
Abstract
Introduction
Currently, patient safety and quality of care have become a public health concern. However, medication administration errors are common in global medical settings and may cause problems ranging from the subtle to the fatal.
Objective
To assess the Magnitude and determinant factors of Medication Administration Errors among nurses working in the public hospitals in the Eastern Amhara region, Northeastern Ethiopia, 2022.
Methods
A multicenter hospital-based cross-sectional study design was used in South Wollo Zone public hospitals from February–March 2022, with 423 nurses selected using a simple random method. Data were collected using a pretested questionnaire, entered, and analyzed using EpiData 4.6.0 and SPSS 26. Predictors of medication administration errors were identified by multivariate logistic regression.
Result
Magnitude of Medication Administration Errors in the study areas was 229 (55%), 95% CI [0.501, 0.599]. Service provision to ≥ 11 patients per day (AOR: 2.52, 95% CI [1.187, 6.78]), interruption (AOR: 4.943, 95% CI [2.088, 11.712]), lack of training (AOR: 6.35, 95% CI [3.340, 7.053]), ≥ 4 years and 5–9 years of experience respectively (AOR: 3.802, 95% CI [1.343, 10.763]), (AOR: 2.804, 95% CI [1.062, 7.424]) were factors associated with Medication Error. likewise, shortage of time (AOR: 5.637, 95% CI [2.575, 12.337]), lack of guidelines (AOR: 2.418, 95% CI [1.556, 5.086]), workload (AOR: 7.32, 95% CI [3.146, 17.032]) and stress (AOR: 12.061, 95% CI [33.624, 53.737]) were determinant factors for Medication Administration Errors.
Conclusion and recommendation
In the current study, medication administration errors were common. Patient load, interruption, nurse's service experience, time deficit, stress, a lack of training, and the absence of guidelines were associated with medication administration errors. Therefore, ongoing training, the availability of guidelines, the presence of a good working environment, and the retention of experienced nurses can all be critical steps in improving patient safety.
Keywords
Introduction
Patient safety has long been a major concern for healthcare organizations around the world, including medication errors (WHO, 2019). The National Coordinating Council for Medication Error Reporting and Prevention (NCCMER) defines a medication error (ME) as any easily preventable error that may lead to or result in inappropriate drug utilization or potentially harm a client's health if chosen to be taken by them or on the order of healthcare workers (Cousins et al., 2008).
Numerous researchers have recognized that “to err is human” and that medication errors in medical practice are inevitable (Stelfox et al., 2006). Medication errors could be categorized in a variety of ways based on several parameters, with the most common being prescription, dispensing, administration, and monitoring (WHO, 2019).
Worldwide, an estimated half a billion (421 million) people have been admitted to hospitals due to iatrogenic causes, with the majority of these admissions occurring in low- and middle-income regions (Mattingly, 2017). Medication errors affect one out of every ten inpatients, based on a study of 26 underdeveloped and developing countries, and nearly half of all hospitalization causes are totally preventable (Mattingly, 2017). In the same study, incorrect medication administration accounts for 8% of adverse drug effects, 30% of which are potentially fatal, and up to 83% of avoidable adverse drug effects (Mattingly, 2017).
Generally, drug use can have no effect or cause subtle problems, as well as severe complications, long-term trauma, prolonged hospitalization, and end-of-life and economic damage (De Vries et al., 2008). Medical error is the leading cause of major health issues worldwide (Makary et al., 2016), with 134 million adverse drug effects reported in hospitals in middle- and low-income countries each year, resulting in 2.6 million deaths (National Academies of Sciences, Engineering and Medicine, 2018). As a result, avoiding preventable medication errors could save nearly 21 billion dollars and the lives of 7 million patients worldwide (Priorities Partnership, 2019).
Medication administration is a daily part of nursing practice, accounting for nearly 40% of nursing working hours. Nurses are the healthcare professionals most accountable for drug administration errors (Cloete, 2015; Schmidt, 2003).
The World Health Organization (WHO) has been doing everything possible to reduce at least 50% of the serious but avoidable harm caused by medication errors within a 5-year period (2017–2022; WHO Global Patient Safety Challenge on Medication Safety, 2017).
Medication errors are likely to be common in developing and middle-income countries, particularly in African countries such as Ethiopia, which has a scarcity of professionals and less experience with electronic-based medical prescription, documentation, or administration (WHO Global Patient Safety Challenge on Medication Safety, 2017). However, their magnitude has not been thoroughly investigated, particularly in the study area, and previous studies were out-of-date, single-centered, and limited to referral and tertiary hospitals. As a result, this helps hospital and nursing managers consider factors of medication error and, ultimately, enhance the quality of care.
