
Abstract
Introduction
One of the primary responsibilities of the nursing profession is the ability to communicate, report, take reports, and record data. The nursing report is the official exchange of written or verbal information between nurses at the end of each shift. In addition to recording the written report of nurses, the oral report is a method of communication whose purpose is to convey vital and crucial information about patients’ medical care (Salimi et al., 2013).
As mentioned, one of the practical reports of nurses is the work-shift delivery report, in which the nurse responsible for the patient provides a summary of the patient's activities and condition before leaving the unit to rest or deliver his or her shift. A work shift delivery report is one of the most prevalent and widespread methods of reporting to members of the healthcare team (Yuliyanti et al., 2020).
Off-going and oncoming nurse handoffs have been described in the literature as a technique for ensuring safe continuity of care and the implementation of optimal patient care by sharing vital patient information, responsibility, and accountability. Communication is essential in providing safe patient care, especially in the nursing profession, where nurses must communicate effectively, record information, and report it efficiently (Riesenberg et al., 2019). Handover is an essential part of nursing communication and a key factor in the continuity of care. It is expressed as the interchange of patient data among healthcare providers, along with the transfer of responsibility and accountability, and thus must be very well communicated (Trossman, 2019). It is critical to foster patient safety and care quality by providing accurate and complete information from one shift's nurses to the next work shift (Yuliyanti et al., 2020).
Review of Literature
Shift statements are the primary vital communication means for sharing important evidence about each patient with other members of the health team (Shahid & Thomas, 2018). It is also known as handover, nursing, change-of-shift, inter-shift report, sign-out, or sign-off (Kitson et al., 2014). During communication swapping between nurses (nurse-to-nurse), the outgoing nurse provides critical information regarding patient lab results, medication, new counsel from other specialties, and changes in the patient's condition. Hence, the exchange of such information must be accurate and complete (Vines et al., 2014). Thus, standardization of this process may improve its effectiveness (Estrella, 2016).
Reporting errors to supervisors and disclosing their consequences to patients and their families is considered error communication (Hendy et al., 2023). It makes a substantial contribution to the prevention of errors and the enhancement of safety. Many factors affect error communication; some allow it, while others forbid it. The culture of error communication and the consequences of error communication for the nurse and the patient, besides individual and professional characteristics, including ethical attributes and interprofessional relationships, all impacted this process (Tindle et al., 2020). Errors pose ethical quandaries for nurses, forcing them to assess error consequences and reveal or conceal them based on their findings. Creating a supportive environment for nurses, setting clear mistake communication methods and guidelines, and providing them with education about ethical practice principles are all things that health authorities may do to encourage them to communicate their errors (Ghezeljeh et al., 2021).
Nevertheless, the handover from one health care member or group to another is susceptible to failures of communication (Müller et al., 2018). This could be due to several factors in the healthcare setting. For example, the increasing number of carers providing care for patients due to increased specialty referrals led to more frequent handovers and errors during communication (McKechnie, 2015; Wheeler, 2015). Another possible factor contributing to the failure of communication is the frequent changes in care level and personnel, with possible loss of information (Arora & Farnan, 2019). Nurses are often at the center of the handoff crisis, being involved daily. Hence, they need the training to acquire the necessary knowledge and develop skills and competencies to use valid tools to improve handover quality (Drach-Zahavy & Hadid, 2015).
The Situation, Background, Assessment, and Recommendation (SBAR) tool, initially developed by the US Navy, was promulgated by the Institute for Health Promotion as a simple and efficient tool for shift reporting (Pope et al., 2008). This tool minimizes communication errors during handover through standardized communication (Callaway et al., 2018). It helps nurses report accurate and complete information that is well organized without unnecessary details (Whittingham & Oldroyd, 2014). The incoming nurse or shift gets a full and clear clinical picture of patient status (Espinoza, 2022).
Nursing care is extremely complex and vital, and it is very challenging and difficult to communicate information using standard methods. Unfortunately, nurses do not approach their reports with a systematic and integrated approach. Consequently, one of the problems and challenges of shift reporting is the nurses’ inability to effectively communicate information. Taking into account the clinical repercussions that poor information transfer has on patients when weak information transfer is present, the current study aimed to investigate the effect of a shift reporting training program using the SBAR tool on nurses’ knowledge and practice and their perception of shift handoff communication in non-critical departments at Suez Canal University Hospitals.
