
Abstract
Background
Assessment of quality of life (QoL) in cancer patients can provide an overall picture of the patient's adaptation to the disease and maintain long-term health and well-being. Determining the QoL in cancer patients could help with better care and could be as prognostic as medical factors and the survival benefit that pharmacological treatment could provide. The main objective of this review was to determine the prevalence of QoL among Ethiopian adult cancer patients.
Methods
A systematic review was conducted using the “Preferred Reporting Results of Systematic Reviews and Meta-Analyses” guidelines. Databases such as PubMed/Medline, CINAHL, AMED, Embase, the Cochrane Library, ScienceDirect, World Health Organization's Hinari portal, and African Journals Online databases were searched from January 2022 to June 2022. Google, Google Scholar, and university repositories were used to access unpublished studies. Two reviewers independently screened the data using a standardized data extraction format and appraised their quality using the Newcastle–Ottawa Scale.
Results
In this review, 10 studies were included. The prevalence of poor QoL ranged from 52 to 89.6. The physical, role, social, and emotional functioning were the most affected domains of QoL and have been significantly associated with QoL. Financial difficulty was the most important predictor of QoL among Ethiopian cancer patients. Pain, dyspnea, nausea, vomiting, and poor appetite were also reported as predictors of QoL. Low income, lower educational status, unmarried status, underweight, anxiety, and depression, advanced stage of cancer, patients with ≤2 cycles of chemotherapy, and the presence of comorbid diseases were significantly correlated with QoL.
Conclusions
The QoL of an Ethiopian cancer patient was low. Quality of life assessments, appropriate symptom management, integration of psycho-oncology care, and providing economic support shall be considered to improve their QoL.
Introduction
Cancer is rapidly becoming a public health priority in Africa. Up to 70% of the predicted 24 million people who will be diagnosed with cancer annually by 2050 will reside in low- and middle-income countries (Parkin et al., 2020). In Ethiopia, the incident rate of cancer will increase from 7,400 to 151,000, and cancer-related mortality will increase from 51,900 to 102,000 in the year 2040 (Ferlay et al., 2020). The increasing prevalence of cancer in recent years and its effects on the various physical, psychological, and social dimensions of human life has made it the century's major health problem (Chagani et al., 2017).
“Cancer is a group of diseases characterized by the uncontrolled and unregulated growth of cells that can affect any part of the body” (Harding et al., 2019, p. 232). Despite advances in medicine, being diagnosed with cancer creates stress for the patient, and they are also prone to developing a wide range of physical, psychosocial, and financial issues, which can decrease their quality of life (QoL) (Chagani et al., 2017).
The World Health Organization (WHO) states that QoL is determined by an individual's perceptions of his or her position in life with respect to goals, interests, expectations, standards, and concerns, as well as the culture and value systems in which they live (World Health Organization Quality Of Life Group [WHOQOLG], 1995). The perception of their living status and satisfaction with life strongly influence their QoL (Alaloul et al., 2019)
The assessment of QoL among cancer patients is an important outcome measurement tool (Uwamahoro, 2017). As a result, measurement of the QoL in cancer patients is recommended in the USA and Germany (Association of Comprehensive Cancer Center, 2015; German Cancer Society [GCC], 2015). Assessing the patient's feelings while they are battling with the disease has a vast effect on their ability to carry out normal daily functions, as well as on their interpersonal relationships and their ability to live a quality life. Additionally, it has been suggested that assessing the QoL in cancer patients could aid in better care and be as prognostic as medical treatment could be; it also showed the individual's ability to manage the disease, maintain good health, and evaluate the effectiveness of interventions (Mosleh, 2018).
Nowadays, measuring QoL is common among cancer patients. Most research in Ethiopia revealed that cancer patients had poor QoL (Abegaz et al., 2018; Hassen et al., 2019; Muhamed et al., 2023). Previous research has shown that low QoL is associated with undesirable treatment outcomes, such as mental illness, that is, anxiety, depression, and hopelessness, which may gradually worsen the prognosis and increase mortality rates (Tesemma et al., 2019). The most significant contributing variables to this problem were low income, anxiety, depression, malnutrition, and an advanced stage of cancer (Abegaz et al., 2018; Hassen et al., 2019; Muhamed et al., 2023; Sibhat et al., 2019).
Works of literature about QoL among adult cancer patients urge policymakers and cancer treatment institutions to give great emphasis and take appropriate action to improve the patient's QoL. There is limited research on the importance of patient-reported QoL as the main treatment domain for cancer patients in Ethiopia. The few available studies on QoL among cancer patients have inconclusive and inconsistent results (Alem et al., 2020; Muhamed et al., 2023). Therefore, this systematic review aimed to determine the status of QoL among Ethiopian adult cancer patients.
