
Abstract
Background
Ergonomic hazards are a growing concern among nursing professionals due to their association with musculoskeletal disorders and occupational injuries.
Objective
This study aimed to assess the knowledge, perceptions, and practices of undergraduate nursing students regarding ergonomic hazards during clinical training.
Methods
A descriptive cross-sectional study was conducted among nursing students at the University of Bisha, Saudi Arabia. Data were collected using a structured, self-administered questionnaire and analyzed using descriptive and inferential statistics.
Results
Students demonstrated moderate knowledge about ergonomic hazards and generally positive perceptions of ergonomic importance. However, their actual ergonomic practices were inconsistent, especially during clinical procedures involving patient handling.
Conclusion
While students are aware of ergonomic risks, gaps in practice highlight the need for targeted training. Ergonomic education should be incorporated into nursing curricula to promote safe clinical behaviors and prevent injuries.
Introduction
Nursing is a physically demanding profession characterized by prolonged standing, repetitive movements, and manual patient handling, all of which contribute to a high risk of work-related musculoskeletal disorders (WMSDs) among healthcare workers (Krishnanmoorthy et al., 2025)
Although ergonomic training is recognized for reducing occupational injuries, limited attention has been given to undergraduate nursing students’ understanding of ergonomic risks prior to entering the workforce (Choi et al., 2020).
During clinical placements, nursing students often undertake physically strenuous tasks without formal instruction in ergonomics, making them vulnerable to developing unsafe habits and potential injuries (Garg & Kapellusch, 2020). Early integration of ergonomic training has been shown to enhance adherence to safe practices and reduce musculoskeletal injuries (Waters et al., 2020). Despite this, many nursing programs lack structured curricula addressing body mechanics, injury prevention, and equipment use (Kandasamy et al., 2024). Despite recognition of ergonomic training's importance, limited evidence exists regarding undergraduate nursing students’ knowledge, perceptions, and self-reported practices of ergonomics, particularly in Middle Eastern contexts. Few studies have examined how demographic factors influence these domains, and evidence on the integration of ergonomics into undergraduate nursing curricula remains sparse.
Understanding students’ awareness of ergonomic hazards is essential for identifying educational gaps and implementing improvements. This study aims to assess nursing students’ knowledge, perceptions, and self-reported practices regarding ergonomic hazards and to evaluate the influence of demographics and prior training on their competence in this area.
Review of Literature
Ergonomic Hazards in Nursing Education
Nursing students frequently engage in physically demanding tasks such as patient lifting, prolonged bending, and working in awkward postures during clinical training, placing them at risk for musculoskeletal discomfort similar to that experienced by professional nurses (Johnson & Lee, 2021). However, many students lack formal ergonomic training, leaving them unprepared for injury prevention (Smith et al., 2022). In Saudi Arabia, Al-Mutairi (2023) reported that only 35% of nursing students had prior ergonomic knowledge, and more than 60% experienced back pain due to incorrect lifting techniques.
Benefits of Early Ergonomic Education
Integrating ergonomic education early in nursing programs improves safety outcomes and confidence in patient handling (Garg & Kapellusch, 2020). Simulation-based learning and hands-on workshops have been particularly effective in translating theoretical knowledge into practice (Waters et al., 2021). A recent cross-sectional study by Alsharari and Kerari (2024) demonstrated that structured ergonomic training significantly reduced musculoskeletal complaints among nursing students during clinical placements, with reported reductions approaching 50%.
Curricular Gaps and Recommendations
Despite growing awareness, ergonomic training remains inconsistently implemented in nursing curricula. Some institutions address body mechanics within broader clinical skills modules, but many fail to offer dedicated instruction on posture correction and injury prevention strategies (Choi et al., 2020). The World Health Organization (WHO) and World Health Organization (WHO), 2020 Occupational Safety and Health Administration (OSHA) emphasize the need for systematic ergonomics education in healthcare disciplines (OSHA, 2020). Strengthening ergonomics instruction through evidence-based guidelines, practical skill assessments, and reinforcement in clinical environments is vital (Kuorinka et al., 1987).