Methods
Design. This study was conducted using a one-group quasiexperimental research design with pre-post evaluation.
Setting. This study was held in the noncritical departments at Suez Canal University Hospitals. Medical, surgical, obstetrics, pediatrics, orthopedics, and urology departments were there.
Subjects—Sampling and sample size. All staff nurses (n = 105) working in the study settings constituted the sampling population. Having at least one year of experience reporting work shifts and distributing them to other peers was the only requirement for inclusion in the study population. Based on moderate effect size (0.50) and an estimated odds ratio of 2.5, the sample size was calculated to imply increases in nurses’ knowledge, practice, and perception (Chinn, 2000). The needed sample size was 80 participants using the Open-Epi software program for a sample size of two proportions at 95% confidence level and 80% power. This was increased to 83 to compensate for an expected dropout rate of around 5%. The staff nurses who met the set criteria were sequentially recruited into the sample to achieve the needed sample size.
Tools for Data collecting. A knowledge questionnaire, an observation checklist, and two perception scales were utilized in data collection.
First Tool—Knowledge Questionnaire. This was divided into two parts.
Part-I (Demographic characteristics): Included age, gender, nursing qualification, years of experience, work department, residence, marital status, and previous training (Mohamed et al., 2022). Part-II (Knowledge questionnaire): The researcher established this based on El sayed, 2013 to assess staff nurses’ knowledge about SBAR shift reports earlier and later implementing the program. It comprised 25 multiple-choice questions concerning SBAR shift reports covering communication (7 items), reporting (6 items), and SBAR shift reports (12 items).Scoring: Each question received a score of “1” for correct answers and “0” for incorrect answers. The scores of the items were added together for each area of knowledge and the overall questionnaire, and the total was divided by the number of items, yielding a mean score for the portion. These scores were converted into percent scores. If the percent score was 60 percent or higher, the knowledge was regarded as satisfactory; if it was less than 60 percent, it was considered unsatisfactory. This is the accepted cutoff point for nursing school acceptance. Second Tool—Experimental checklist. The researcher created this based on El sayed, 2013 to evaluate nurses’ practice of shift handover. It consists of 35 items grouped under three sections, namely the preparation of report before handover (4 items), handover process of the report (6 items), and exchange of SBAR shift report contents (25 items). There are four sub-sections in this section: Situation (5 items), Background (4 items), Assessment (9 items), and Recommendation (7 items).Scoring: Each item was given a “0” if not completed and a “1” if completed. The scores of the items were added up for each section and the entire scale, and the total was divided by the number of items, yielding a mean score for the section. These results were converted to percentile rankings. The practice was considered adequate if 60% or more scores were achieved and inadequate if less than 60% were completed (22). Third Tool—Handover Perception Scale for Nurses: This consisted of two subscales, namely the Handover Evaluation Scale (HES) and the Nurse Handoff Communication Scale (NHCS).
HES. This scale was developed by O’Connell et al. (2014) to evaluate nurses’ perceptions of the quality of handoff in their hospitals. It was translated to Arabic utilizing the translate-back-translate method for validity. This scale gives 14 items on a 7-point Likert scale: “strongly agree, agree, slightly agree, neither agree nor disagree, slightly disagree, disagree, and strongly disagree” These consist of three subscales: 6 items for quality of information, 5 items for interaction and support and 3 items for efficiency.Scoring: Each item has a score ranging from 0 to 6 for “strongly disagree” and “strongly agree” responses. Scores of the subscale and total scale items were summed-up, then divided by item number, resulting in a mean score for the part. Hence a higher score indicates a higher perception by transforming these scores into percent scores; in similarity with the cutoff point of the observation checklist, a high nurse's perception is achieved by a 60% or higher score, while the low one is achieved by a score less than 60%. NHCS. This scale was developed by (Rowe, 2015) based on (Böhmer et al., 2012) and (McDowell & McComb, 2014) to evaluate both nurses’ satisfaction and perception of professional practice of nurse-to-nurse shift handoff communication. Also, it was converted to the Arabic language utilizing the translate-back-translate procedure for validity. 19 items were involved in this scale, with a 5-point Likert scale varying from “strongly agree” to “strongly disagree.” These are classified into three categories: general (7 items), outgoing nurse (6 items), and incoming nurse (6 items).Scoring: Each item response was scored from “1” to “5” for the responses from “strongly agree” to “strongly disagree.” As the same in the previous scale, for each category and the total scale, the mean score resulted from dividing the total score by the number of items, and then by transforming these scores into percent score and in similarity with the cutoff point of the observation checklist, high nurse's perception achieved by 60% or higher score, while the low one achieved by a score less than 60%.