Methods and Materials
Literature Searching Strategies
A systematic literature search was conducted to review studies that evaluate the QoL among adult cancer patients in Ethiopia. We followed the Preferred Reporting Items of Systematic Reviews and Meta-Analysis guidelines (Moher et al., 2009). Using combined keywords and subject headings, studies were systematically searched on major medical electronic databases. Databases such as PubMed/Medline, CINAHL, AMED, Embase, Cochrane Library, Science Direct, WHO's Hinari portal, and African Journals Online databases were searched to get relevant articles for this review. In addition, Google and Google Scholar were used to access grey literature. Academic institution research repositories and libraries were also used to access the thesis and dissertations. All databases were searched from January to June 2022.
All the database search results were exported to EndNote citation manager software (version X9; Thomson Reuters, New York, NY), and duplicate articles were removed. The key terms used for searching published literature were (“assessment” OR “evaluation” [MeSH terms] AND (“prevalence” OR “magnitude” OR “proportion” OR “incidence” [MeSH terms] AND ((“Health-Related Quality of Life,” OR “health-related quality of life”)), [MeSH terms] OR “QUALITY OF LIFE” OR “Quality of Life,” OR “quality of life” [MeSH terms] OR “HRQOL” OR “QOL,” [MeSH terms] AND (CANCER, OR “cancer,” [MeSH terms] “Malignant,” OR “malignant,” or “tumor,” or neoplasm, [MeSH terms] AND “Adult,” OR “adult,” [MeSH terms] AND “patient,” OR “persons,” OR “client,” OR “individuals,” OR “population,” [MeSH terms] AND “cross sectional studies,” OR “cohort studies,” OR “follow-up studies,” OR “longitudinal studies,” OR “prospective studies” AND “Ethiopia”) [MeSH terms].
Eligibility Criteria and Selection of Studies
All articles were considered for an initial review if they met the following inclusion criteria: adult cancer patients (≥18 years) and assessing QoL as the outcome of interest. The outcomes of this review is (a) the prevalence of QoL measured by QoL questionnaires, (b) domains of QoL, that is, functional scales (physical, role, emotional, cognitive, and social functioning) and symptom scales (fatigue, nausea, vomiting, pain, dyspnea, insomnia, appetite loss, constipation, diarrhea, and financial difficulties), and (c) factors that are associated with quality of life. Studies that assess QoL using European organization for research and treatment of cancer QoL questionnaire (EORTC QLQ-C30). The following exclusion criteria were used: studies conducted outside Ethiopia, with less than 10 patients, qualitative studies, validity test reports, conference abstracts, and studies that did not pass our quality screening.
Study Scope. All studies conducted in Ethiopia on QoL among adult cancer patients were published in the English language, and no restriction was applied to study design, study setting, and publication year.
Data Extraction and Quality Assessment
Data extraction was undertaken using a standardized Excel spreadsheet format using the Joanna Briggs Institute Reviewers’ Manual 2014 (Munn et al., 2018). This standardized data extraction format includes the following: author name, study area, publication year, study design, sample size, response rate, an assessment tool used to diagnose QoL, the prevalence of poor QoL, and quality assessment. The database search results were combined, and duplicate articles were manually removed using EndNote (version X9). After the removal of duplicates, titles and abstracts were screened independently by two authors (AN and BC), followed by an assessment of the full text for selected studies to determine compliance with the inclusion criteria. Any disagreements were settled through discussion until a consensus was reached. Two independent reviewers critically evaluated each paper. Disagreements between those reviewers were solved by discussion. If not, a third reviewer was involved to resolve the inconsistencies between the two independent reviewers. The average of the two independent reviewers’ scores was used to determine whether the articles should be included.
The quality assessment and risk of bias were done using the 10-item Newcastle–Ottawa Scale (NOS) criterion developed by Hoy et al. for cross-sectional studies (Moskalewicz & Oremus, 2020). Each item was given a score of one if it met the methodological criteria or zero if it did not, and the aggregate of these ratings was used to calculate the study's overall quality score. A “low risk of bias” was defined as a score of 8–10, a “moderate risk” as a score of 6–7, and a “high risk” as a score of 0–5. Articles with NOS quality scores of less than 6, methodological flaws, and incomplete reporting of results were excluded from the final analysis (Moskalewicz & Oremus, 2020).