Study Objective
This study aimed to assess undergraduate nursing students’ knowledge, perceptions, and self-reported practices regarding ergonomic hazards during clinical training, and to explore associations with demographic factors.
Methods
Study Design
A descriptive cross-sectional study design was employed to assess the knowledge, perceptions, and self-reported practices of undergraduate nursing students regarding ergonomic hazards. This design is appropriate for capturing data at a single point in time, offering a comprehensive overview of students’ current awareness and behavior patterns (Al-Mutairi, 2023). It also helps identify potential knowledge-practice gaps, which may inform targeted educational interventions. This cross-sectional study adheres to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines; the completed checklist is provided in Supplementary Appendix S1.
Study Setting
The research was conducted at the Nursing Department, College of Applied Medical Sciences, University of Bisha, Saudi Arabia. The department provides both theoretical instruction and clinical training, exposing students to real-world healthcare environments where ergonomic risks are prevalent. Eligible participants were undergraduate nursing students who had completed at least one clinical training course and provided informed consent. Students without prior clinical training experience, those diagnosed with musculoskeletal disorders that could confound the results, and those who declined participation were excluded.
Study Population and Sampling
A convenience sample of 200 undergraduate nursing students across all academic levels (first to fourth year) was recruited for the study.
Sample Size Calculation
Sample size was calculated using G*Power 3.1.9.7 software, with the following parameters: Confidence level: 95% (α = .05), Power: 80% and Effect size: Medium (Cohen's d = 0.5)
Drawing from previous ergonomic awareness studies that used samples of 150–300 students (Choi et al., 2020; Smith et al., 2022), a target sample of 200 participants was deemed sufficient for robust statistical analysis. The target sample size was increased to 200 participants to account for potential non-response and ensure adequate statistical power for subgroup analyses.
Data Collection Instrument
A structured, self-administered questionnaire was developed based on established ergonomic assessment tools. The questionnaire drew upon the Nordic Musculoskeletal Questionnaire (NMQ; Kuorinka et al., 1987), OSHA ergonomic guidelines, and World Health Organization recommendations, with minor modifications to fit the undergraduate nursing context.
The instrument consisted of four main sections: a demographic profile (age, academic year, previous ergonomic training, and musculoskeletal discomfort); knowledge of ergonomic hazards (six multiple-choice questions on safe body mechanics and injury prevention, scored as 1 for correct and 0 for incorrect answers, categorized as good [5–6], average [3–4], or poor [0–2]); perceptions of ergonomic hazards (eight items measured on a 5-point Likert scale ranging from 1 = strongly disagree to 5 = strongly agree, with total scores classified as high [31–40], moderate [20–30], or low [0–19]); and self-reported ergonomic practices (four items rated on a 4-point scale from 1 = never to 4 = frequently, with total scores categorized as satisfactory [10–16] or unsatisfactory [0–9]).
The questionnaire was initially piloted among 20 students to assess clarity and reliability. Feedback was incorporated to refine the tool. Cronbach's alpha was calculated to assess internal consistency, with a threshold of ≥0.70 indicating acceptable reliability.
Data Collection Procedures
Data were collected in two sequential phases. In the first phase, which focused on instrument validation and ethical approval, authorization was obtained from the Institutional Review Board at the authors’ institution (Approval No.: [H-06-BH-087/(11/03/46)]). A pilot study was then conducted in March 2025 with 20 undergraduate nursing students to evaluate the clarity, content validity, and internal consistency of the questionnaire. Feedback from participants led to minor wording adjustments and reordering of certain items, and Cronbach's alpha values confirmed acceptable reliability (≥0.70) for all domains.
In the second phase, representing the main data collection, participants received a link to the questionnaire via Google Forms. Data were collected between March and April through institutional email and official student WhatsApp groups. The average completion time was 15–20 min. Participation was voluntary, no incentives were provided, and responses were anonymous.