The tool reliability was completed by looking at their internal consistency. With Cronbach Alpha ratings of 0.85 for the SBAR practice scale and 0.84 for the communication scale, they indicated excellent reliability. The perception tool has documented high reliability, with Cronbach's alpha coefficient reaching 0.86 (O’Connell et al., 2014).
Fieldwork
Assessment Phase. The researchers obtained official permissions and ethical approvals to perform the study and fine-tuned the data collection tools following the pilot. Data were then collected before the training using the three tools to assess nurses’ knowledge, practice, and perception of shift handoff communication. These data served as a pretest, as well as in identifying nurses’ learning needs. The time duration to fill the self-administered questionnaires for each nurse was 15–20 min, and 25–30 min to observe practice during the work shift delivery report. This was done based on the SBAR checklist for three different work shifts for each nurse and taking their average. Then, a schedule and venue were set to implement the training program after consultation with the nursing director and coordination with the head nurses of the study departments.
Planning phase. The training program was prepared based on the identified needs and in view of the most recent pertinent literature. It consisted of 18 training hours, 12 theoretical and 6 practicals. The theoretical part covered communication, documentation, shift reporting, and the SBAR shift report, including its definition, benefits, and process. The valuable part included training in applying shift reports using the SBAR tool. The teaching methods were interactive lectures, group discussions, and practice using role-playing and training scenarios. Teaching aids included data show, blackboard and chalk, and SBAR form. A booklet was prepared by the researchers in Arabic language and attached with figures and illustrations in addition to SBAR forms to help attending nurses during and after training.
Implementation phase. The program venue was in the educational classrooms at the educational section in Suez Canal University Hospitals. Participating nurses were divided into six groups according to their work departments. It was implemented on two nonconsecutive days per week and three nonconsecutive weeks. Each day included three hourly sessions, two theoretical and one practical. The program sessions lasted from 10:00 am to 1:00 pm. Each attending nurse received a knowledge booklet and a lecture printout by the end of each session. During sessions, they were encouraged to ask questions and give feedback. In the practical sessions, each nurse was asked to fill a template for reporting the work shift using the four elements of the SBAR tool after the applied training provided by the researchers.
Evaluation phase. The evaluation of the efficiency of the training program was done through an immediate post-test and a follow-up test three months after the end of program implementation. These were done using the same tools and methods used in the pretest.
Ethical Consideration
This study protocol was approved by the ethical committee of the faculty of nursing at Suez Canal University with code 118–8/2021. Consent was obtained from each nurse before participation. The purpose of the study was explained in written words in the introduction part of the survey. In addition, participants who agreed to participate in the study were assured that all information obtained would be kept confidential and there were no personal identifiers in the questionnaire. They were notified that they had the right to withdraw from the study at any time.
Statistical Analysis
It was performed using SPSS 20.0 statistical package. Qualitative data were presented as frequencies percentage using descriptive analysis, while quantitative data were presented as means, standard deviations, and medians. For comparing categorical data, chi-square or Fisher exact tests were used, as well as Spearman's rank correlation for the relationships between quantitative and ranking variables. Using multiple regression analysis, the independent predictors of knowledge, practice, and perception scores were identified. Statistical significance was tested at a p-value <.05. statistical analysis
Results
The study sample consisted of 83 diploma nurses; a significant percentage of the study sample (85.5%) was females, ranging from 22 to 45 years. About 70% of the study sample has experience of less than 10 years. Slightly more than half of them (55.4%) were married and residing in rural areas. Only 9.6% reported having attended training in SBAR, as mentioned in Table 1.