Risk Bias Assessment
The quality score of the included study ranged from 7 to 8, with a mean score of 7.4 (SD = 0.91). Out of 10 studies, four (40%) received a low risk of bias, and six (60%) received a moderate risk of bias. The author also found a kind of bias. Five studies were at high risk of sampling and representation bias (Abegaz et al., 2018; Alem et al., 2020; Bekele, 2016; Muhamed et al., 2023; Negewe, 2016), and four studies were at high risk of random selection bias (Araya et al., 2020; Ayana et al., 2018; Bekele, 2016; Hassen et al., 2019).
Results
Characteristics of Included Studies
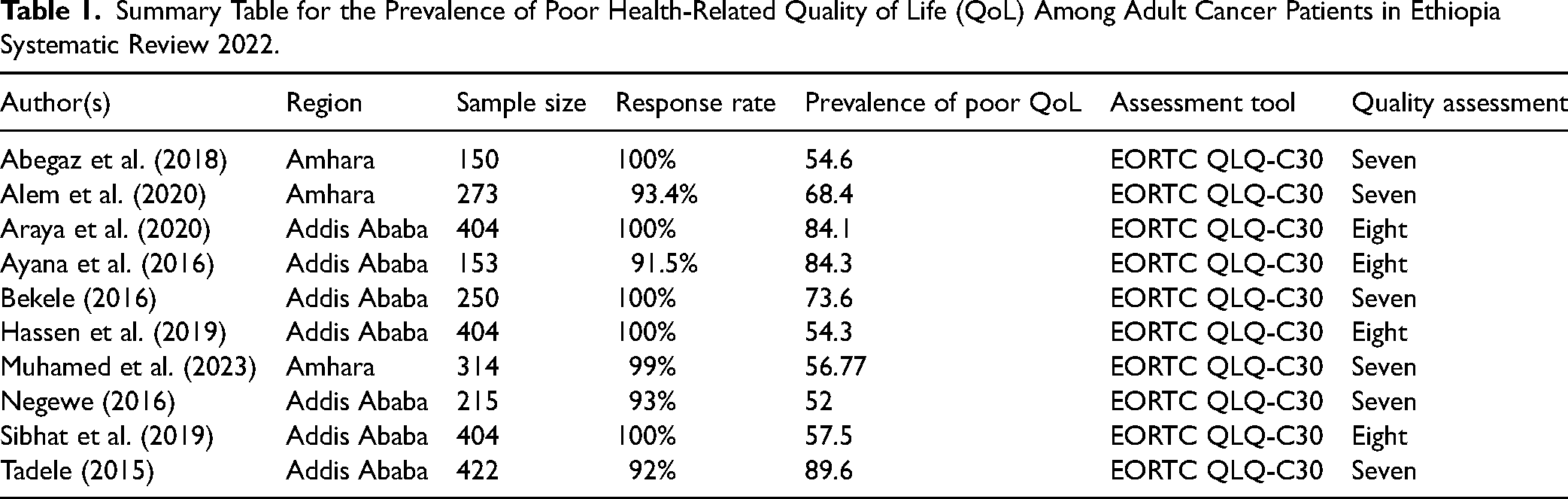
The total respondents in this review were 2,905 study participants. Of the 10 articles selected, seven were conducted in Addis Ababa (Araya et al., 2020; Ayana et al., 2018; Bekele, 2016; Hassen et al., 2019; Negewe, 2016; Sibhat et al., 2019; Tadele, 2015), and three were conducted in the Amhara region (Abegaz et al., 2018; Alem et al., 2020; Muhamed et al., 2023). See Figure 1. With regard to research design, all of the studies employed a cross-sectional quantitative study. The sample sizes ranged from 153 to 404 cancer patients. The prevalence of poor QoL and domains of QoL were reported. See Table 1 for sociodemographic and prevalence of QoL.

Preferred Reporting Results of Systematic Reviews and Meta-Analyses (PRISMA) flow diagram describes the selection of studies for a systematic review quality of life of Ethiopian cancer patients, 2022.
Summary Table for the Prevalence of Poor Health-Related Quality of Life (QoL) Among Adult Cancer Patients in Ethiopia Systematic Review 2022.
Questionnaires
All of the studies used the Amharic version of the EORTC QLQ-C30 questionnaires to assess QoL among cancer patients. The EORTC QLQ-C30 is designed for use with a wide range of cancer patients and has been translated and validated in over 100 languages, including Amharic (Scott et al., 2008). The tool was valid and reliable in Ethiopia (Ayana et al., 2016). The EORTC QLQ-C30 is the main questionnaire that is aimed at addressing the health-related QoL of cancer patients. It incorporates 30 items, among which five functional scales (physical, role, cognitive, emotional, and social functioning); three symptom scales (fatigue, pain, and nausea or vomiting); a two-item global health/QoL scale; and six single items (dyspnea, appetite loss, insomnia, constipation, diarrhea, and financial difficulties). It uses Likert-type scales, and all dimensions are summarized in a final score ranging from 0 to 100.
