
Abstract
The phenomenon of workplace violence (WPV) is prevalent in clinical settings affecting nurses and nursing students. Mental health nursing simulations may be used to impart knowledge and skills to nursing students to manage and prevent incidents of WPV. This article presents attained competency skills by nursing students after attending a simulation, and how they implemented their knowledge learned in their clinical rotations. Students attended a Mental Health Nursing Simulation on WPV and completed surveys. The simulation enhanced the students' communication skills, empathy, ability to manage verbally aggressive patients, ability to set personal boundaries, and ability to seek support from others. Participants reported physical and verbal forms of WPV and application of learned evidence-based skills in their clinical rotations. Evidence-based skills to manage and prevent WPV taught to nursing students via mental health nursing simulations can enhance their clinical competency, and they should be embedded in a nursing curriculum.
Keywords
Introduction
Workplace violence (WPV) may be defined as “any physical or verbal assault toward a person in a work environment” (Occupational Safety and Health Administration [OSHA], 2015, p. 1). Health-care workers around the world have a significant risk of being exposed to WPV (World Health Organization [WHO], 2018). The WPV phenomenon is prevalent in various nursing clinical settings (Edward et al., 2016). A recent review of the literature highlighted the fact that nurses and nursing students are vulnerable to experience incidents of WPV in clinical settings (Hopkins, Fetherston, & Morrison, 2018). Training initiatives to properly address the phenomenon of WPV are supported by national and global organizations (OSHA, 2015; WHO, 2018). Researchers suggest that training programs should be developed for nurses and nursing students to prevent and manage aggressive and challenging situations (Edward et al., 2016; Hopkins et al., 2018). To address this gap in nursing education, nursing simulations are innovative teaching modalities faculty could use to supplement new knowledge and skills to nursing students to combat incidents of WPV.
Nursing simulations have been broadly used in nursing education; however, the utilization of simulations in mental health nursing courses is limited (Felton & Wright, 2017). There is a need for nurse educators to design and impart realistic educational pedagogies to ensure that students have adequate learning experiences that will allow them to provide competent patient care (Kunst, Mitchel, & Johnson, 2017). Evidence-based knowledge and skills aiming to manage and prevent incidents of WPV imparted via simulations have the potential to enhance a mental health nursing curriculum. Recent research in mental health nursing simulations has been focused on assessing the students' confidence, knowledge, and communication skills following a simulation (Doolen, Giddings, Johnson, De Nathan, & Badia, 2014). There is limited research showing how nursing students apply the knowledge and skills learned in simulations in clinical settings (Kunst et al., 2017); therefore, the assessment of the students' performance in their clinical practicum can enhance the value of simulations (Choi, 2012).
This article presents a secondary data analysis that demonstrates competency skills attained by prelicensure students who participated in Martinez's (2017) study. Martinez (2017) developed a Mental Health Nursing Simulation on WPV employing a standardized patient (SP) who behaved as an agitated patient with mental illness. Martinez's (2017) study aims were to improve the participants' knowledge on WPV, develop their ability to assess for signs of aggression, provide an experiential learning experience for them to employ evidence-based interventions to de-escalate the SP's behavior, and assess their views and perceptions about their learning experience. In addition, this article provides new evidence about how the students' knowledge and skills acquired during the simulation were employed in their mental health nursing clinical rotation in subsequent weeks after their simulation experience.
Review of the Evidence
Simulations in Nursing Education
Simulations have become a common training modality in nursing education courses (Goh, Selvarajan, Chng, Tan, & Yobas, 2016). Simulations can be used in combination with clinical experiences allowing new knowledge and skills to be introduced for the students (Choi, 2012; Schwindt & McNelis, 2015). In certain situations where psychiatric clinical placements are scarce, simulations may help facilitate the students' completion of required clinical hours (Doolen et al., 2014). In regards of preparation for clinical practice and acceptance of nursing simulations as an innovative teaching modality, Alexander and Dearsley (2013) reported that 62.5% of the students who participated in a nursing simulation with SPs stated it was beneficial for their clinical practice. Doolen et al. (2014) stated that 95.75% of the students who participated in simulation with SPs reported that it prepared them for the mental health clinical environment, and 100% of the respondents stated the scenarios were useful.