Literature Review
Globally, according to a 2018 National Academy of Sciences report, the greatest (84.7%) rate of MEs happens during medication administration, accompanied by a phase of subsequent clinical supervision at 6.2% (National Academies of Sciences, Engineering and Medicine, 2018).
According to a study conducted in two Dutch university hospitals, the overall prevalence of MAEs was 13.7%, with the three most frequently observed errors being failure of drug provision or omission (22.9%), erroneous handling (19.7%), and dosing error (19.2%; Jessurun et al., 2022). And also, the prevalence of MEAs was 28.3% in Jordan (Alrabadi et al., 2020) and 30.5% in Malaysia (Shitu et al., 2020). Besides, findings from Jordan University Hospital's pediatric unit show that the magnitude of MAE was 26.5% (Abu Farha et al., 2018). Furthermore, a study conducted in two countries in Europe (England and Wales) from 2007 through 2016 indicates that 66.4% of MAEs have been made in hospital units, of which 31.4% were related to omission errors (Härkänen et al., 2019).
According to a systematic review, 15.22%–88.6% of MAEs occurred in Southeast Asia, with the most common types of MAEs being wrong-time drug provision, failure to give medication, and provision of medication with the incorrect dose (Salmasi et al., 2015).
A study carried out in Nigeria found that 66% of nurses made errors during their clinical careers, and the administration of overdosed medications accounted for about 30% of the errors they committed (Ojerinde et al., 2014). Further, a study done in East Africa, Uganda, in Mbara Hospital shows that among all cancer patients receiving chemotherapy, 47.4% of patients have received the wrong chemotherapy drugs, which means 42.31%, 37.18%, and 20.51% of all the anti-carcinoma medicines have had some kind of error made anytime during the prescription, provision, transcription, and/or dispensing stages, respectively (Dorothy et al., 2021).
According to a meta-analysis and systematic review conducted in Ethiopia, the magnitude of MAE attributed to nurses was found to be 39.3% (Bifftu et al., 2020). Besides, it was noted in Tigray that the magnitude of MAE committed by nurses in public hospitals throughout the region was 62.7%, with miscalculated doses of certain drugs being the most common type of error (Baraki, 2018). A similar study done in three hospitals located in Ethiopia's capital city, Addis Ababa, shows that the magnitude of MAE made by nurses over a one-year span of time was 68.1% (Wondmieneh et al., 2020). Furthermore, studies conducted at the University of Gondar Teaching Hospital, Jimma University Specialized Hospital, and Felegehiwot Specialized Hospital discovered that the magnitude of MAE was 29.1%, 51.8%, and 56.4% (Bifftu et al., 2016; Feyissa et al., 2020; Felike et al., 2015), respectively. Another observational study conducted in three public hospitals, namely Gondar Specialized Hospital, Felegehiwot Specialized Hospital, and Debre-Markos Hospital, located in the northwest part of Amhara, Ethiopia, indicates that 54% of nurses working in the mentioned hospitals made MAEs over a one-year period (Mekonen et al., 2020). Furthermore, findings from five referral hospitals located in the Amhara region of Ethiopia identified the overall MAE rate as 57.7% and the three most common forms of mistakes done at the hands of nurses that lead to drug administration errors as 38.6%, 27.5%, and 26.1% due to ill-timed drug administration, misdiagnosis, and wrong evaluation, respectively (Tsegaye et al., 2020).
Many studies have identified a variety of factors associated with medication administration errors, including but not limited to professional factors, setup or organizational factors, and managerial factors (Dorothy et al., 2021; N. Priorities Partnership, 2019; Cloete 2015; Conceptual Framework for Patient Safety, 2009; Björkstén et al., 2016). Therefore, this study aimed to assess the magnitude of medication administration errors and its associated factors among nurses working in public hospitals in the south Wollo zone, northeastern Ethiopia.