Demographic and Job Characteristics of Nurses in the Study Sample (n = 83).

As illustrated in Table 2, nurses’ preintervention knowledge was unsatisfactory, particularly regarding SBAR (7.5%). The postintervention phase revealed significant improvements in their adequate total knowledge from 4.8% to 92.8% (p < .001), with a slight decline in the follow-up phase (74.7%).
Nurses’ Knowledge and Practice of Situation, Background, Assessment, and Recommendation (SBAR) Throughout Intervention Phases.
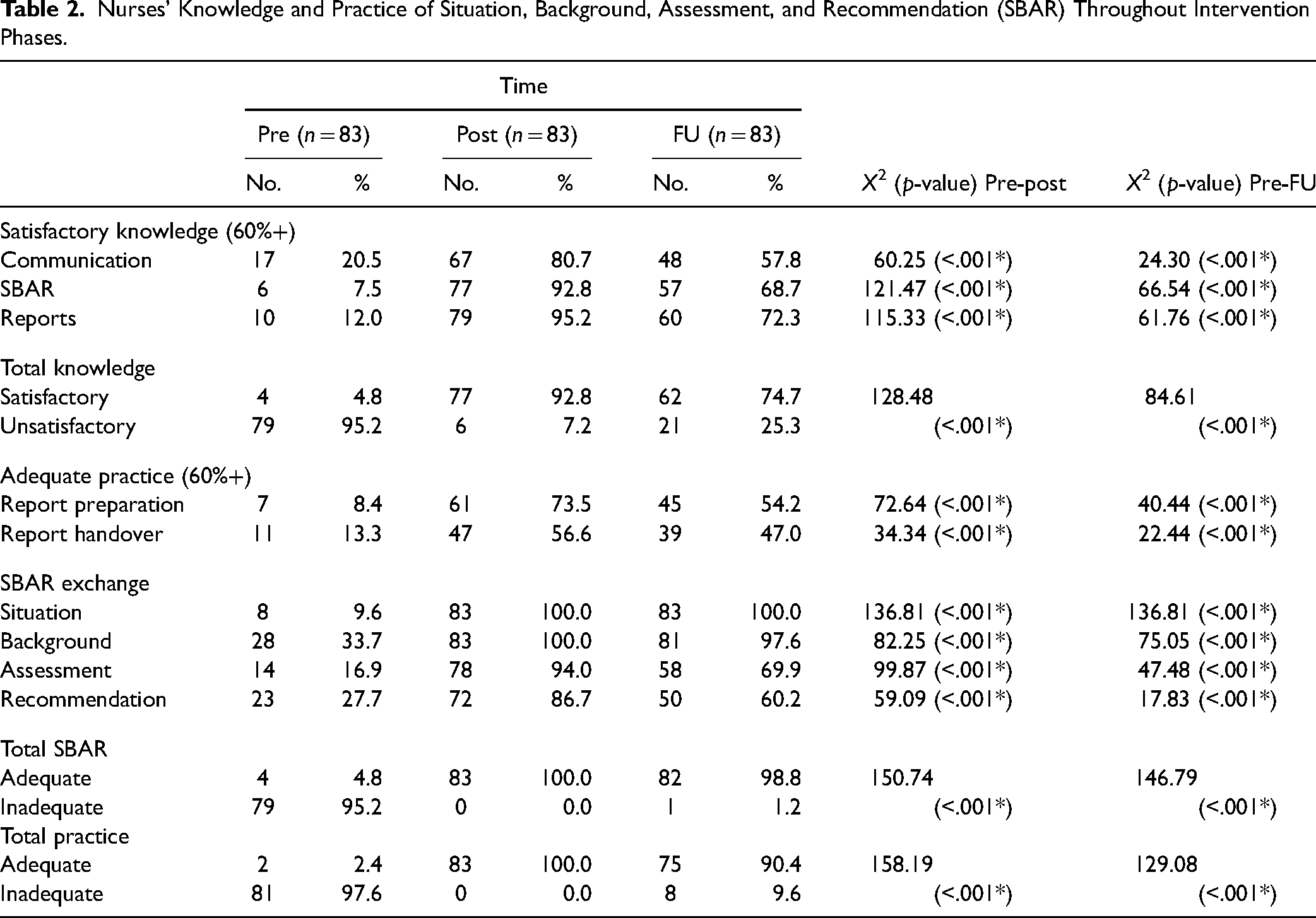
Similarly, the table indicates that their practice of SBAR and total practice mainly were inadequate in the pre-intervention phase, with only 4.8% and 2.4% having adequate practice, respectively. These significantly improved in the postintervention phase, reaching 100%. They slightly decreased to 98.8% and 90.4% during the follow-up phase, respectively.