Data Analysis
Data were analyzed using IBM SPSS version 25. Descriptive statistics, including frequencies, percentages, means, and standard deviations, were used to summarize the data. Inferential analyses were conducted using the Mann–Whitney U test to compare two independent groups, the Kruskal–Wallis test for comparisons across more than two groups, and Spearman's correlation to assess relationships among study variables. Statistical significance was set at p ≤ .05 (p < .01 was considered highly significant, p < .05 significant, and p ≥ .05 not significant). Potential confounders such as age, gender, and academic year were examined through subgroup analyses.
Reliability Testing
Cronbach's alpha values for internal consistency were as follows: Knowledge: 0.730, Perception: 0.766 and Reported Practices: 0.778
These values confirm the questionnaire's reliability across its domains.
Results
For clarity, detailed frequency distributions are summarized in Tables 1–5, while the narrative text highlights key findings.
Frequency Distribution of the Studied Sample According to Demographic Characteristics (n = 200).

Note. SD = standard deviation. Percentages are rounded to one decimal place. Missing data were handled using pairwise deletion. Bold values represent key summary measures and statistically significant results where applicable.
Frequency Distribution of Students’ Knowledge Regarding Ergonomic Hazards (n = 200).

Note. Correct answers scored 1, incorrect answers scored 0. Total score range 0–6, categorized as Good (5–6), Average (3–4), Poor (0–2). SD = Standard deviation. Percentages rounded to one decimal place. Missing data handled using pairwise deletion.
