
Abstract
Introduction
Adolescent pregnancy is considered a global public health problem that affects both developed and developing countries. While the obstetric and perinatal outcomes of adolescent pregnancies have been extensively studied, there is not much available data comparing the obstetric and perinatal outcomes of younger and older adolescents.
Objective
The objective of this study is to compare the obstetric and perinatal outcomes between two groups of adolescent pregnancy.
Methods
This unmatched case–control study was conducted at Gadarif Maternity Hospital in eastern Sudan. The cases (n = 141) were young/middle-aged adolescents (13–17 years), who were compared with older adolescents (18–19 years) as the controls (n = 159).
Results
Compared with controls, cases had a lower level of education (78.0% vs. 62.3%; P = .003). There was no significant difference between the cases and controls in terms of antenatal follow-up (56.0% vs. 57.9%; odds ratio [OR] = 0.92; 95% confidence interval [CI]: 0.58–1.46), maternal anemia (46.8% vs. 39.0%; OR = 0.72; 95% CI: 0.45–1.15), preterm delivery (11.3% vs. 10.7%; OR = 0.93; 95% CI: 0.45–1.92), a cesarean delivery (13.5% vs. 15.1%; OR = 1.14; 95% CI: 0.59–2.18), low birth weight (10.6% vs. 13.8%; OR = 0.74; 95% CI: 0.36–1.49), neonatal intensive care unit admission (10.6% vs. 7.5%; OR = 1.45; 95% CI: 0.65–3.23), or neonatal deaths (5.0% vs. 5.0%; OR = 0.98; 95% CI: 0.34–2.79).
Conclusion
Young/middle-aged pregnant Sudanese adolescents are not at increased risk of obstetric and perinatal complications compared to older pregnant adolescents.
Introduction
According to the World Health Organization, adolescence is defined as the phase of life between childhood and adulthood, which includes the ages of 10 to 19 years. This is an important stage in laying the foundations of good health (World Health Organization, 2023). The adolescent period is further divided into stages, with a widely acceptable scheme including early adolescence (10–14 years), middle adolescence (15–17 years), and late adolescence (18–19 years) (Akseer et al., 2022; Amerjee et al., 2020; Hardin et al., 2017; Zhang et al., 2020). Pregnancy during adolescence is a global public health problem that affects both developed and developing countries. Against this background, reducing adolescent pregnancy is crucial to achieving sustainable development goals (Alukagberie et al., 2015).
Review of Literature
The prevalence of adolescent pregnancies is very high in Africa, with an overall estimation of 24.8% in sub-Saharan Africa (Asmamaw et al., 2023) and 54.6% in East Africa (Worku et al., 2021). Factors leading to adolescent pregnancy are variable, including geographical, financial, educational, and social circumstances (Pradhan et al., 2015; Sagalova, Garcia et al., 2021a). Giving birth at an early age may have serious health implications for both the mother and the child, including preterm birth, low birth weight (LBW) (Thirukumar et al., 2020), postpartum hemorrhage, hypertensive disorders of pregnancy, anemia (Todhunter et al., 2022), cesarean delivery, operative vaginal delivery, low 5-min Apgar score, infections, neonatal sepsis (Eliner et al., 2022), and neonatal death (Indarti et al., 2020; Zhang et al., 2020). Conversely, other researchers have reported no significant difference in adverse obstetric outcomes in adolescent pregnant women who receive high-quality care compared to adult women of similar a sociodemographic background (Bukulmez and Deren, 2000; Raatikainen et al., 2006). Nevertheless, giving birth at an early age may also increase the likelihood of being poor, illiterate, and having more children than adults (Sagalova, Nanama et al., 2021b). Adolescent marriage and socioeconomic status are inversely related, with early marriage often leading to reduced educational attainment, limited economic opportunities, and increased poverty, particularly for girls. This may be explained by the fact that caring for a child may significantly impairs mother's ability to complete education, obtain employment, and become financially independent (Shpiegel and Cascardi, 2018). Conversely, poverty can be a driver of adolescent marriage, especially in Africa (Kok et al., 2023).