QoL
Studies reported that the prevalence of poor QoL among Ethiopian cancer patients ranged from 52% to 89.6% (Abegaz et al., 2018; Alem et al., 2020; Araya et al., 2020; Ayana et al., 2018; Bekele, 2016; Hassen et al., 2019; Muhamed et al., 2023; Negewe, 2016; Sibhat et al., 2019; Tadele, 2015).
Functional and Symptom Scale Scores of EORTC QLQ-C30
In the EORTC QLQ-C30, the functional scale of study participants scored a mean of 40.38 ± 30.93 in social functioning (Araya et al., 2020), 42.26 (32.08) in role functioning (Abegaz et al., 2018), 44.48 (21.29) in emotional functioning (Muhamed et al., 2023), and a mean of 80.06 ± 22.89 for cognitive functioning (Hassen et al., 2019). The most affected functional domain was emotional functioning, role, physical, and social function (Bekele, 2016; Hassen et al., 2019; Muhamed et al., 2023). Cognitive function was the least affected functional domain (Sibhat et al., 2019). Among the symptom scale and the single items, all studies reported that financial difficulties were the commonest problem in Ethiopian cancer patients (Abegaz et al., 2018; Ayana et al., 2018; Bekele, 2016; Hassen et al., 2019; Muhamed et al., 2023; Negewe, 2016; Sibhat et al., 2019; Tadele, 2015). Fatigue, appetite loss, pain, constipation, diarrhea, nausea, and vomiting were also the most frequent symptoms in cancer patients (Ayana et al., 2018; Hassen et al., 2019; Muhamed et al., 2023; Negewe, 2016).
Other Predictors of QoL
Most of the studies examined the association between QoL and sociodemographic and clinical predictors (Alem et al., 2020; Araya et al., 2020; Bekele, 2016; Hassen et al., 2019; Muhamed et al., 2023; Sibhat et al., 2019; Tadele, 2015). Low income (Bekele, 2016; Hassen et al., 2019; Sibhat et al., 2019), lower educational status (Ayana et al., 2018; Hassen et al., 2019; Muhamed et al., 2023), divorced or separated status (Alem et al., 2020; Hassen et al., 2019), underweight (Muhamed et al., 2023), anxiety (Muhamed et al., 2023), depression (Muhamed et al., 2023), advanced stage of cancer, patients with ≤2 cycles of chemotherapy, and the presence of comorbid diseases were significantly correlated with poor QoL (Hassen et al., 2019; Muhamed et al., 2023).
Discussion
To our knowledge, for the first time, the current study has reviewed the results of 10 kinds of research examining the QoL among Ethiopian cancer patients. Quality of life refers to global well-being, including physical, role, emotional, social, and cognitive components. Today, globally, QoL gets great attention in cancer research and is considered an important patient-reported measurement. This systematic review is very necessary to know the status of the QoL of adult cancer patients and associated factors in a resource-constrained context in Ethiopia.
The findings of this review showed that cancer patients have a poor QoL. This review was consistent with a study in Rwanda and Tanzania (Masika et al., 2012; Uwamahoro, 2017). However, the result of this study is contrary to studies conducted in Iran, Turkey, and India (Abdollahzadeh et al., 2012; Arslan et al., 2013; Ramasubbu et al., 2020). Therefore, the reason for poor QoL in the Ethiopian studies might be that the treatment protocol is focused on disease management and gives less attention to the psychosocial dimension of the patient's life (Hassen et al., 2019; Muhamed et al., 2023); the quality of care provided in the setup (Abegaz et al., 2018); chemotherapy is expensive, and many patients struggle to buy the drug (Bekele, 2016; Hassen et al., 2019; Negewe, 2016); stigma related to cancer diagnosis; and less symptom management (Hassen et al., 2019; Muhamed et al., 2023; Negewe, 2016).
In the functional domain of EOCRTS, most of the studies reported that the physical, social, role, and emotional aspects of the patient's life were affected, and they are associated with poor QoL (Bekele, 2016; Muhamed et al., 2023; Tadele, 2015). The findings of this study were lower compared to studies conducted in India (Ramasubbu et al., 2020), Turkey (Ustundag & Zencirci, 2015), Nepal (Pandey et al., 2015), Jordan (Mosleh, 2018), and Brazil (Mansano-Schlosser & Ceolim, 2012). Poor social and role functioning might be due to the fact that most cancer patients in the hospital have advanced cancer stages, which can hinder their functioning in different social activities.