Students’ Perceptions Regarding Ergonomic Hazards (n = 200).
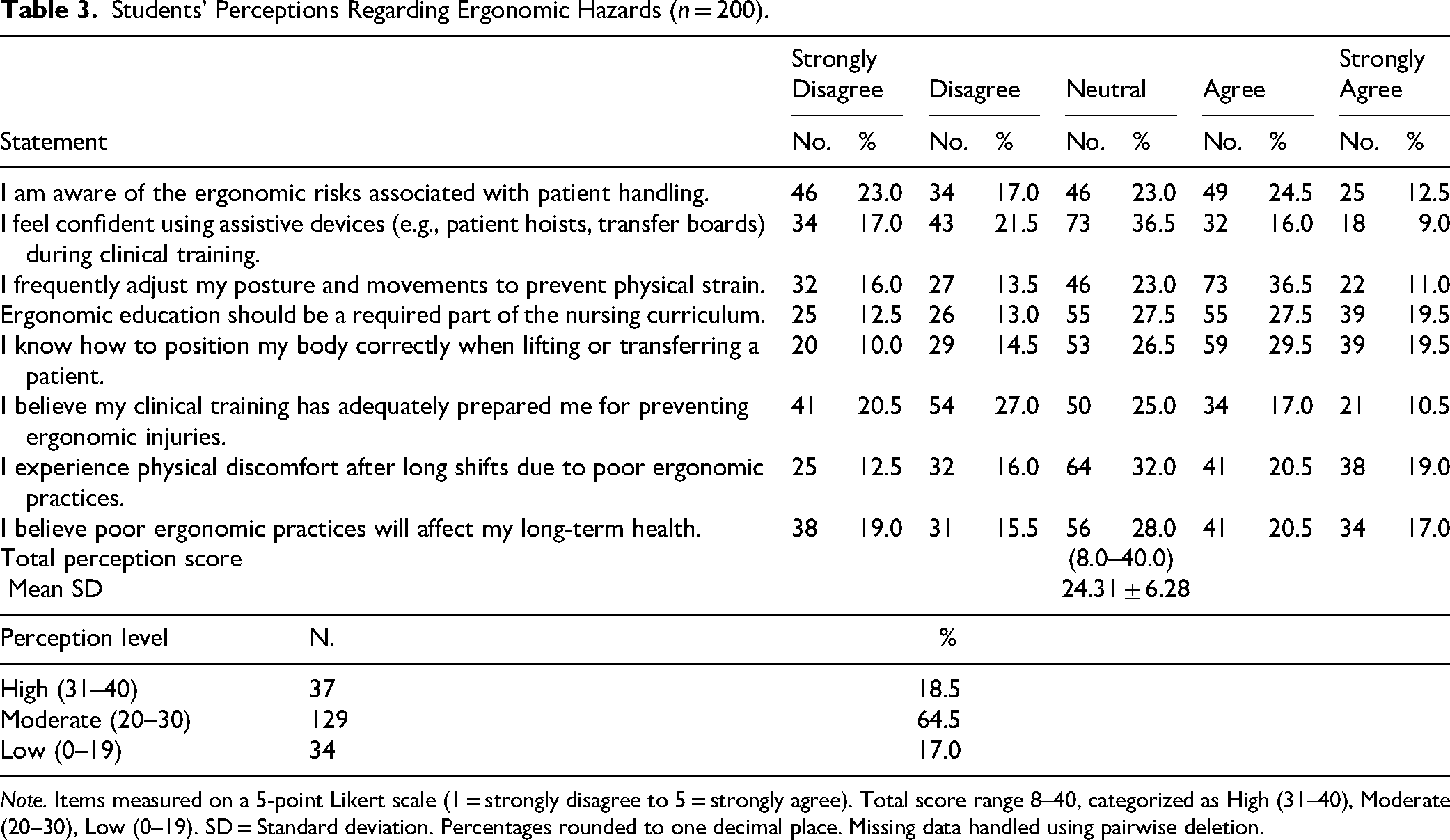
Note. Items measured on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree). Total score range 8–40, categorized as High (31–40), Moderate (20–30), Low (0–19). SD = Standard deviation. Percentages rounded to one decimal place. Missing data handled using pairwise deletion.
Students’ Self-Reported Ergonomic Practices (n = 200).
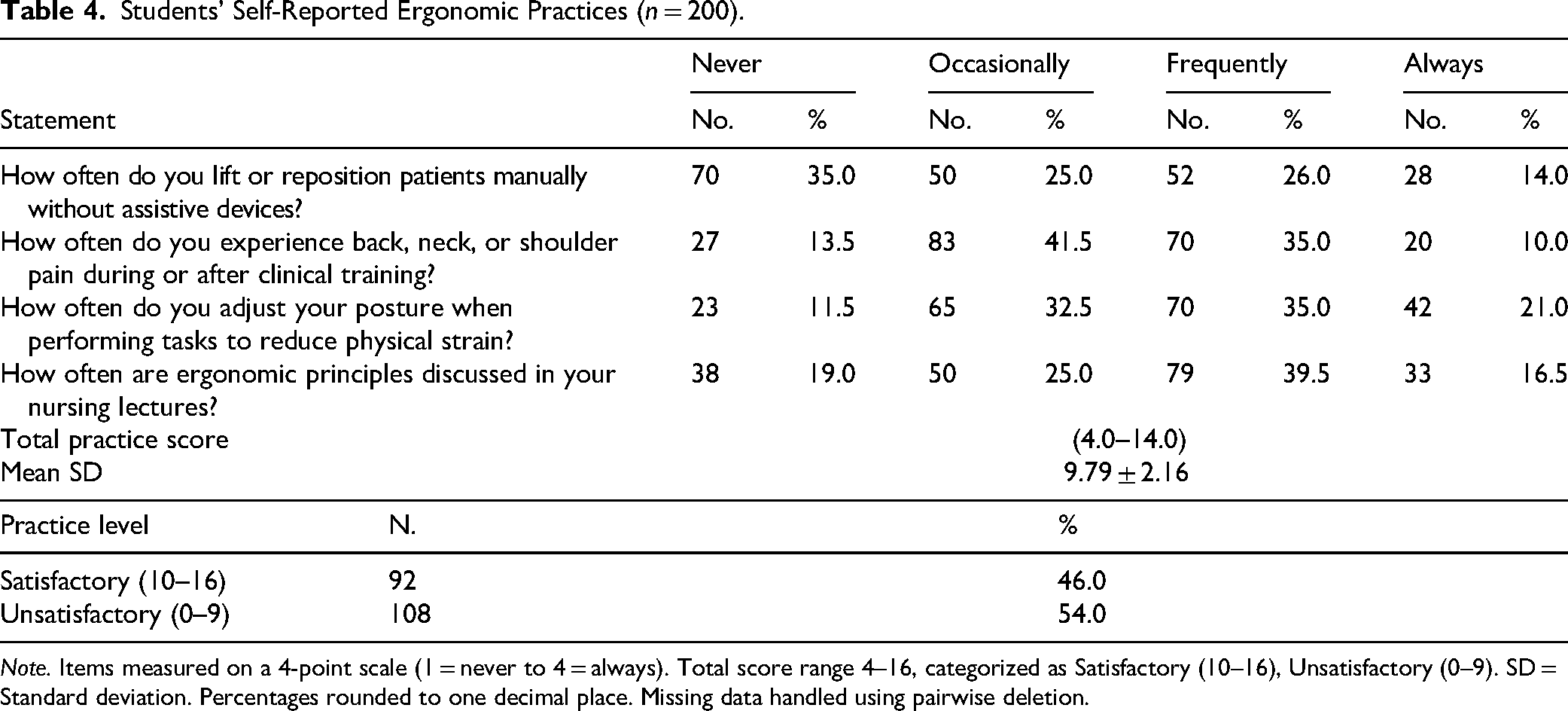
Note. Items measured on a 4-point scale (1 = never to 4 = always). Total score range 4–16, categorized as Satisfactory (10–16), Unsatisfactory (0–9). SD = Standard deviation. Percentages rounded to one decimal place. Missing data handled using pairwise deletion.
Relationship Between Students’ Demographic Characteristics and Total Knowledge, Perception, and Practice Scores (n = 200).

Note. Mean rank values calculated using *Kruskal–Wallis or Mann–Whitney U test. p < .05 considered significant; p < .01 highly significant. Missing data handled using pairwise deletion.
Table 1 summarizes the demographic characteristics of the 200 undergraduate nursing students. The majority were female (73.5%) and aged between 20 and 25 years (59%). Nearly half of the students (48%) were in their fourth academic year. While 69% reported having received some form of ergonomic training, only 52.2% of those received classroom-based instruction. About 65% experienced musculoskeletal discomfort following clinical training, most frequently in the lower back (44.6%), neck (24.6%), and shoulders (21.5%).