Methods and Materials
Study Area and Period
The study was conducted in the South Wollo Zone in northeastern Ethiopia from February 2022 to March 2022. It is one of the administrative zones of the eastern Amhara region, with Dessie as its capital, and covers an area of approximately 1,872,611 square kilometers. It is surrounded by North Shewa and Oromia Region on the south, East Gojjam on the west, North Wollo on the north, and Oromia Zone on the east. According to the Central Statistical Agency of Ethiopia's (CSA) 2007 Census, this zone has a total population of 2,518,862, up 18.60% from the 1994 Census, of which 1,248,698 are males and 1,270,164 are women (Ethiopia, 2008). There are 125 health facilities: 14 government hospitals with 1150 nurses overall, 1 comprehensive and specialized hospital with specialist care, and 5 more private general hospitals. However, the public hospitals in this zone are estimated to provide for 5 million people. The study hospitals have a mandatory MAE reporting system. Each unit has a medication administration sheet, physician order sheet, and nurse-to-nurse handover sheet that can be considered a daily audit mechanism. In some study hospitals, there are also clinical audit committees, which are mainly responsible for handling these kinds of errors. If the nurse did MAEs, either the nurse alone or the unit coordinators would report, and based on the type and frequency of error made, disciplinary measures would be taken, starting from a verbal warning to a medico-legal court.
Study Design
A multicenter hospital-based cross-sectional study design was employed.
Population
The current study's population sources were all nurses working in South Wollo Zone government hospitals in northeastern Ethiopia. The actual data, however, was gathered from nurses working in five randomly chosen government hospitals in northeastern Ethiopia's south Wollo zone.
Eligibility Criteria
Nurses who were explicitly enrolled in client health care provisions, had working experience longer than 6 months, have a minimum diploma qualification in nursing, and are full-time workers were included. whereas, nurses who had no direct contact with drug provision, were involved in administrative duties, had difficulty administering questionnaires, refused to participate in this study, or were unavailable for the duration of the study were excluded.
Sample Size Determination
A formula for a single population proportion was applied to determine the required final samples included in this study. Taking the following assumption into account: a study finding conducted in five referral hospitals in Ethiopia was used to obtain the required samples in this study and to obtain the maximum sample size for one of the factors (work interruption, 51.2% for medication administration errors (MAEs; Tsegaye et al., 2020), with a 95% level of confidence and a 5% margin of error. By including a 10% nonresponse rate, the total sample size increased to 423.
Sampling Procedure
Five of the fourteen government hospitals in the south Wollo zone were chosen at simple random using a lottery technique, namely: Dessie Comprehensive Specialized Hospital, Kombolicha General Hospital, Akesta Referral Hospital, Empress Zewuditu General Hospital, and Mekaneselam General Hospital. The randomly selected hospitals can represent more than half of the study population in the South Wollo Zone (633 nurses out of a total of 1150). Similarly, lists of study subjects were then distributed among the randomly selected hospitals using proportional allocation. As a result, once the sample size was determined, simple random sampling was used to select the final study participants from the prepared sampling frame. Medical, surgical, adult ICU, NICU, pediatrics, and orthopedics inpatient departments and emergency departments were represented proportionally.
Data Collection Instrument and Procedure
The tool used for data collection was a structured, self-administered questionnaire. The tool was adapted and modified from previous studies (Björkstén et al., 2016, Härkänen et al., 2019). It contains more than 50 questions arranged into four sections. The first section deals with the sociodemographic characteristics of the participants; age, sex, marital status, qualification, and work experience. The second section contains work-related factors on MAEs, which had a total of 21 questions, and of those, 18 inquirer responses were “yes” or “no,” coded as “1” and “0.” However, working shift, nurse-to-patient ratio, and types of prescription had more than two responses. Besides, the third section deals with nurse-related factors on MAE and has seven questions with a “yes” or “no” response coded as “1” or “0.” Negligence, no interest in the job, stress, mood disturbance, lack of knowledge, and experiencing either economic or personal and family problems. Lastly, the fourth section dealt with the reporting of MAEs for the last year, and if yes, there were eight types of errors and the participants could be reported. The types of errors had yes” or “no” responses and were coded as “1” or “0.” Participants who reported at least one type of error were considered to have made MAEs (Härkänen et al., 2019). Face validity and content validity were assessed by four experts to determine the instrument's validity. The content validity ratio (CVR) and content validity index (CVI) were calculated and found to be 0.23 and 0.84, indicating that the instrument is valid. The instrument's reliability was tested using Cronbach's alpha, which was 0.821, indicating that the instrument was reliable.
Operational Definitions
Omission drug error: when a nurse ignores the patient's request to provide the ordered medicine (Härkänen et al., 2019).