Younger adolescents may have defining characteristics, including less developed muscles, joints, and bones, especially the pelvis, which may contribute to impairing pregnancy outcomes. Despite this, the majority of research that has addressed adolescent pregnancy has compared their obstetric and perinatal outcomes to those of adults, and only a few studies have compared pregnancy outcomes among early and late adolescents (Abu-Heija et al., 2016; Ambia et al., 2023; Ergen et al., 2017; Radu et al., 2022; Zhang et al., 2020). For example, in Oman, Abu-Heija et al. (2016) reported that early teenage pregnant Omani women are not at increased risk of obstetric and perinatal complication compared to older teenagers. Pregnancy outcomes vary between different populations and geographical areas, so any population should have been evaluated in terms of its own critical data. A previous study has shown that 31.7% of deliveries in Khartoum, Sudan, were performed on those less than 20 years of age, and teenage pregnancies were associated with less education, lower antenatal attendance, and an increased prevalence of anemia (Adam et al., 2009). The aim of this study was to compare the obstetric and perinatal outcomes of the young/middle-aged Sudanese adolescents (13–17 years) and their relatively older counterparts (18–19 years) who gave birth at Gadarif Maternity Hospital. The study sought to assess whether there were differences in outcomes between these two groups, with the goal of identifying and targeting the more vulnerable adolescents. Based on clinical observations, there appeared to be no increased risk of adverse outcomes among young/middle-aged adolescents compared to their older counterparts. This study aimed to gather data that could inform targeted interventions for at-risk adolescent populations.
Methods
Study Area
Gadarif Maternity Hospital is the largest government-run maternity hospital in eastern Sudan. Situated in Gadarif, the capital of Al Gadarif State, it is approximately 410 km east of the capital, Khartoum. Serving a population of nearly 500,000 people, the hospital offers comprehensive services to women throughout the state. The antenatal and postnatal clinics are covered by hospital staff and provided to patients free of charge. High rates of teenage pregnancy, its complications including poor antenatal care, preterm birth, and obstructed labor were reported in eastern Sudan (Ali et al., 2011). This is similar to the neighboring African countries (Asmamaw et al., 2023; Mezmur et al., 2021). The overall teenage pregnancy in sub-Saharan Africa countries was 25.0%, and adolescents from Chad were more than three times at risk of being pregnant during teenage (Asmamaw et al., 2023). In eastern Ethiopia, one in three teenagers had been pregnant (Mezmur et al., 2021).
Subjects and Study Design
This unmatched case–control study was conducted in the period from March 1, 2022 to February 28, 2023, at Gadarif Maternity Hospital, Sudan among adolescent pregnant women between 13 and 19 years of age who gave birth after 24 weeks gestation, that is, the recruitment was after delivery. The cases were young/middle-aged pregnant adolescents (13–17 years), and older pregnant adolescents (18–19 years) were the controls (Diabelková et al., 2023). The guidelines of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) initiative were strictly followed (von Elm et al., 2008). Similar study design was conducted in other context (Abu-Heija et al., 2016; Bukulmez and Deren, 2000).
Outcome Measures
In this study the cases were young/middle-aged pregnant adolescents (13–17 years), and older pregnant adolescents (18–19 years) were the controls. The main obstetric outcome measures include antenatal care visits (˃four visits, ˂four visits), maternal anemia (hemoglobin concentration ˂11 g/dl) (Ramsay, 2010), and mode of delivery (vaginal delivery or cesarean section). Perinatal outcome measures include preterm birth (delivery before 37 completed weeks of gestation), LBW ˂ 2.5 kg, neonatal intensive care unit (NICU) admission, and neonatal outcome (alive or dead).
Data Collection
Data were collected via a face to face questionnaire to women who gave birth in Gadarif Maternity Hospital during the study period. Two female medical officers were trained to counsel the participants and collect the data. Data collection was carried out on daily basis. All adolescents between 13 and 19 years of age who met the inclusion criteria and accept to participate were enrolled in the study after delivery and before discharge. Women were typically discharged 4 to 8 hr after vaginal delivery and 2 to 4 days after cesarean delivery. All participants signed a written informed consent form before data collection commence. The questionnaire contained items covering sociodemographic (age, residence, and education), obstetric and perinatal parameters. Women's height (cm) and weight (kg) were measured. Body mass index (BMI) was calculated as the weight (in kg) divided by the square of the height (in m) (kg/m2) (World Health Organization, 2024). Maternal and perinatal outcomes were then recorded, including the number of antenatal care visits (˃four visits, ˂four visits), maternal anemia (hemoglobin concentration ˂11 g/dl), preterm birth (delivery before 37 completed weeks of gestation), mode of delivery, LBW ˂ 2.5 kg, NICU admission, and neonatal outcome. Investigators did not interfere with the management decisions which were entirely taken by the hospital staff.