Simulations in Mental Health Nursing Using SPs
The use of SPs in mental health simulations can facilitate application of psychiatric concepts. Patient simulation can help facilitate clinical application. The SP is an individual who has been coached to portray the role of a patient portraying a particular clinical problem in a realistic manner (Alexander & Dearsley, 2013; Oh, Jeon, & Ko, 2015). The SP can be trained by the facilitator to perform specific behaviors, emulate a patient interaction in a controlled environment, and provide a brief feedback to the participants (Doolen et al., 2014).
The field of mental health nursing may challenge nursing students because patients suffering of mental illnesses can exhibit unpredictable behaviors requiring prompt nursing interventions and expertise to deliver sophisticated patient care (Alexander & Dearsley, 2013; Kunst et al., 2017). At times, students may experience anxiety and apprehension when interacting with psychiatric patients (Choi, 2012). Appropriate preparation prior to their clinical experience can help enhance the students' competency skills to care for these patients. Recent research studies have reported that using SPs during mental health nursing simulations may enhance students' confidence (Alexander & Dearley, 2013; Goh et al., 2016), promote anxiety reduction prior to real patient encounters (Doolen et al., 2014; Kameg, Szpak, Cline, & Mcdermott, 2014), and help prepare students prior to their mental health nursing clinical rotation (Doolen et al., 2014). Mental health simulations with SPs can provide the students the ability to practice nurse–patient scenarios prior to real patient encounters in psychiatric settings in a safe learning environment.
Methods
Design
Martinez's (2017) mental health nursing simulation had a qualitative descriptive and quantitative design. According to Lambert and Lambert (2012), using qualitative descriptive design in a study provides a summary of the data collected in an organized manner. This method was chosen to represent the students' responses collected from the weekly surveys postsimulation. The simulation consisted of a single-group pre- and posttest design. This type of quantitative design is commonly used in nursing research (Spurlock, 2018), and it was selected to assess the students' learning outcomes after participating in the simulation.
Theoretical Framework
Kolb's (1984) experiential learning theory guided Martinez's (2017) simulation. The theory points out that assimilation of knowledge can be attained by practicing the learned skills (Kolb, 1984). The realistic experience portrayed by the SP during the simulation encounters can facilitate the students' learning while employing the different components of Kolb (1984) theory.
Instruments
The mental health nursing clinical confidence scale (MHNCCS) developed by Bell, Horsfall, and Goodin (1998) was employed by Martinez (2017) to measure participants' confidence pre- and postsimulation. The MHNCCS contains 20 items ranging from Number 1 meaning confident to Number 4 meaning completely confident (Bell et al., 1998). The authors indicated that the MHNCCS can be used to assess nursing students' confidence levels and a Cronbach's alpha result of .926 demonstrating the scale's reliability (Bell et al., 1998). Permission to use the scale was granted via e-mail by the main author.
In addition, Martinez (2017) developed a questionnaire to be completed by the students every week for 4 weeks after participating in the simulation. The questionnaire was delivered via e-mail using the software program Qualtrics©. The questionnaire aimed to assess how the participants employed their evidence-based knowledge and skills learned in the simulation and their ability to assess incidents of WPV in their respective clinical rotation sites (see online Appendix A).