Dose error: When a nurse provides a miscalculated dose of drugs to patients, the therapeutic dose of the medicine administered is quite contrary to what has been issued (Härkänen et al., 2019).
Patient error: occurs when a drug is administered to an unintended patient (Härkänen et al., 2019, Björkstén et al., 2016).
Route of Administration Error: A route of administration error occurs when a drug is administered in a different route than it should be (Härkänen et al., 2019, Björkstén et al., 2016).
Ill-timed medication administration: Drug provision ≥1 h earlier or later than it should be (Härkänen et al., 2019, Björkstén et al., 2016).
Technical error: an error that occurs during dose calculation or when antagonist is not realized (Härkänen et al., 2019, Björkstén et al., 2016).
Wrong choice: Providing a patient with a nurse's choice of medication while disregarding what the doctor prescribed (Björkstén et al., 2016).
Administering without assessment: giving medication to patients without first assessing their allergy history (Björkstén et al., 2016).
Medication Administration Errors (MAEs): the presence of at least one of the medication errors mentioned above (Björkstén et al., 2016).
Data Quality Management and Analysis
The tool has been translated into the local Amharic language. Ten data collectors and five supervisors were trained, and a pretest of 5% of the sample size was done at the nearby hospital with appropriate amendments. The confidentiality of the information was maintained by placing a strong emphasis on the “no name, no blame” principle. The data was cleaned, encoded, and entered into Epi-Data software version 4.7 before being exported to SPSS version 26 for analysis. The magnitude of MAEs was calculated and assessed using descriptive statistics. The effect of predictor variables on the dependent variable was evaluated using binary logistic regression analysis. After performing bivariable logistic regression analysis, variables with a P-value of less than 0.25 were considered significant and were transferred to multivariable binary logistic regression analysis. The final model test was performed by Hosmer-Leme to demonstrate goodness of fit. When the p-value was less than 0.05, significance was declared, and if it was greater, it was assumed to be confounding variables. A collinearity test was determined after analyzing the VIF results of each variable, which were between 1 and 3.
Result
A sample of 423 participants were involved in this study, of which 416 nurses successfully completed the questionnaire, resulting in a response rate of 98.4%.
Socio-Demographic Properties of Respondents
The respondents’ median age was 30 (SD ± 7.03) years, and 170 (40.9%) of them were between the ages of 20 and 30. Females made up approximately 222 (53.4%) of the total participants. The vast majority of participants (344; 82.7%) were nursing BSc holders; about 185 (52.9%) of them were married; and 143 (34.4%) participants had 15 or more years of professional working experience (Table 1).
Socio-Demographic Characteristics of Nurses Working in South Wollo Zone Public Hospitals, Northeastern Ethiopia, 2022 (n = 416).

Work-Related Factors on MAEs
Approximately half (50.7%) of the staff provided service to more than 11 clients individually, with 369 (88.7%) of the prescribed medications ordered by handwriting (they didn't use computerized prescriptions). Only 35.3% and 13.2% of all study participants had medication administration-related guidelines and error reporting systems in the institutions where they worked, respectively. Of the 416 participants, 136 (32.7%) and 144 (34.6%) nurses reported being overburdened and lacking time to provide health care services on multiple occasions in the previous year. Only 107 (25.7%), 78 (18.8%), and 43 (10.3%) nurses received safe drug administration training, were interrupted while giving medication, and administered medication to physiologically unstable patients, respectively. Furthermore, 326 (78.4%) and 63 (15.1%) of nurses neither consulted their colleagues before administering medications they were unfamiliar with nor brought their faults to the attention of their heads, respectively (Table 2).
Work-Related Variables Among Nurses Working in South Wollo Zone Public Hospitals, Northeastern Ethiopia, 2022 (n = 416).