Inclusion and Exclusion Criteria
Sudanese primipara women with singleton pregnancy aged between 13 and 19 years who gave birth after 24 weeks in the Gadarif Maternity Hospital in the period from March 1, 2022 to February 28, 2023 were enrolled in the study. Women older than 19 years were excluded. Additionally, multiparous women and those with multiple pregnancies were also excluded to avoid confounders and potential bias as they may have different obstetric histories, experience, and risk factors compared to primipara women, whose outcomes are more directly influenced by age and first-time pregnancy experiences. These exclusions were necessary to maintain the homogeneity of the study population and to accurately assess the outcomes associated with young teenage pregnancies.
Sample Size Calculation
For this unmatched case–control study, the sample size was calculated using OpenEpi Menu software (Dean et al., 2024). We assumed that the ratio between the two groups of adolescents (older adolescents and the young/middle-aged adolescents) would be 1:1. Moreover, we assumed that 45.0% of the older adolescents and 60.0% of the younger adolescents would have anemia. This assumption was based on a previous study of adolescent pregnancy in Khartoum, Sudan (Adam et al., 2009).
Statistical Analysis
Version 24.0 of the Statistical Package for the Social Sciences® (SPSS®) for Windows (SPSS Inc., New York, United States) was used to analyze the data. Categorical data were expressed as frequencies and percentages. A Shapiro–Wilk test was used to evaluate the normality of the continuous variables, which were found not to be normally distributed and were expressed as medians (with interquartile ranges [IQRs]). The statistical analysis was performed using the chi-square test, and a univariate analysis was used to compare the adverse obstetric outcomes. Initially, we plan to perform multivariate logistic regression, however, the investigated variable had a P-value >.20. Differences between the values were considered significant when the two-side P-value <.05.
Results
A total of 300 eligible teenage women aged between 13 and 19 years were enrolled in the study. Of these 300 adolescent women, 141 (47%) were in the case group (13–17 years), while 159 (53%) were the controls (17–19 years). Table 1 shows the sociodemographic characteristics of the two groups. The median (IQR) age of the young/middle-aged adolescents was 17.0 (13.0–17.0) years, and it was 18 (18.0–19.0) years for the older group (P < .001). There were no significant differences in the place of residence or BMI between the two groups of adolescents. Compared with older adolescents, younger adolescents had a lower level of education (78.0% vs. 62.3%; P = .003).
Sociodemographic Characteristics of Pregnant Adolescents in Eastern Sudan, 2022–2023.

Table 2 compares the maternal outcomes between the two groups. There were no significant differences between young/middle-aged adolescents and old adolescents in terms of antenatal follow-up (56.0% vs. 57.9%; odds ratio [OR] = 0.92; 95% confidence interval [CI]: 0.58–1.46), maternal anemia (46.8% vs. 39.0%; OR = 0.72; 95% CI: 0.45–1.15), preterm delivery (11.3% vs. 10.7%; OR = 0.93; 95% CI: 0.45–1.92), and cesarean deliveries (13.5% vs. 15.1%; OR = 1.14; 95% CI: 0.59–2.18). Likewise, there were no significant differences between young/middle-aged adolescents and older adolescents in terms of the rates of LBW (10.6% vs. 13.8%; OR = 0.74; 95% CI: 0.36–1.49), NICU admissions (10.6% vs. 7.5%; OR = 1.45; 95% CI: 0.65–3.23), and neonatal deaths (5.0% vs. 5.0%; OR = 0.98; 95% CI: 0.34–2.79), as reported in Table 3.
Comparison of Maternal Outcomes of Pregnant Adolescents in Eastern Sudan, 2022–2023.

Note. 95% CI = 95 %confidence interval.