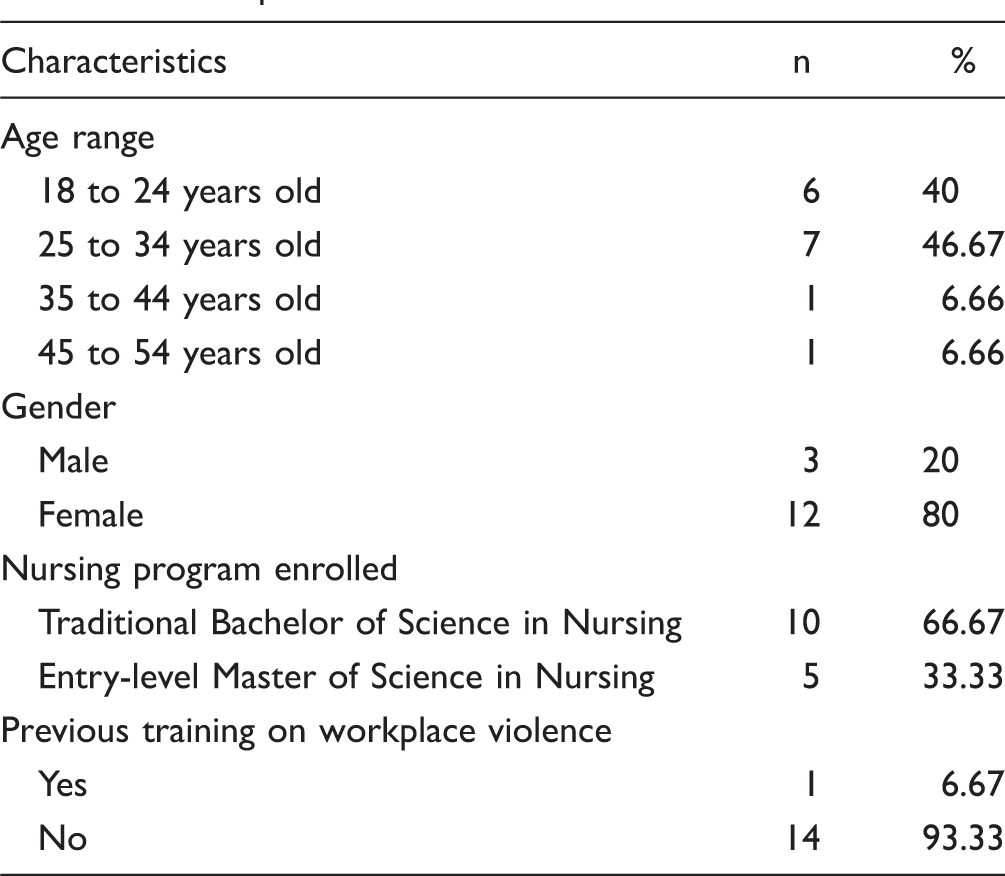
Participants
Participants Characteristics.
Ethical Considerations
Institutional review board exemption was secured from the university to conduct the study at the university's school of nursing simulation laboratory (Martinez, 2017). A consent for the participants was written by Martinez (2017) following the university's guidelines, and they voluntarily signed the consent and also had opportunities to ask questions and raise concerns about the study. All the participants were informed that their participation was strictly voluntary, would not influence their grade in the clinical course, and they also had the opportunity to abstain from attending the simulation (Martinez, 2017).
Procedure
Martinez (2017) reported that on the simulation day, the participants were divided in seven pairs, and one participant completed the encounter unaccompanied. This decision was made based on the logistics and scheduling of the simulation room which was limited to 2 hours. One week prior to the simulation, each participant had received handouts containing evidence-based interventions they could implement during their encounter (Martinez, 2017). Martinez (2017) stated that the participants watched a PowerPoint presentation about WPV highlighting the various forms of WPV that could be found in clinical settings, how WPV affects the nursing workforce, and evidence-based interventions suggested by Price and Baker (2012) to manage this phenomenon. Among those interventions provided to the participants included therapeutic communication skills such as active listening, being aware of verbal and nonverbal forms of communication, engaging the patient, maintaining personal control such as controlling one's own anxiety, remaining calm, offering alternatives, and maintaining personal space (Price & Baker, 2012).
Every encounter was timed to 5 minutes and was video recorded, and the participants received a 2-minute debriefing session provided by the SP after every encounter (Martinez, 2017). The facilitator decided this time to be sufficient after several trials between the SP and the facilitator, and also to minimize any potential distress that could have been experienced by the participants with a longer simulation session. The debriefing session with the facilitator included playing each of the recorded encounters where an open dialogue among all participants occurred, and verbal feedback was provided to all the participants by the facilitator (Martinez, 2017).
Participants were asked to complete the MHNCCS before and after the simulation. The MHNCCS was used to assess the participants' competency skills learned in the simulation. Participants' competence skills included employing therapeutic approaches to de-escalate patients, therapeutic communication skills, verbal de-escalation skills, safety techniques, and recognizing and assessing signs of aggression (Martinez, 2017).
