
Abstract
Introduction
Low birth weight is one of the important predictors of perinatal survival, infant morbidity, and mortality, as well as the risk of developmental disabilities and diseases in the future.
Objective(s)
The study aimed to identify the associated factors of low birth weight among newborns at Debre Tabor referral hospital, Northwest Ethiopia.
Methods
A hospital-based cross-sectional study was conducted from January 1, 2021 to October 30, 2021 at Debre Tabor Referral Hospital. A total sample of 420 newborn birth records was considered. The binary logistic regression model was used to assess the associated factors of low birth weight. The results are presented as crude odds ratios and adjusted odds ratios (AOR) together with their corresponding 95% confidence intervals.
Results
In this study, 422 participants were included. Rural residence (AOR = 2.01; 95%CI 1.10–3.69), married marital status (AOR = 0.82; 95%CI 0.78–0.86), formal education (AOR = 0.79; 95%CI 0.67–0.92), smoking during pregnancy (AOR = 1.19; 95%CI 1.07–1.33), attended antenatal care (ANC) visits (AOR = 0.57; 95%CI 0.35–0.91), diabetes during pregnancy (AOR = 4.34; 95%CI 3.50–5.39), iron supplementation (AOR = 0.23; 95%CI 0.20–0.25), and maternal history of anemia (AOR = 5.87; 95%CI 2.67–12.89) were significantly associated with low birth weight of newborns.
Conclusion
This finding showed that residence, marital status, educational status, smoking during pregnancy, ANC visit, diabetes during pregnancy, iron supplementation, and mother's history of anemia were significantly associated with low birth weight. Therefore, policy makers and public health experts/practitioners should plan smoking preventive public health promotion campaigns. Furthermore, it is important that all health professionals properly manage the possible cause of LBW during pregnancy.
Introduction
The newborn's weight is the initial measurement taken after birth. It is one of the main determinants of perinatal survival, infant morbidity, and mortality, as well as the risk of developmental disabilities and illnesses in the future (Gebregzabiherher et al., 2017; Mingude et al., 2020). Low birth weight (LBW) is defined as weight at birth of less than 2500 g (5.5 pounds) (WHO, 2019). Every year, more than 20 million babies with LBW are born around the world (Tessema et al., 2021).
Review of Literature
The prevalence of LBW in developing countries (16.5%) is more than twice the prevalence in developed regions (7%) (Taywade & Pisudde, 2017). Most (96.5%) of LBW births were reported from low-income and middle-income countries and, especially, in the most vulnerable populations (Zaveri et al., 2020).
Africa is a continent that has high rates of children born with LBW and the most recent studies have shown a high rate of child mortality (Tchamo et al., 2016). It is estimated that in sub-Saharan Africa, LBW represents 14.3%, which is approximately twice the rate of LBW in European countries (Tchamo et al., 2016). In Ethiopia, according to the Summary Report of the National Newborn and Child Survival Strategy of the Federal Minister of Health, the prevalence of LBW was found to be 20% (Mingude et al., 2020). Studies conducted in different parts of the country, namely Addis Ababa, Gondar, and Tigray, showed different rates of LBW 8.8%, 11.2%, and 14.6%, respectively (Adane et al., 2014; Gebremedhin et al., 2015; Mulatu et al., 2017).
In Ethiopia, the under-five mortality rate is 59 per 1,000 live births (Gebrehawerya et al., 2018). LBW alone can be considered an important predictor of child mortality risk (Vilanova et al., 2019). Understanding the causes of LBW is important for designing cost-effective intervention strategies to reduce LBW rates. However, in Ethiopia, there is limited research on the associated factors of LBW, particularly in northwest Ethiopia. Several studies have shown that LBW was significantly associated with maternal residence, marital status, age at first pregnancy, mother history of spontaneous abortion, maternal nutritional status, inter-pregnancy interval, antenatal care (ANC) follow-up, pregnancy-induced hypertension, anemia at pregnancy, and cigarette smoking (Girma et al., 2019). LBW is the most significant risk factor for neonatal and infant mortality. It is one of the major public health problems in developing countries, especially in Ethiopia (Katiso et al., 2020). Therefore, this study aimed to identify the associated factors of LBW among newborns at Debre Tabor Referral Hospital, Northwest Ethiopia.