Nurse-Related Factors on MAEs
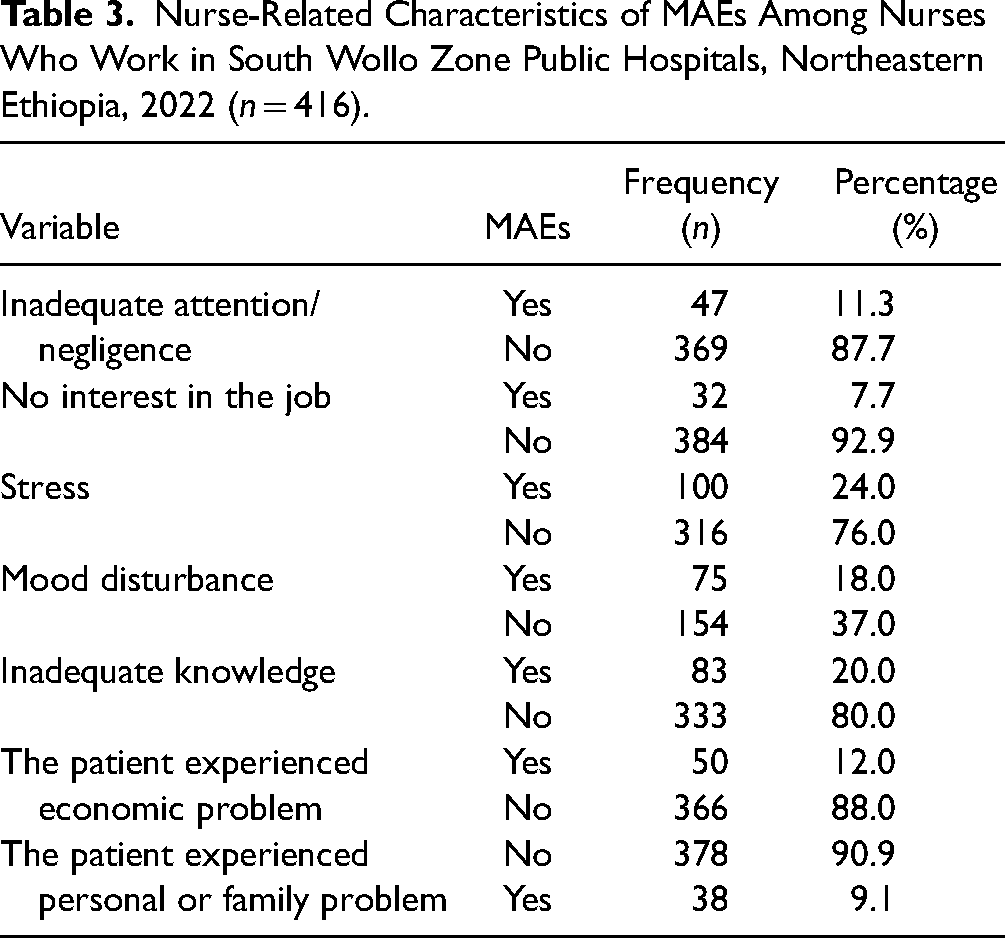
In this study, within the last 12 months, the majority of participants, 369 (87.7%), did not provide medication inadvertently, 316 (76.0%) did not provide medication while they were stressed out, 316 (76.0%) did not provide medication while their mood was off, and 333 (80%) did not provide medication due to inadequate knowledge (Table 3).
Nurse-Related Characteristics of MAEs Among Nurses Who Work in South Wollo Zone Public Hospitals, Northeastern Ethiopia, 2022 (n = 416).
Magnitude of MAEs
The overall magnitude of medication administration errors (MAE) in the study area was 229 (55%), 95% CI (0.501, 0.599), with improper timing being the most common MAE (121, 29.1%), followed by missing or omitted doses (103, 24.8%), and provision of miscalculated or incorrect doses (88, 21.2%). Furthermore, the least reported MAEs were giving the right medication to the wrong patient (23, 5.5%) and providing medication based on a nurse's prescription (26, 6.3%; Figure 1). The MAEs were reported to be very common in the morning session (150; 65.5%) and accompanied by night shifts (79; 34.5%). Nurses who worked at the adult medical inpatient department reported the most common MAEs, with 85 (37.1%), followed by the surgical inpatient department with 62 (27%). Besides, the least common MAEs were reported in the adult ICU 6 (2.6%). Only two cases were brought to court due to medico-legal issue and money compensation for victim clients was paid.

Types of MAEs among Nurses Working in South Wollo Zone Public Hospitals, Northeastern Ethiopia, 2022 (n = 416).
Factors Associated with MAEs
After running a multivariable logistic regression analysis, the final predictors of MAEs were determined to be the following variables: work experience, nurse–patient ratio, interruption, lack of training, absence of guidelines, scarcity of time, workload, stress, and inadequate knowledge.