Two studies indicated that cognitive functioning is also one of the QoL predictors and showed a significant mean difference between cognitive functioning and QoL (Bekele, 2016; Sibhat et al., 2019), which is in line with a study conducted in Turkey (Sahin & Tan, 2012). The cognitive functioning of patients could be compromised due to chemotherapy, pain, and the burden of diseases (Bekele, 2016; Sibhat et al., 2019).
Financial difficulty was the most common problem among Ethiopian cancer patients (Hassen et al., 2019; Muhamed et al., 2023; Negewe, 2016; Sibhat et al., 2019). This is consistent with Rwanda, Tanzania, and Jordan (Masika et al., 2012; Mosleh, 2018; Uwamahoro, 2017). This showed that the financial burden of cancer patients in Ethiopia is considerably high because chemotherapy is a prolonged and expensive treatment that creates a financial burden among cancer patients. There is also less coverage of health insurance in the Ethiopian settings, and since the study participants are adult populations, the impairment in functional status has an effect on the economic condition of the family (Muhamed et al., 2023).
The studies showed a higher number of symptoms among cancer patients in Ethiopia. Pain (Tadele, 2015; Wondie & Hinz, 2020), dyspnea (Negewe, 2016), fatigue, and appetite loss (Muhamed et al., 2023; Negewe, 2016) were associated with QoL and affected their ability to take care of themselves and their families. These findings are also consistent with studies done in Nepal, Sweden, and Rwanda (Hinz et al., 2014; Pandey et al., 2015; Uwamahoro, 2017). Studies indicated that symptoms experienced by cancer patients influence the continuation of treatment and affect their QoL (Hassen et al., 2019; Tesemma et al., 2019). A study in Turkey reported that cancer patients suffered from a variety of symptoms such as fatigue and pain during their treatment, which had an impact on their daily lives and QoL (Arslan et al., 2013). Studies revealed that malignancy by itself could induce malaise and weakness. It has resulted from the therapy, including radiotherapy and chemotherapy, as well as the disease state. Consequently, the QoL of patients is reduced as fatigue becomes severe (Ayana et al., 2018; Negewe, 2016). A high number of symptoms in this review could be explained by the advanced stage of cancer diagnosis and poor symptom management (Araya et al., 2020; Muhamed et al., 2023; Negewe, 2016).
Nausea and vomiting are also other symptoms that show an association with poor QoL (Abegaz et al., 2018; Negewe, 2016). The side effects of chemotherapies, underutilization of antiemetics due to fewer prescriptions, and nonadherence to the treatment might contribute to the high prevalence of waves of nausea and vomiting (Tadele, 2015).
Limitation
This study has some limitations. First, the studies were reviewed from two administrative regions of Ethiopia, which may underrepresent the rest of the country. Second, all of the included studies were cross-sectional study designs, in which the result might be affected by confounding variables, which hinders the possibility of assessing for cause-and-effect relationships.
Implications for Practice
According to this review, Ethiopian cancer patients have a poor QoL, and identification of those predictor factors would permit the Ministry of Health and nongovernmental organizations to design appropriate management strategies that can be important in improving the QoL of cancer patients. The review indicated that the QoL of Ethiopian cancer patients was mainly affected by financial difficulty, symptoms, and psychosocial status. Hence, this finding emphasizes the need for financial support, proper symptom management, and psychosocial care to improve the patient's QoL.
Conclusions
The findings of this review showed that cancer patients had a lower QoL. The findings also indicated that poor physical, role, social, and emotional functioning was associated with poor QoL. From the symptoms and single items, financial difficulty was the leading predictor of poor QoL among Ethiopian cancer patients. Symptoms such as pain, dyspnea, loss of appetite, nausea, and vomiting are also associated with poor QoL. The findings in this review suggest that healthcare workers should understand the potential impact of QoL on cancer patients and take this into consideration in the care of these individuals. Therefore, financial support, psychosocial support, and symptom management should be important components of care for a cancer patient.
Footnotes
Acknowledgments
The authors would like to thank Wolkite University for providing an available online database.
Authors’ Contribution
AN proposed the initial concept idea, conceived, and designed the systematic review protocol. AN, FE, and BC designed search strategies. BF, BB, AM, and GD performed the study selection, data extraction, and study quality assessment. AN, BB, and AM wrote the first draft of the manuscript. All authors discussed and revised the manuscript. All authors read and accepted the final version and agree to be accountable for all aspects of the work.
Authors’ Note
Data will be made available by request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.