Regarding nurses’ perception of shift handover, Table 3 points to the generally low perception of the process and related communication at the preintervention phase. Thus, only 10.8% of them had a high perception of the process and 44.6% of related communication. The perception of the process showed significant improvement in the postintervention phase reaching 45.8% (p < 0.001) but decreased to 21.7% in the follow-up phase. Meanwhile, the perception of related communication reached 100% during the post and follow-up phases (p < .001).
Nurses’ Perception of Shift Handover Process and Related Communication Throughout Intervention Phases.
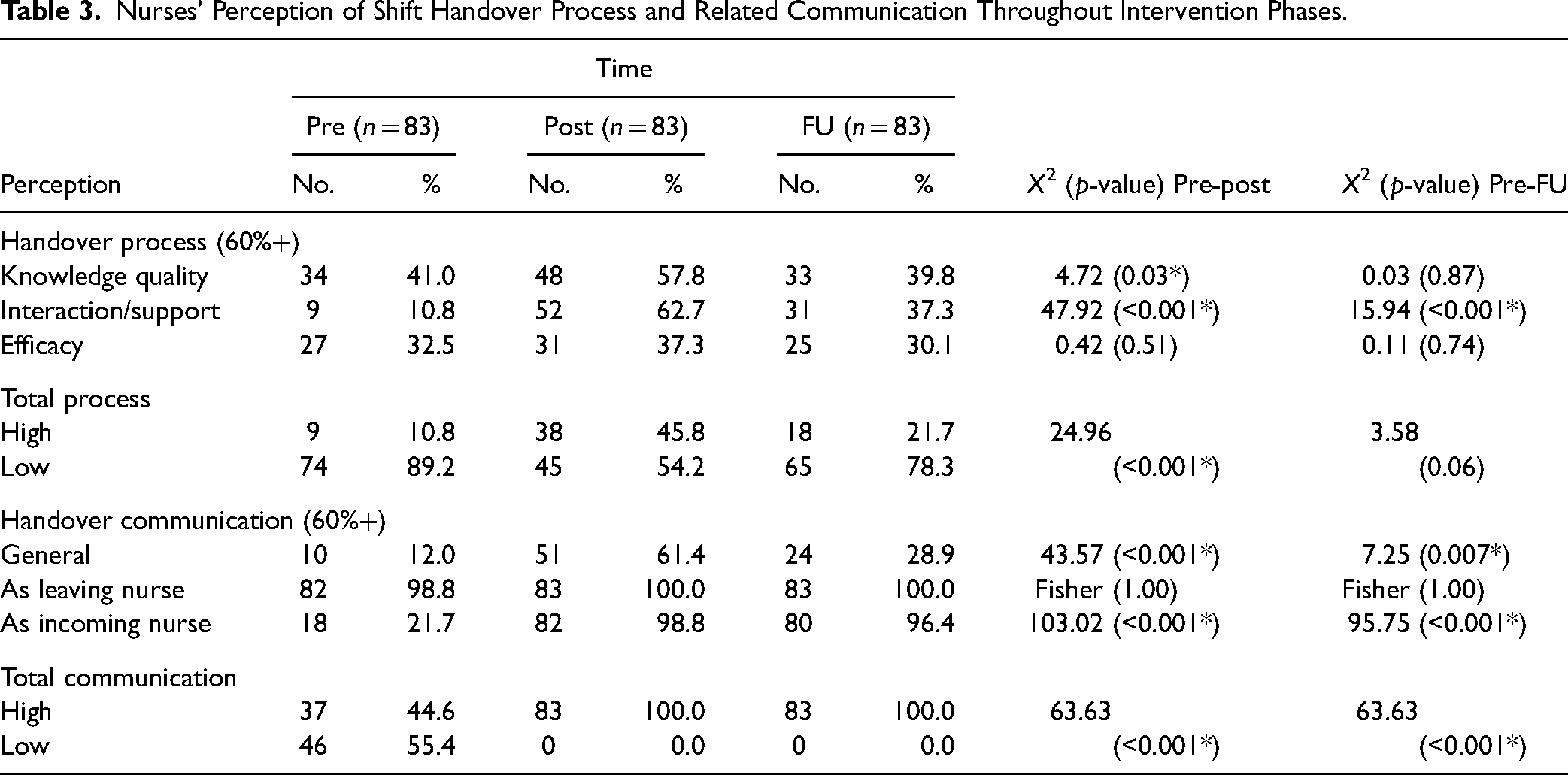
Table 4 shows a significant moderate positive correlation between nurses’ scores of knowledge and SBAR practice (r = .661) and a weak positive correlation between their perception of the handover process and related communication (r = .349). Meanwhile, none of these scores significantly correlated with nurses’ age or experience years.
Correlation Matrix of Nurses Scores of SBAR Knowledge, Practice, and Perception of the Process and of Related Communication, and Their age and Experience.

(**) statistically significant at p< .01.
According to multivariate analysis (Table 5), the study intervention was the main statistically significant independent positive predictor of nurses’ knowledge and practice scores and being married and working in urology/orthopedics departments. The knowledge model explains 58% of the variance in its score. The model also includes the knowledge score as a positive predictor for the practice score, and it explains 85% of the differences in the practice score.