Comparison of Perinatal Outcomes of Pregnant Adolescents in Eastern Sudan, 2022–2023.
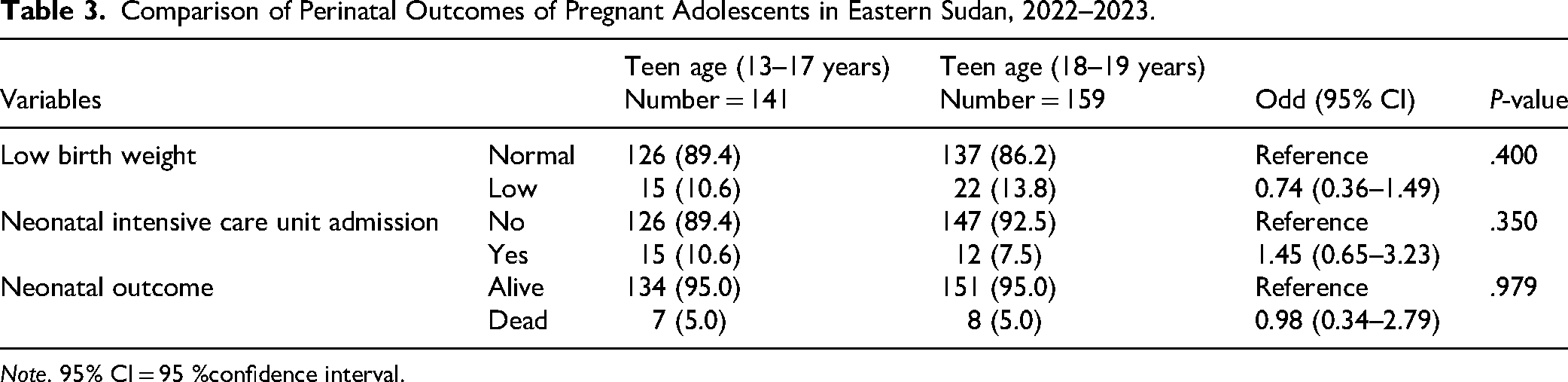
Note. 95% CI = 95 %confidence interval.
Discussion
The present study showed no differences in the maternal and perinatal outcomes between the two groups of pregnant adolescents. Furthermore, the antenatal follow-up in this cohort did not differ between the two groups. In contrast, a study conducted in Uganda in 2023, in which 82% of pregnant adolescents in a rural community had attended antenatal care (ANC) clinics (Kayemba et al., 2023). In India, adolescent pregnant women were shown to have better utilization of antenatal care services than their adult counterparts (Fulpagare et al., 2019). Generally, adolescent utilization of ANC varies widely among different communities, depending on different socioeconomic factors and the availability of these services (Anaba et al., 2022; Hackett et al., 2019).
This study showed a high prevalence of anemia at term among both the early/middle-aged adolescents and older adolescents, but this difference was not statistically significant. We have previously reported that anemia was more prevalent among adolescent pregnant women compared to adults (20–24 years) (Adam et al., 2009). Similarly, Heija et al. failed to find a significant difference in the prevalence of anemia between early (14–16 years) and late (17–19 years) pregnant adolescents (Abu-Heija et al., 2016). Generally, the prevalence of anemia has been shown to be high among adolescents (Annan et al., 2021; Indarti et al., 2020), and this can be justified by the increased nutritional requirements, especially for iron, due to the abrupt growth in this age group.
The present study showed no significant differences in the prevalence of preterm birth between the young/middle-aged and older adolescents. Similarly Zhang et al. (2020) found that women aged 10–19 years had a higher risk of preterm delivery compared to women aged 20–34 years; however, they failed to find a significant difference in the level of risk between young adolescents (10–17 years) and older adolescents. Moreover, Heija et al. (2016) found no significant differences in the prevalence of very preterm birth <32 weeks between early teenage pregnancies (14–16 years) and late teenage pregnancies (17–19 years) (Abu-Heija et al., 2016). At the same time, several researchers have reported that young adolescents were more likely to have preterm births (Akseer et al., 2022; Ambia et al., 2023; do Vale de Almeida et al., 2020; Ergen et al., 2017; Traisrisilp et al., 2015). A higher preterm birth rate in young adolescents may be due to changes in the hormonal milieu and increased uterine sensitivity to the circulating hormones (Perez et al., 2020), but it could also be influenced by other ethnic and sociodemographic factors.