Methods
Design
A hospital-based cross-sectional study was conducted from January 1, 2021 to October 30, 2021 at the delivery ward of Debre Tabor Referral Hospital. The hospital is located in Debre Tabor town, 666 km from Addis Ababa. It serves about 3,840 deliveries annually (Bayih et al., 2020). The hospital currently serves approximately 3.5 million people in its catchment area and is used as a teaching hospital for different disciplines of medical and health sciences students of Debre Tabor University (Tesfaw et al., 2019). Annually, nearly more than 1250 neonates were admitted to the neonatal intensive care unit with different health problems. It has 22 beds, 3 pediatricians, and 20 nurses, of which 2 are neonatal nurses.
Research Question(s)
Is mother's age, residence, marital status, educational status, and occupation associated with low birth weight among newborns at Debre Tabor referral hospital, Northwest Ethiopia?
Is a mother's alcohol consumption during pregnancy, and smoking during pregnancy associated with low birth weight among newborns at Debre Tabor referral hospital, Northwest Ethiopia?
Is a mother's history of spontaneous abortion, ANC visits, diabetes during pregnancy, iron supplementation during pregnancy, history of gestational hypertension, and history of anemia associated with low birth weight among newborns at Debre Tabor referral hospital, Northwest Ethiopia?
Sample
A single population proportion formula was used to determine the sample size at 95% confidence level, marginal error of 5%, the proportion of LBW 50%, and adding a non-response rate of 10%. Therefore, the calculated sample size is n = 422. A simple random sampling technique was used to select study participants. Birth records were selected using a lottery based on their identification number.
Inclusion Criteria and Exclusion Criteria
All newborns delivered at the Debre Tabor referral hospital and met the inclusion criteria were recruited for the study/used as a source population. A preterm baby (preterm birth is when a baby is born too early, the gestational age from 28 completed weeks to 37 completed weeks), births with comorbidities such as twin delivery, still birth, and newborns above normal birth weight (birth weight > 4,000 g) were excluded from the study.
Data Collection Procedure
The data was collected by observing medical records of the mothers and the newborns using a checklist. The recording of medical charts was conducted by five trained midwives working in delivery rooms of the Debre tabor referral hospital and two supervisors.
Data Quality Management
The data collection instrument was pre-tested on 21 respondents out of the total sample size in Debre tabor referral hospital before actual data collection was made. The pre-test was used to check for language clarity, appropriateness of data collection tools, time estimation and for the necessary adjustment. Training concerning the data collection tools and data collection process has been given to both data collectors and supervisors. During the data collection, supervision was conducted by supervisors and principal investigators for the quality of data. Finally, all the collected data was also checked by the supervisor and investigator for its completeness and accuracy. Consistency has been examined through a random selection of a checklist.
Variables in the Study
Dependent Variable
The response variable for this study was the birth weight of a newborn categorized as normal birth weight (birth weight ≥2,500 g and ≤ 4,000 g) and LBW (birth weight < 2,500 g) (WHO, 2004).
Independent Variables
The study used 13 independent variables. These independent variables include the sex of the newborn, the age of the mother, the residence of the mother, marital status of the mother, the educational status of the mother, smoking during pregnancy, alcohol consumption during pregnancy, the history of spontaneous abortion of the mother, ANC visits (ANC at least four times increases the likelihood of receiving effective maternal health interventions during the antenatal period (Tessema & Minyihun, 2021)), iron supplementation during the pregnancy, the history of hypertension during pregnancy, the history of anemia during pregnancy, and gestational diabetes during pregnancy.
Statistical Analysis
Data was extracted using SPSS version 21 software and then exported to the R version 4.0.3 statistical software for further analysis. Descriptive statistics including frequencies and percentages were computed to describe study participants. Multicollinearity diagnostics were performed to check for collinearity between independent variables and evaluate whether each of the independent variables in the multiple analysis had a tolerance value > 0.1 against every other independent variable. A dependent variable in a binary logistic regression has two levels (Harris, 2021). Therefore, a binary logistic regression analysis was performed to identify predictors of LBW. The adjusted odds ratio (AOR) with a 95% confidence interval (CI) and p-value < .05 were used to claim statistical significance.