The students' application of knowledge learned in the simulation in their clinical settings was assessed from the weekly open-ended questionnaire developed by the facilitator (see online Appendix A). This particular questionnaire was sent to the participants via e-mail using Qualtrics© software over a period of 4 weeks following their simulation experience. This was determined by the facilitator in consideration of the students' academic demands during that semester. Responses from the participants were stored and kept confidential by the facilitator in a password-protected computer. To protect the participants' confidentiality reporting incidents of WPV, no identifying information was collected from the weekly surveys. Also, the patients' confidentiality was maintained because no demographic, medical or psychiatric history, racial, gender, or any type of identifying information from the patients from both clinical settings was obtained.
Data Analysis
Qualitative and quantitative data were obtained from all the participants' responses. Quantitative data from the MHNCCS were statistically analyzed using the SPSS software version 24. Responses from the weekly questionnaires were read, tabulated, and summarized by the facilitator.
Qualitative and Quantitative Data From the Participants' Reports
Number of Verbal and Physical WPV Incidents Reported by the Participants.

Note. WPV = Workplace violence.
Examples of WPV Incidents Reported by the Participants.
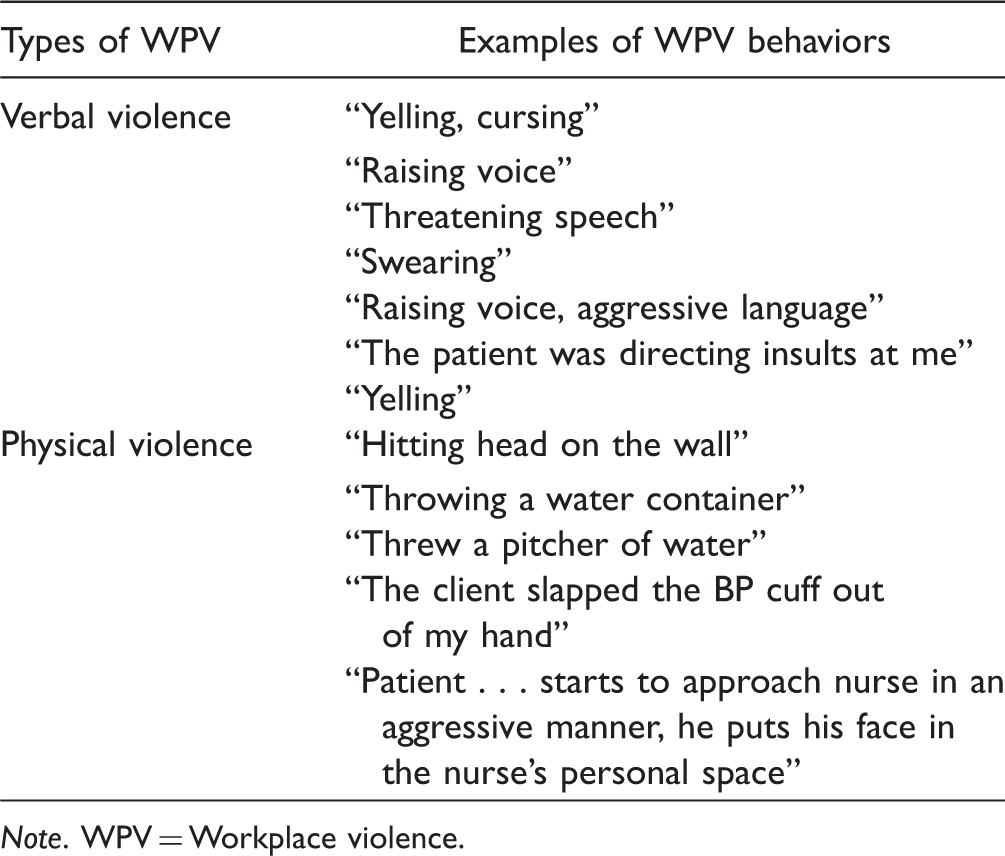
Note. WPV = Workplace violence.
Participants' Application of Knowledge Into Practice to Manage WPV Incidents.

Note. WPV = Workplace violence.