Table 2 presents participants’ responses to the six knowledge items. The mean knowledge score was 2.69 ± 1.80 out of 6. Only 21.5% demonstrated a good level of knowledge, while 51% showed average and 27.5% poor knowledge. Awareness was highest regarding the use of ergonomic equipment (51.5%) and the definition of ergonomics (51%), while lowest for posture-related items.
Table 3 outlines students’ perceptions toward ergonomic hazards. The mean perception score was 24.31 ± 6.28 out of 40, with 64.5% reporting moderate, 18.5% high, and 17% low perception. Confidence in using assistive devices was relatively low, with only 25% of students agreeing or strongly agreeing that they felt confident during clinical training. A total of 47.0% agreed or strongly agreed that ergonomic education should be a required part of the nursing curriculum (27.5% agree; 19.5% strongly agree), and 47.5% agreed or strongly agreed that they adjust their posture to prevent strain (36.5% agree; 11.0% strongly agree).
Table 4 displays students’ self-reported ergonomic practices. The mean practice score was 9.79 ± 2.16 out of 16, with 54% indicating unsatisfactory practices. A total of 65.0% reported manually lifting or repositioning patients without assistive devices (25.0% occasionally; 26.0% frequently; 14.0% always), and 45% reported experiencing pain during or after clinical training frequently or always. While 56% (35% frequently + 21% always) indicated that they adjusted their posture to reduce physical strain, 56% (39.5% often + 16.5% always) reported that ergonomic principles were discussed during lectures.