Results
Sample Characteristics
In this study, a total of 422 birth records from newborn babies were included. Most mothers (48.10%) were 15–24 years old. Most of the study respondents were from rural residences (63.27%). About 54.50% of women were married, 19.43% were never married, 26.07% were widowed/divorced. About 57.34% of mothers had no formal education and 42.65% of mothers had formal education. Most of the respondents were housewives (60.19%) and 39.81% of the respondents were employed. The majority (76.54%) of mothers drank alcohol during pregnancy, 15.17% of mothers smoked during pregnancy, and 7.58% of the respondents had a history of spontaneous abortion. Out of 422 mothers, 63.74% of mothers did not attend ANC visits. Of the 422 respondents, 41.94% of mothers had diabetes during pregnancy, 25.12% of mothers used iron supplementation during pregnancy, 13.03% of mothers had a history of hypertension during pregnancy, and 19.19% of mothers had a history of anemia (Table 1).
Socio-Demographic and Obstetric Characteristics of the Mother who Gave Birth at Debre Tabor Hospital, Northwest of Ethiopia.

Factors Associated With Low Birth Weight
In binary logistic regression analysis, the odds of LBW were 2.01 (AOR = 2.01; 95% CI 1.10, 3.69) times higher in newborns from mothers who lived in rural areas compared to newborns from mothers who lived in urban areas. The odds of LBW were 0.82 (AOR = 0.82; 95% CI 0.78, 0.86) times lower in newborns whose mother's marital status was married compared to newborns whose mother's marital status was never married. The odds of LBW were 0.79 (AOR = 0.79; 95% CI 0.67, 0.92) times lower in newborns whose mother's educational status was formal education compared to newborns whose mother's educational status was no formal education. The odds of LBW were 1.19 (AOR = 1.19; 95% CI 1.07, 1.33) times higher in newborns from mothers who smoked compared to newborns from mothers who did not smoke. The odds of LBW were 0.57 (AOR = 0.57; 95% CI 0.35, 0.91) times lower among mothers who attended at least four ANC visits compared to mothers who did not attend at least four ANC visits during pregnancy. The odds of LBW were 4.34 (AOR = 4.34; 95% CI 3.50, 5.39) times higher among mothers who had diabetes during pregnancy compared to mothers who did not have diabetes during pregnancy. The odds of LBW were 0.23 (AOR = 0.23; 95% CI 0.20, 0.25) times lower among mothers who took iron supplementation compared to mothers who did not take iron supplementation during pregnancy. The odds of LBW were 5.87 (AOR = 5.87; 95% CI 2.67, 12.89) times higher among mothers who have a history of anemia compared to mothers who did not have a history of anemia during pregnancy (Table 2).
Factors Associated With Low Birth Weight Among Mothers who Gave Birth at Debre Tabor Hospital, Northwest Ethiopia.
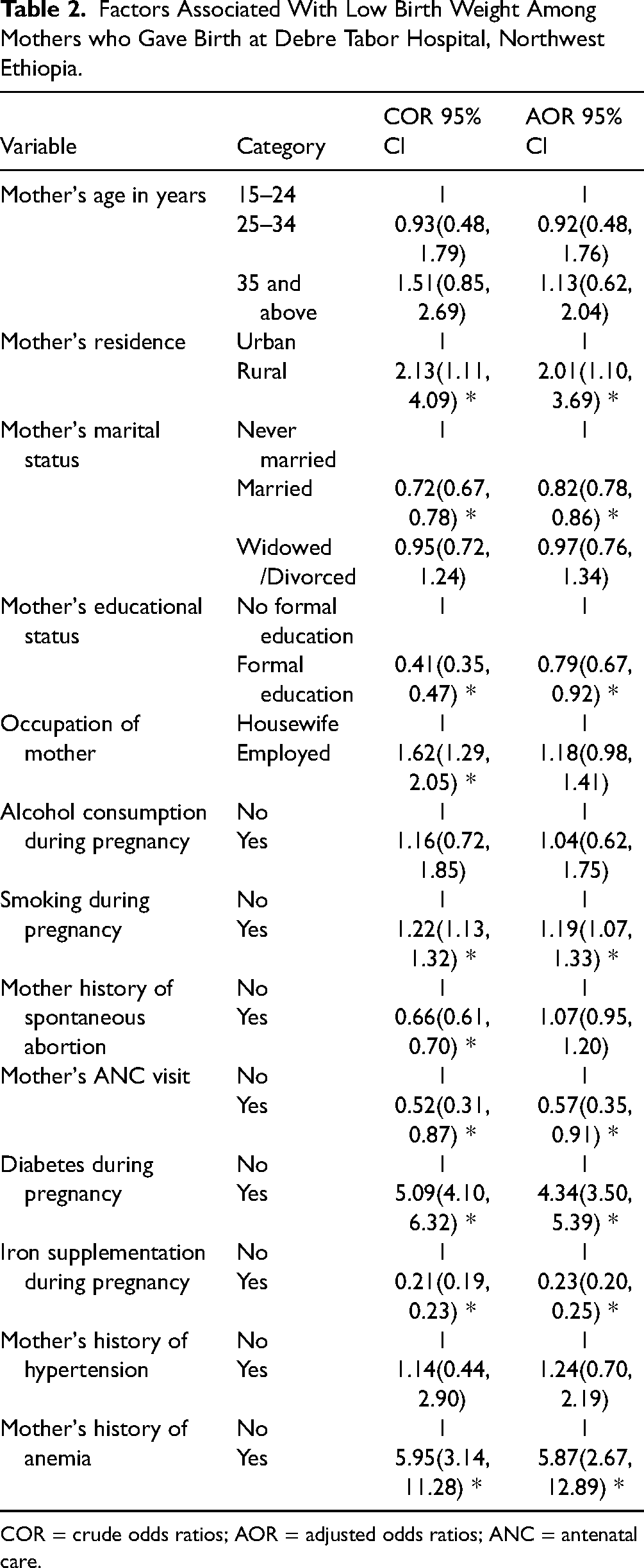
COR = crude odds ratios; AOR = adjusted odds ratios; ANC = antenatal care.
Discussion