Quantitative Results From the Simulation
Pre- and Postresponse Percentages of Each Item of the Mental Health Nursing Clinical Confidence Scale.
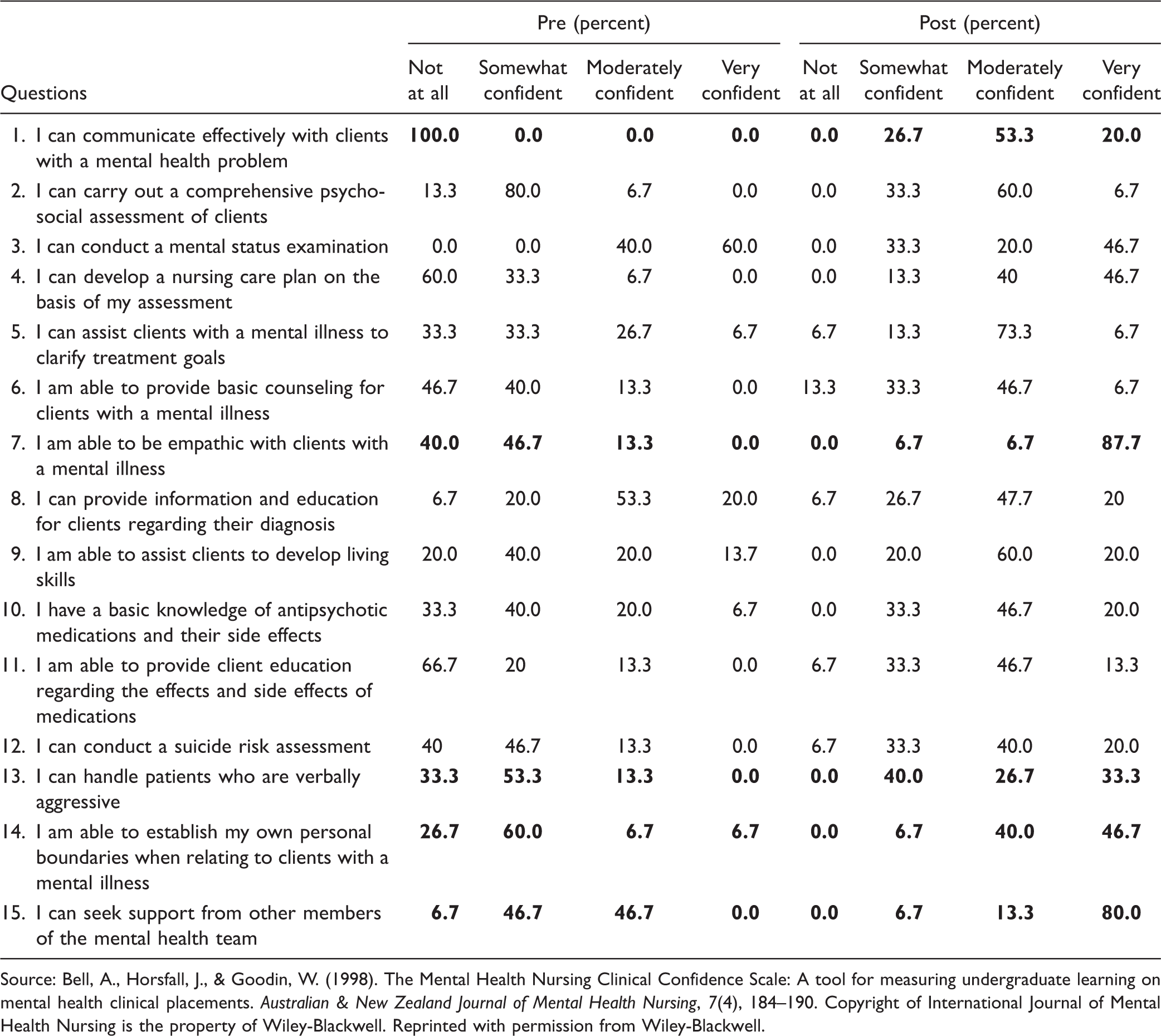
Source: Bell, A., Horsfall, J., & Goodin, W. (1998). The Mental Health Nursing Clinical Confidence Scale: A tool for measuring undergraduate learning on mental health clinical placements. Australian & New Zealand Journal of Mental Health Nursing, 7(4), 184–190. Copyright of International Journal of Mental Health Nursing is the property of Wiley-Blackwell. Reprinted with permission from Wiley-Blackwell.