Table 5 shows the associations between demographic variables and KPP (Knowledge, Perception, and Practices) scores. Students aged >30 years and those in the fourth academic year had significantly higher scores across all domains (p < .001). Those who received prior ergonomic training also scored significantly higher. Conversely, students experiencing musculoskeletal discomfort had lower scores, suggesting a relationship between ergonomic competence and injury risk.
Table 6 summarizes the Spearman correlations between knowledge, perception, and practice scores. Positive correlations were found between knowledge and perception (r = .478), knowledge and practices (r = .384), and perception and practices (r = .381), all statistically significant (p < .001), indicating that better ergonomic knowledge and perception are associated with improved practices.
Correlation Between Total Knowledge, Total Perception and Total Self-Reported Practices Scores (n = 200).

Note. Spearman correlation coefficients (r) reported. p < .05 considered significant; p < .01 highly significant. Missing data handled using pairwise deletion.
Discussion
This study assessed knowledge, perceptions, and self-reported practices regarding ergonomic hazards among undergraduate nursing students. The results revealed deficiencies in all three domains, despite reported exposure to ergonomics training.
Only 21.5% of participants had good ergonomic knowledge, with the lowest scores related to posture and patient handling techniques. This aligns with prior research from Saudi Arabia and India, highlighting insufficient curriculum coverage of ergonomic principles (Al-Mutairi, 2023; Behera et al., 2023; Rajpurohit et al., 2024). However, moderate to high levels reported in Ethiopia suggest curriculum quality and clinical integration may vary between regions (Mohammed et al., 2023).
In terms of perception, 64.5% demonstrated a moderate level, while fewer felt confident using assistive devices or considered their training sufficient. This aligns with findings from Saudi Arabia and Botswana, where traditional teaching approaches limited students’ ergonomic confidence (Alsharari & Kerari, 2024; Kgakge et al., 2025). Simulation-based approaches have shown more promising outcomes in improving perception and preparedness (Alrashidi et al., 2023).
Unsatisfactory ergonomic practices were prevalent (54%), including frequent manual lifting and musculoskeletal discomfort. These behaviors parallel prior reports from India and other low- and middle-income settings (Behera et al., 2023; Rajpurohit et al., 2024). However, evidence from senior students and registered nurses shows that training and repeated reinforcement can improve adherence to safe practices (Abdollahi et al., 2020; Hochhauser & Liberman, 2024).
Significant associations were found between higher ergonomic competence and factors such as academic year, age, and prior training—indicating that experience and education enhance awareness and behavior (Karppi et al., 2022). Students who reported musculoskeletal discomfort scored lower in knowledge and practice, indicating a possible association between lower ergonomic competence and increased injury risk, without implying causality due to the cross-sectional design.
Positive correlations among knowledge, perception, and practices support the need for integrated educational strategies. This aligns with ergonomic education frameworks and empirical studies that emphasize interconnected learning across cognitive, attitudinal, and behavioral domains (Karppi et al., 2022; Waters et al., 2021).
Although conducted in a Saudi Arabian context, these findings align with international evidence highlighting similar ergonomic challenges among nursing students worldwide. This underscores the need for global integration of practical ergonomics training in nursing education.
Implications for Practice
The findings of this study emphasize the urgent need to strengthen ergonomic education in undergraduate nursing curricula. The current reliance on theoretical lectures without adequate practical reinforcement limits students’ ability to translate knowledge into safe clinical practices. Structured training that spans all academic years integrating hands-on practice, simulation modules, and competency-based evaluation should be prioritized to ensure that ergonomic principles are effectively applied in real-world settings. Effective mentorship during clinical placements is also essential for modeling safe patient handling and posture techniques, thereby reducing the risk of musculoskeletal disorders among future nurses. These implications highlight the importance of aligning ergonomic education with both theoretical instruction and supervised clinical practice to build lasting competence.
The positive correlations among knowledge, perceptions, and practices suggest that an integrated educational strategy combining theoretical instruction, simulation-based training, and supervised clinical mentorship may improve all three domains concurrently.