The study aimed to identify the determinants of LBW among newborn births at Debre Tabor referral hospital, Northwest, Ethiopia. Residence of mothers was significantly associated with LBW. The odds of LBW were higher among mothers who lived in rural areas compared to mothers who lived in urban areas. This finding was consistent with other studies conducted in Ethiopia and Zimbabwe (Bekela et al., 2020; Demelash et al., 2015; Feresu et al., 2015; Gebremedhin et al., 2015). The probable explanation might be that the low accessibility of health facilities and the utilization of maternal health services in a rural area could increase the likelihood of having a LBW of newborns.
The results of this study also revealed that the martial status of mothers significantly associated with birth weight of a newborn. Mothers whose marital status was married were negatively associated with LBW compared to mothers whose marital status was never married. This finding was consistent with another study conducted in Ethiopia (Mulu et al., 2020). This might be because mothers who have husbands have a high chance of complete balanced nutrition (having more income to afford fresh food) and have high support to get ANC service (Wiradnyani et al., 2016). This result showed that the educational status of the mothers significantly associated with the weight of newborns. This finding was consistent with other studies conducted in Ethiopia (Bekela et al., 2020; Demelash et al., 2015; Kastro et al., 2018). This could be because educated mothers visit the health facility in a timely manner for ANC, have better knowledge of fetus growth, high dietary knowledge, and timely detection and treatment of different infections (Gizaw & Gebremedhin, 2018; Ngwira & Stanley, 2015).
The odds of LBW for newborns from mothers who smoked cigarettes were higher compared to newborns from mothers who did not smoke cigarettes. This finding was consistent with other studies conducted in Ethiopia and Pakistan (Dendir & Deyessa, 2017; Rozi et al., 2016). This is because smoking has adverse effects on the developing fetus by increasing the level of nicotine and carbon monoxide in the blood, resulting in a deficiency of oxygen and nutrient delivery to the growing fetus (Ashford et al., 2010; Lambers & Clark, 1996; Martinez et al., 1994; Mingude et al., 2020).
In the present study, the ANC visit was another predictor of LBW. The result showed that mothers who attended ANC visits are more likely to get normal-weight babies compared to mothers who did not attend ANC visits. This study was consistent with other studies conducted in Ethiopia, Morocco, and Nepal (Asmare et al., 2018; Bhaskar et al., 2015; Mumbare et al., 2012; Noureddine & Abdellatif, 2015). This might be because ANC visits are very important for both fetus and mothers, as they provide opportunities for timely detection and intervention of fetal/maternal problems and enable the mother to promote her health through counseling that she might receive (Tadesse Berehe & Modibia, 2020). Another possible explanation might be that mothers who had ANC follow-up could receive nutritional counseling to improve their dietary diversity, which allows her and her fetus to have better pregnancy outcomes (Assefa et al., 2012).