The rates of cesarean deliveries in this cohort were not significantly different between the young/middle-aged group and the older group. Elsewhere, it has been reported that the cesarean delivery rate is significantly lower in adolescents than in adults (Ergen et al., 2017; Indarti et al., 2020; Katz Eriksen et al., 2016). In Karachi, Pakistani adolescents below 17 years of age had a 29% less chance of cesarean delivery compared to adults and older adolescents (Amerjee et al., 2020). Likewise, another retrospective cohort study conducted in 2015 concluded that the cesarean section rate was significantly lower in adolescent mothers ≤15 years of age compared to their older counterparts and adults (Traisrisilp et al., 2015).
The present study showed no difference in perinatal outcomes in younger adolescents compared to older adolescents. In contrast, several previous studies have reported worse perinatal outcomes in younger adolescents compared to older adolescents (Alves et al., 2012; Ambia et al., 2023; Ergen et al., 2017; Kumar et al., 2007; Zhang et al., 2020). These findings were expected in this case, since there was no difference in the prevalence of preterm labor between the two groups.
Poverty, religion, cultural traditions, and the legality of child marriage are the most important drivers that encourage early marriage in different Sudanese communities. It is important to consider that adolescent girls who choose to become mothers may differ from those who are forced along this path. Accordingly, stress and social support may confound obstetric and perinatal outcomes. Psychosocial factors should be parallelly evaluated along with age when comparing obstetric and perinatal outcomes among different adolescent age groups.
The Study’s Strengths and Limitations
This study's strengths include its specific focus on an understudied population (younger vs. older adolescents in eastern Sudan) and its direct comparison of obstetric and perinatal outcomes between these two groups. This addresses a gap in existing research on adolescent pregnancy.
The main limitation of this research is that it was a single-center study, and the results might not be representative of other parts of Sudan. Also, this was a facility-based study and thus might not reflect what is going on in the community in general. In addition, there are other obstetric and perinatal outcomes that were not investigated, which may have significantly different rates between the adolescent age groups. Moreover, all the teenage women in this study were married, as pregnancies outside wedlock in Sudan are usually unsafely terminated outside hospitals, so any further studies should also consider the implications of this cultural phenomenon.
Implication for Practice
This study suggests that in Gadarif, nurses shouldn't assume younger adolescents (13–17 years) face inherently worse obstetric or perinatal outcomes than older ones (18–19 years) based solely on age. Instead, focus on individual risk factors and providing comprehensive care. Tailored health education, perhaps addressing the observed lower education levels in younger mothers, is a key to improving overall outcomes for all pregnant adolescents.
While this study found no significant differences in most obstetric and perinatal outcomes between younger and older adolescents in Gadarif, it highlights crucial areas for future focus. A key recommendation is to address the educational disparity observed, as younger adolescents had significantly lower education levels. Interventions promoting continued schooling or tailored educational support for pregnant adolescents could improve broader life outcomes, even if direct pregnancy complications appear similar. For future research, it's imperative to conduct larger, multicenter prospective studies that include a wider range of socioeconomic and nutritional factors. Given the known association of hormonal changes with preterm birth, future studies in this region should incorporate biochemical analyses to explore the role of specific hormones (e.g., progesterone, cortisol, placental hormones) in driving preterm labor among adolescent mothers. This would provide a more nuanced understanding beyond demographic comparisons.
Conclusion
In spite of the observed high rate of neonatal mortality, the analysis of the data obtained from young/middle-aged adolescent and older adolescents revealed no significant differences between the two groups regarding their obstetric and perinatal outcomes. We think that the high maternal and perinatal mortality rates should, however, be further investigated.
Footnotes
Acknowledgements
We would like to thank women who participated in the study.
Ethical Considerations
The study received ethical approval from the Research Board of the Faculty of Medicine, University of Gadarif, Sudan (reference number 2021, #6). Also, the approval of the hospital manager was obtained.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the present study's findings are available from the corresponding author upon reasonable request.