Best Fitting Multiple Linear Regression Model for the Knowledge and Practice Scores.

Concerning nurses’ scores of process perception, Table 6 indicates that the knowledge and practice scores were positive predictors. Conversely, working in urology/orthopedics departments was a negative predictor. The model explains 17% of the differences in the process perception score.
Best Fitting Multiple Linear Regression Model for the SBAR Process.
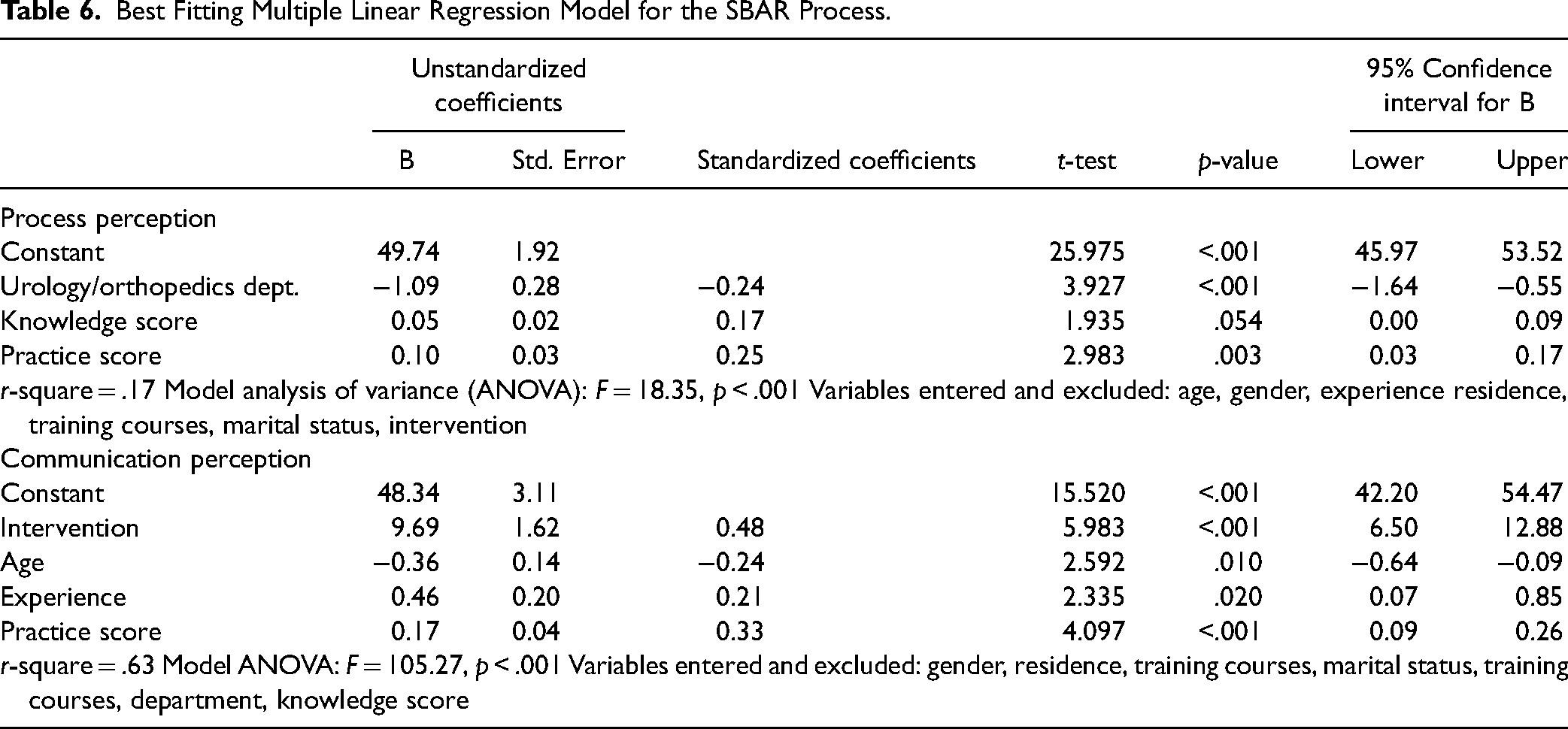
As for nurses’ scores of communication perception, the same table shows that intervention was the main positive predictor as the practice score and experience years. Conversely, age was a negative predictor. The model explains 63% of the variation in the communication perception score.
Discussion
This study was conducted to evaluate the research hypothesis that, after adopting an SBAR shift report training program, nurses’ understanding and practice of SBAR shift reporting and their impression of shift handoff communication would greatly improve. The study results demonstrated that the percentages of nurses having satisfactory knowledge, adequate practice, and high perception were significantly higher in the post-intervention and follow-up phases, with some declines at follow-up. The findings lead to the acceptance of the set research hypotheses.
Before the intervention, the current study's findings demonstrated that nurses’ awareness of handoff shift reporting was lacking. These results may be due to a lack of training, as shown by the tiny percentage reporting previous related activity. A similar situation of deficient nurses’ knowledge of effective handover was highlighted by Yu and Kang (2017) in a study in South Korea.
The implementation of the study intervention led to significant improvements in attending nurses’ knowledge immediately after the program, and this continued through the three-month follow-up phase. These results are supported by a study on Jordanian nurses who reported significant improvements in their knowledge following an SBAR training intervention (Dalky et al., 2020). Similarly, Ghosh et al. (2021), in a study of the impact of a structured clinical handover protocol on communication in India, demonstrated significant improvement in nurses’ knowledge of SBAR shift reporting after implementing their intervention.
Concerning nurses’ practice of SBAR, the study results revealed a moderately significant positive correlation between nurses’ knowledge scores and SBAR practice. Moreover, the improvement in their knowledge scores was a significant positive predictor of the improvement in their practice score in the multivariate analysis. In line with this, a study in Iran found that nurses’ practice in the use of SBAR was widely variable and tended to be most inadequate regarding its “background” component (Beigmoradi et al., 2019). Also, in agreement with this, a training intervention in handover led to significant improvement in Canadian nurses’ practice, with increases in practice adequacy from 4% in the pre-intervention phase to 79% in the post-intervention phase (Abela-Dimech & Vuksic, 2018).