In this study, the workload was found to be associated with medication administration errors, where nurses who provided health care services for more than 11 patients per day were 2.52 times more likely to make errors in drug administration than those who served for less than or equal to 7 patients (AOR: 2.52, 95% CI [1.187, 6.78]). Similarly, those nurses who were interrupted by somebody or something were nearly 5 times more likely to carry out drug administration errors than those who didn’t (AOR: 4.943, 95% CI [2.088, 11.712]). Likewise, nurses who didn’t take safe drug administration training were approximately six times more likely to perform errors during medication administration services than those who took similar training (AOR: 6.35, 95% CI [3.340, 7.053]). Furthermore, those with less than or equal to 4 years of work experience and those with 5–9 years of work experience were nearly four times and three times more likely to make drug administration errors than those with 15 or more years of professional experience, respectively (AOR: 3.802, 95% CI [1.343, 10.763]), (AOR: 2.804, 95% CI [1.062, 7.424]). Nurses who became busy (lacked time) were nearly six times more likely to make medication errors than those who did not (AOR: 5.637, 95% CI [2.575, 12.337]), and nurses who did not have medication safety guidelines in their institution were almost two times more likely to make administration errors than those who did (AOR: 2.418, 95% CI [1.556, 5.086]; Table 4).
Factors Contributing to MAEs Among Nurses Working in South Wollo Zone Public Hospitals, Northeastern Ethiopia, 2022 (n = 416).

NB.*** stands for p ≤ .001; ** stands for p ≤ 0.05 in multivariate (backward stepwise log- regression).
Discussion
The current study's objectives were to measure the magnitude of MAEs in the study institutions and pinpoint the relevant factors that influence nurses’ decisions to administer MAEs. The findings of this study showed that the magnitude of MAEs in the study area was 229 (55%), 95% CI [0.501, 0.599]. In addition, work experience, nurse–patient ratio, interruptions, lack of training, absence of guidelines, scarcity of time, workload, stress, and inadequate knowledge were important predictors of medication administration errors.
The magnitude of this study is in line with the results of the previous studies done at Jimma University Hospital (51.8%; Feyissa et al., 2020), Felegehiwot referral hospital (56.4%; Feleke et al., 2015), three public hospitals in north-western Amhara (Gondar Specialized Hospital, Felegehiwot Specialized Hospital, and Debre-Markos Hospital, 54%; Mekonen et al., 2020), and five referral hospitals in the eastern Amhara region (57.7%; Tsegaye et al., 2020).
However, the magnitude of medication administration errors in this study was less frequent than findings done at public hospitals in the Tigray region (62.7%; Baraki et al., 2018), three public hospitals in Ethiopia's capital Addis Abeba (68.1%; Wondmieneh et al., 2020), and two European nations (England and Wales, 66.4%; Härkänen et al., 2019). The difference might be due to the methodologies (since the above-mentioned studies were prospective and observation-based), the hospital setting, and the availability of error management systems.
Furthermore, the magnitude of medication administration errors in this study was more prevalent than findings of studies carried out in Dutch hospitals (13.7%; Jessurun et al., 2022), Jordanian nurses’ MAEs (28.3%; Alrabadi et al., 2020), Malaysia (30.5%; Shitu et al., 2020), and Jordanian pediatric nurses (26.5%; Abu Farha et al., 2018), as well as in public hospitals in Ethiopia (37.3%; Asefa 2021), and Gondar University Specialized Hospital (29.1%; Bifftu et al., 2016). The mismatch may be caused by differences in the time frame in which a study was done, the research methodologies used, the environment in which a study was conducted, and the availability of error management systems.
In this study, those with less than or equal to four years of work experience, as well as those with five to nine years of work experience, were nearly four times and three times more likely, respectively, to make drug administration errors than those with 15 or more years of professional experience. This finding is in line with studies in the Felegehiwot referral hospital (Feleke et al., 2015), public hospitals in Addis Ababa (Tassew et al., 2022), and tertiary hospitals in Addis Ababa (Wondmieneh et al., 2020). One possible explanation is that medication administration is part of basic nursing practice, and the nurse will improve his or her knowledge and skills in medication administration through practice, working in different units, and experience with the administration of various types of drugs. If the nurse has less experience, the likelihood of MAEs increases. This implies that hospital and nurse managers think about less experienced nurses and prioritize training, guidelines, and clinical mentorship for MAEs.