In addition, the result showed that the occurrence of diabetes during pregnancy was a risk factor for LBW. The odds of LBW were higher in mothers who had diabetes during pregnancy compared to mothers who did not have diabetes during the pregnancy period. This finding was inconsistent with the other studies conducted in Ethiopia, China, and Iran (Chen et al., 2013; Demelash et al., 2015; Mirzarahimi et al., 2013). This inconsistency may be due to mothers who have diabetes during pregnancy took the medication of diabetes that affects the weight of the newborn baby. Another possible explanation of diabetes is causes/risk factors of preterm due to that may occur LBW. Women with diabetes had significantly more risk factors than women without diabetes to LBW babies (Persson et al., 2018). In addition, gestational diabetes affects the mother in late pregnancy, after the baby’s body has been formed, but while the baby is busy growing.
Furthermore, mothers who received iron supplementation were also at lower risk of delivering LBW babies than mothers who did not receive iron supplementation during the current pregnancy. This result is similar to another study conducted in Kerala (Ismail & Venugopalan, 2016). This could be because iron and folic acid supplementation for pregnant mothers is of great importance in preventing anemia during pregnancy, thereby improving better health outcomes for both the mother and the fetus (Abu-Ouf & Jan, 2015; Mahande & Obure, 2016; Smith et al., 2003; Smits & Essed, 2001). Finally, a mother's history of anemia has significantly affected the birth weight of babies. This indicates that mothers who had a history of anemia were more likely to have LBW babies compared to mothers who did not have a history of anemia. This study was consistent with other studies conducted in Ethiopia and Maharashtra (Domple et al., 2016; Gebrehawerya et al., 2018; Mingude et al., 2020). This could be because anemia could alter oxygen and nutrient delivery to the fetus and delay normal intrauterine growth and also influence placental angiogenesis (Jwa et al., 2015; Stangret et al., 2017).
Strengths and Limitations
The strength of the present study is identifying the potential risk factors using the appropriate model. This study used hospital-based single-center cross-sectional data; the cross-sectional data does not show the cause-and-effect relationship between variables. This study was hospital-based and, therefore, may not be as good as population-based studies to generalize the results in the population. Home birth babies are not considered in this study. Other limitations did not test folic acid supplements, lack of quantification for alcohol intake and smoking during pregnancy.
Implications for Practice
This study identified the factors that contribute effectively to strategies of LBW prevention and to getting involved in birth weight stewardship programs.
Implications for Education and Research
Early intervention programs or special care for LBW children in school could be an effective means of improving the educational outcome and behavior of these children. It is also important to increase awareness among parents, teachers, and the community about the higher risk of low school performance for LBW children. The study provides baseline data in its research setting to develop a program that can enhance birth weight.
Conclusion
The findings of this study showed that residence, marital status of the mother, educational level of the mother, smoking status of the mother, ANC visits of the mother, diabetes during pregnancy, iron supplementation during pregnancy, and history of anemia of the mother were significantly associated with LBW. Therefore, the concerned health authorities and health professionals should strengthen the existing promotion of complete ANC and adhere to the iron and folic acid supplementation recommendations during ANC. In addition, policy makers and public health experts/practitioners should plan smoking preventive public health promotion campaigns. Furthermore, it is important that all health professionals properly manage the possible cause of LBW during pregnancy.
Footnotes
Acknowledgments
We would like to express our great thanks to Debre Tabor University Research and community service coordinators for facilitating this proposal work. Second, we would like to acknowledge Debre Tabor referral hospital staff for their cooperation and support to get the baseline data used to contract the sampling procedure. Last but not least, we would like to acknowledge our friends, who supported us all the time from the start to the end of this study.
Author Contributions
MWM: conceptualized, designed, prepared the original draft, data curation, performed the statistical analysis, interpretation of data, participated in the supervision, and draft the manuscript. SSM, ATB, and YAM: methodology, coordinated the study, acquisition, analysis, interpretation of data and review, and editing the revised manuscript. All authors read and approved the final manuscript.
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Consideration
Ethical approval for this study was obtained from the Institutional Review Board of Debre Tabor University, Debre Tabor, Ethiopia. Further permission was obtained from Debre Tabor Referral Hospital administration for the use of birth records. Data obtained within the study were treated as confidential and stored securely. This study is carried out in accordance with the Declaration of Helsinki.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.