Strengths and Limitations
This study provides valuable insights into ergonomic knowledge, perceptions, and practices among nursing students in Saudi Arabia, addressing a relatively under-researched topic in the region. The use of a validated and reliable instrument, a large sample size including students across all academic years, and a high response rate strengthen the robustness of the findings. However, several limitations should be noted. The cross-sectional design limits causal inference, and the single-institution setting may restrict generalizability to other nursing schools. Additionally, reliance on self-reported practices introduces the possibility of recall and social desirability bias. Despite these limitations, the study contributes important evidence that can guide curriculum development and inform interventions to promote safe ergonomic practices among future nurses.
Conclusion
This study revealed critical gaps in ergonomic knowledge, perceptions, and practices among undergraduate nursing students, despite some exposure to relevant training. The findings highlight the need for more integrated, experiential ergonomics education to enhance students’ preparedness for clinical demands and reduce the risk of musculoskeletal injuries. Strengthening curriculum content, incorporating simulation-based learning, and fostering clinical mentorship are essential strategies to improve ergonomic competence in future nurses. These results underscore the importance of proactive educational reform in promoting long-term occupational health and patient safety.
Supplemental Material
sj-docx-1-son-10.1177_23779608251411368 - Supplemental material for Assessment of Undergraduate Nursing Students’ Knowledge, Perceptions, and Practices Regarding Ergonomic Hazards: A Cross-Sectional Study
Supplemental material, sj-docx-1-son-10.1177_23779608251411368 for Assessment of Undergraduate Nursing Students’ Knowledge, Perceptions, and Practices Regarding Ergonomic Hazards: A Cross-Sectional Study by Shimmaa Mansour Moustafa Mohamed, BN, MSc, PhD, Puvaneswari Kanagaraj, MSc, PhD, Sudha Annasaheb Raddi, MSc, PhD, Gihan Mohamed Mohamed Salem, BN, MSc, PhD, Noha Mohammed Ibrahim, PhD, Vasantha Gurusamy, MSc, PhD, Raghad Almushawah, BSN, RN, Nehal Demerdash, MSc, PhD and Wael G. Nouh, MSc, PhD in SAGE Open Nursing
Footnotes
Acknowledgments
The authors are thankful to the Deanship of Graduate Studies and Scientific Research at University of Bisha for supporting this work through the Fast-Track Research Support Program.
Ethical Approval
Ethical approval was obtained from the UB-RELOC Institutional Review Board of the University of Bisha, Saudi Arabia (Approval No.: H-06-BH-087/(11/03/46)). All participants were informed about the purpose of the study, and written informed consent was obtained prior to participation. Confidentiality and anonymity were maintained throughout the research process, and participation was voluntary.
Consent Statement
All participants provided written informed consent prior to data collection.
Author Contributions
All authors have participated sufficiently in the work to take public responsibility for appropriate portions of the paper and approve of the final version of the manuscript.
Shimmaa Mansour Moustafa Mohamed: Made substantial contributions to conception and design, data collection, analysis and interpretation, drafting and final approval of the manuscript.
Puvaneswari Kanagaraj: Involved in drafting the manuscript, revising it critically for important intellectual content and final approval of the manuscript.
Sudha Raddi: Involved in drafting the manuscript, revising it critically for important intellectual content and final approval of the manuscript.
Gihan Mohamed: Involved in drafting the manuscript, revising it critically for important intellectual content and final approval of the manuscript.
Noha Mohamed: Involved in drafting the manuscript, revising it critically for important intellectual content and final approval of the manuscript.
Raghad Almushawah: Involved in drafting the manuscript and final approval of the manuscript.
Vasantha Gurusamy: Involved in drafting the manuscript, revising it critically for important intellectual content and final approval of the manuscript.
Nehal Demerdash: Involved in drafting the manuscript and final approval of the manuscript.
Wael Gamal: Involved in drafting the manuscript and final approval of the manuscript.
All authors agreed to the final approval of the version to be published and to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Recommendations
Future research should explore the long-term impact of simulation-based ergonomics training on students’ clinical behavior and injury rates.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available due to confidentiality agreements but are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.