Similarly, in the current study, the nurse-patient ratio was an important predictor of MAEs, where nurses who provided patient care for more than 11 patients per day were nearly three times more likely to make errors in drug administration than those who served for less than or equal to 7 patients. This is consistent with studies in Ethiopia, which include the Felegehiwot referral hospital (Feleke et al., 2015), North Shewa public hospitals (Asefa et al., 2021), and public hospitals in Addis Ababa (Tassew et al., 2022). This could be because, since the nurses are overburdened, medication administration is a single task in nursing practice, and as the number of patients per nurse increases, so does the workload. Therefore, the workload increases the likelihood of making MAEs.
Interrupting nurses during drug administration increases the likelihood of medication errors. This is consistent with the findings in Ethiopia, which include Felegehiwot referral hospital (Feleke et al., 2015), Addis Abeba public hospitals (Tassew et al., 2022), Amhara Region referral hospitals (Mekonen et al., 2020), Addis Abeba tertiary hospitals (Wondmieneh et al., 2020), and five referrals from the Amhara Regional State (Tsegaye et al., 2020). This is due to the fact that, because drug preparation and administration require mental focus, distractions during these tasks cause cognitive failures in nurses in terms of working memory and attention to detail.
Inadequate knowledge contributes to MAEs in this study. This finding was backed by studies conducted in hospitals in Australia (Alomari et al., 2015), Africa (Mekonnen et al., 2018), London (Alqasoumi, 2016), as well as Amhara Region Referral Hospitals in Ethiopia (Mekonen et al., 2020). Knowledge serves as the foundation for clinical decision-making and implementation; a lack of it leads to poor decision-making and performance. Medication administration is a complex process that usually requires a thorough understanding of the drug's name, side effects, dosage, and patient condition, as well as its application in clinical practice. When this is applied in clinical practice, MAEs occur as a result of a lack of knowledge. This means that the nurse must receive extensive and up-to-date pharmacologic training on-site in order to maintain patient safety and good clinical practice habits, including medication administration.
In the current study, lack of training and unavailability of medication administration guidelines in the hospital greatly contribute to MAEs. This is supported by findings from tertiary hospitals in Addis Ababa (Wondmieneh et al., 2020), public hospitals in Tigray (Baraki et al., 2018), and five referrals in Amhara regional state (Tsegaye et al., 2020). Keeping drug and drug-related knowledge and skills up to date for the sake of patient safety is a priority concern. As a result, if the nurse receives current training on drug administration procedures and current guidelines are available in the medication preparation room, they will be able to comply with patient safety and evidence-based practice, reducing MAEs and enhancing the early reporting culture. This is also endorsed by WHO's 2017 “medication without harm” strategies, which strive to enhance patient safety by minimizing medication errors by up to 50% over the next 5 years, from 2017 to 2022 (WHO Global Patient Safety Challenge on Medication Safety, 2017).
Consequently, the regional health, hospital, and nurse managers should improve the nurse-patient workload and ratio by increasing the number of care providers per standard. Moreover, special attention shall be paid to less experienced nurses and strengthened their capacity by providing continued career development training, availing themselves of medication administration guidelines sufficiently, and creating a mentoring system. Lastly, the hospitals should strengthen MAE mandatory reporting and measures taken, as well as the digital prescription and documentation systems, to curtail errors and ultimately ensure patient safety.
Strengths and Limitations of the Study
The researchers used the Switchboard, a peer-reviewed and validated survey tool, and worked with more than five public hospitals. However, due to a lack of time and financial resources, the actual practice of drug administration was not observed. The disadvantage of a self-administered questionnaire is that it does not always reveal the true scope and contributing causes of pharmaceutical administration errors in a healthcare setting. Furthermore, if sufficient funding had been available, an interventional study rather than a cross-sectional study would have been preferable.
Implication for Practice
A proportional patient-to-nurse ratio, a pleasant working environment, and adequate time for each procedure will reduce MAEs among nurses significantly. As a result, patient safety will be ensured, as will the quality of care. Furthermore, it aids in the establishment of a structured system for the daily reporting of medication administration errors and digital medication documentation for nurses and other medical personnel.
Conclusion
In the study area, medication administration errors were common and required more effort. Patient load, intermissions, service experience, time deficits, stress, a lack of training, and the absence of guidelines were all linked with medication administration errors. The hospitals shall consider nurses’ physical and emotional well-being in their working places, and avoiding job-related distractors such as workload and stressful jobs may have positive implications for decreasing medication errors. Consequentially, this ensures patient safety. Hospital administrators must establish a link with continuing professional development centers so that nurses can receive safe medication administration training and the guidelines will be accessible at work.
Footnotes
Abbreviations
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.