Change in Pre- and Postresponses to Each Mental Health Nursing Clinical Confidence Scale Questions.

Source: Bell, A., Horsfall, J., & Goodin, W. (1998). The Mental Health Nursing Clinical Confidence Scale: A tool for measuring undergraduate learning on mental health clinical placements. Australian & New Zealand Journal of Mental Health Nursing, 7(4), 184–190. Copyright of International Journal of Mental Health Nursing is the property of Wiley-Blackwell. Reprinted with permission from Wiley-Blackwell.
Discussion
The quantitative data obtained from the participants' responses demonstrated the effectiveness of the simulation in achieving the desired study's outcomes. The uniqueness of the SP's agitated behaviors exhibited during the simulation created a realistic scenario that enhanced the participants' educational experience. The controlled environment and the scenario provided a unique opportunity for the participants to apply evidence-based skills to manage the SP's agitated behaviors and establish boundaries with the SP. In concordance with previous simulations (Alexander & Dearsley, 2013; Choi, 2012; Doolen et al., 2014), an enhancement in the participants' communication skills was obtained. The students' ability to seek support from other team members was also enhanced showing the value of teamwork. An increase in students' empathy toward psychiatric patients was also attained after the simulation. This added educational benefit may potentially contribute to the reduction of the stigma that some students may have toward patients with mental illness. This result is consistent with the research by Alexander, Sheen, Rinehart, Hay, and Boyd (2017) whose study demonstrated that simulations have the potential to shape students' attitudes toward psychiatric patients.
The participants' qualitative and quantitative responses from the weekly questionnaire demonstrated the prevalence and exposure of WPV that the participants encountered in their clinical rotations. Their responses reflected their ability to recognize verbal and physical forms of WPV in their clinical rotations. Prompt recognition of agitated behaviors can be useful to de-escalate incidents of WPV. Less than half of the participants reported that they were able to apply verbal de-escalation and other evidence-based interventions to manage patients' agitated behaviors reflecting how knowledge was translated into practice. This could have occurred because the students being exposed to WPV incidents may not have directly intervened to manage those incidents. Their application of the skills learned showed the value of having the students practice these skills in a controlled setting before their mental health clinical rotations. The participants were assigned to two different clinical settings that added the possibility of encountering differences in patient populations as well as the acuity of psychiatric symptoms exhibited by the patients. Students encountered more incidents of verbal and physical violence on one clinical site compared with the other students placed in a different clinical site. A possible explanation of this difference might be due to many factors impacting prevalence of incidents of WPV in clinical settings such as census, types of patients, and acuity of the unit. Regardless of the participants' clinical site, there was a prevalence of WPV concurring with the findings of Edward, Ousey, Warelow, and Lui (2014) who pointed out that the prevalence of WPV is high in psychiatric units, emergency rooms, and nursing homes.
Limitations
This study had several limitations. Martinez (2017) reported that he was the psychiatric clinical instructor assigned to seven participants; therefore, there could have been an increase in biases from those participants' subjective responses. Most students completed the simulation in pairs; this may have influenced the participants' ability to fully engage with the SP. Future simulations may address this by having all the participants complete their simulation experience alone. Assessment of the students' application of evidence-based interventions in their clinical rotations was limited. A semester-long follow-up is strongly suggested.
Because the simulation was conducted in only one nursing school in an urban location, with a small sample size (N = 15), the generalization of the results is limited (Martinez, 2017). As a result, it is recommended to evaluate these findings with caution. A larger sample and implementation of Martinez's (2017) simulation in other nursing schools is strongly suggested to increase the validation, transferability, and generalizability of the findings obtained.
Also, it is possible that some students may not have included all the incidents of WPV they encountered in their clinical settings due to the fact that they may have completed their surveys outside their clinical hours. The participants' race and ethnicity were not assessed; therefore, it is difficult to assess if the training program can be transferred to other student body populations abroad. Future studies on nursing simulations should attempt to have an equal balance in participants' ethnicity, race, gender, and cultural backgrounds section to compare and contrast the results among participants to enhance the transferability and generalizability of the results to other nursing students.