According to the nurses’ perception, the results revealed a generally low perception of the shift handover process and related communication before implementing the study intervention. Similar low perceptions of handover communication were demonstrated in the qualitative research of nurses in a pediatrics department in an American hospital (Reese et al., 2016).
Furthermore, our findings revealed significant improvements in nurses’ perceptions of handover communication and, to a lesser extent, process perceptions, which declined to borderline significance at the follow-up phase. These results are consistent with two South Korean studies that reported a similar success of a training intervention in improving nurses’ perceptions of handover communication (Do & Shin, 2019; Uhm et al., 2019).
Other studies, including Sears et al. (2014), Randmaa et al. (2014), and Cornell et al. (2014), showed that using the SBAR communication tool has been very effective in improving the level of patient safety, reducing the time spent by nurses on shift delivery, and improving nurses’ professional relationships. Also, Inanloo et al. (2017) reported that using the shift work reporting method had a significant effect on the study participants using SBAR tool and improved their performance with regard to work shift delivery report.
Our study mentioned a significant positive correlation among nurses’ knowledge and SBAR practice (r = .661) and a weak positive correlation between their perception of the handover process and related communication (r = .349). Meanwhile, none of these scores significantly correlated with nurses’ age or experience years. These results, supported by Chiew et al. (2019), revealed that there was a statistically significant relationship (p = .000) between perception and compliance on ISBAR tools.
According to multivariate analysis, the knowledge score was a positive predictor for the practice score, and it explains 85% of the differences in the practice score. Also, marriage had a negative predictor for the practice score. These results are consistent with the study by Hendy et al. (2022), which stated that there was a high positive correlation between nurses’ practice and knowledge.
Multiple linear regression model for knowledge; the study intervention, along with being married and working in urology or orthopedic departments, was the main statistically significant independent positive predictor of nurses’ knowledge and practise scores. The knowledge model explains 58% of the variance in its score. These results, reported by Abdel-Aal et al. (2020), stated that the staff nurses in the study setting had deficient knowledge and inadequate performance in communication and shift report handover. There was a significant positive correlation between the knowledge score and the performance score.
Concerning nurses’ scores of process perception, the evidence indicated that the knowledge and practice scores were positive predictors. Conversely, working in urology or orthopedic departments was a negative predictor. These results are inconsistent with the study by Nagammal et al. (2016), who reported that there was no statistically significant difference between the overall perception scores observed among participants with differences in age group, gender, and the total number of years of experience in nursing.
As for nurses’ scores of communication perception, the intervention was the main positive predictor, followed by the practice score and experience years. Conversely, age was a negative predictor. The model explains 63% of the variation in the communication perception score. In line with this, a significant relationship between age and the resistance to change was previously demonstrated (Mousavizadeh & Banazadeh, 2020).
Strengths and Limitations
The study results were based solely on the perceptions of 83 staff nurses. This study did not evaluate the effectiveness of the SBARtool where patient outcomes were concerned; future research could address this.
Implication for practice
Conclusions
Using the shift work reporting method had a significant effect among the study participants using SBAR tool and improved their knowledge, practice, and perception of shift handoff communication. Furthermore, this study recommends comprehensive training courses in SBAR use in shift reporting for nurses. Standardized SBAR shift reporting should be applied in all departments and units at Suez Canal University Hospitals and similar settings. A future study of the feasibility and effectiveness of integrating electronic SBAR shift report in hospital is proposed. Therefore, this research is an evidence of the effectiveness of SBAR training program in the development of nurses’ capabilities in the field work shift delivery report in hospitals.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Dean of the Faculty of Nursing, Suez Canal Univ., requested official permission to perform the study in Suez Canal University Hospitals. The aim of the research and data collection tools was attached in the official request to get approval and cooperation for program implementation and data collection. The director provided permission and directed the nursing hospital director to facilitate the researchers’ mission. The Scientific Research Ethical Committee granted ethical permission.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Before giving their informed consent, participants were informed about the study's purpose and procedures. They were notified about privacy for any obtained information and were informed about their rights to decline or withdraw at any moment. No harmful effect was entailed resulting from the study procedure on participants.