptom distress, and improved QOL, as reported by women. Nurses can use the PBSP to augment their role in supporting patients throughout their treatment journey.
Footnotes
Acknowledgments
The authors wish to thank to all the participants who greatly contributed to this study, staff of oncology department of Yancheng No.1 People's Hospital in Jiangsu, China, and Mr. Qin Yang for their support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Burapha University (grant number N/A).