Implications for Nursing Education
Nurse educators must ensure students' safety prior to their clinical rotations. Embedding evidence-based content on management and prevention of WPV in nursing curricula via simulations is strongly suggested for nurse educators. This may provide several benefits to nursing students such as boosting the students' confidence, therapeutic communication skills, and recognition of signs of aggression exhibited by patients to manage those incidents during their mental health clinical rotation. A WPV simulation training program could be a viable teaching methodology that could enhance the students' preparation to manage and prevent incidents of WPV in various clinical settings during their school training. The development, implementation, and analysis of new mental health simulations using SPs may include scenarios portraying agitated patients with different psychiatric diagnoses.
Implications for Nursing Research
The increased use and acceptance of simulations in nursing schools provides nurse researchers opportunities to develop and implement new mental health nursing simulations focusing on the prevention and management of WPV. Researchers could further study the effects that simulations may have in the students' learning domains. Nurse researchers can further explore the students' perceptions about the effectiveness of experiential learning experience using SPs in mental health simulations. Nurse researchers could use a control group and also conduct randomized controlled trials to assess the effectiveness of the simulation experience. The students' application of their knowledge learned is translated and applied during their clinical rotations should be further examined in future mental health nursing simulations.
Implications for Nursing Practice
In regards of nursing practice, simulation-based training programs on management and prevention of WPV can be integrated as part of the nurses' competency programs, especially those working in nursing clinical settings with the highest incidence of WPV incidents. The realism added with the use of an SP can be beneficial for nurses who want to learn and practice evidence-based skills aiming to de-escalate agitated behaviors in a controlled learning environment. Further assessment about the efficacy of WPV training programs in reducing incidents of WPV in clinical settings is strongly suggested.
Nurse managers and hospital administrators should develop and implement hospital-based policies and procedures on management and prevention of WPV. Reporting systems must be readily available for nurses to facilitate the reporting process of incidents of WPV. The reporting system could be embedded as part of the hospital's electronic systems in place to aid in the proper documentation and follow-up about WPV incidents. Proper support for affected nurse victims of WPV should be made available including but not limited to medical care, counseling, managerial support, peer support, and so forth.
Conclusion
The participants application of evidence-based skills learned during the simulation scenario were in line with Kolb's (1984) experiential learning theory (Martinez, 2017). Findings obtained from Martinez's (2017) simulation illustrate how an evidence-based mental health nursing simulation can augment nursing students' clinical competence to manage the phenomenon of WPV. The students' application of the learned evidence-based skills in their respective clinical settings provided evidence about how knowledge was translated into practice. This simulation helped bridge the gap in nursing education by addressing some of the recommendations highlighted by Hopkins et al. (2018) and Edward et al. (2016). The educational benefits that students acquired after participating in Martinez's (2017) study could be useful across all clinical nursing rotations and in their future nursing career.
It is important to note that the findings obtained may contribute to the efforts of reducing incidents of WPV in clinical settings. Management and prevention of WPV should be taught in nursing schools because WPV can impact nursing students across educational levels. Given that there may not be any mandated guidelines across nursing schools to implement a training program on management and prevention of WPV, this author strongly recommends the development and integration of training programs for nursing students with didactic content and hands-on experiences on management and prevention of WPV in graduate and undergraduate nursing curricula.
Footnotes
Author’s Note
Adapted from Martinez, A. S. (2017). Implementing a Workplace Violence Simulation for Undergraduate Nursing Students A Pilot Study. Journal of Psychosocial Nursing & Mental Health Services, 55(10), 39–44.
Acknowledgments
The author would like to thank all the staff members involved in the implementation of the simulation, Dr. Yarandi for his guidance in the statistical analyses, and Dr. De Oliveira for guidance in the development of article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this article was made possible (in part) by Grant Number 1H79SM080386-01. The views expressed in written training materials or publications and by speakers and moderators do not necessarily reflect the official policies of the Department of Health and Human Services; nor does mention of trade names, commercial practices, or organizations imply endorsement by the U.S. government.