
Abstract
Introduction
The Anorexia–Cachexia Syndrome (ACS) is a severe complication of cancer and is considered to be a significant cause of morbidity and mortality affecting up to two-thirds of cancer patients and one that needs specialized nursing care. Studies showed that the ACS has been relatively under-researched and under-resourced whist the nurses’ knowledge has not been systematically explored.
Objective
Τo explores nurses’ knowledge, understanding, and management of ACS in clinical practice in two European countries.
Methods
Descriptive-comparative study with 197 cancer nurses recruited during two National Conferences in Greece and Cyprus. Data were retrieved with the “Investigation of anorexia–cachexia syndrome in Practice” questionnaire.
Results
In terms of nurses’ perceptions on ACS, the prevailing characteristic reported in both countries was anorexia (p = .65) followed by weight loss (p = .04). 189 nurses (95.9%, p = .176) do not currently use a tool to assess patients’ nutritional status as part of their standard clinical practice. Statistically significant differences were found in relation to the routine assessment of nutritional-related symptoms including early satiety (Cyprus 64% vs. Greece 37%, p = .001), hiccough (66% vs. 36%, p < .001), alteration of the taste/odor sensation (77% vs. 45%, p < .001), problems in the oral cavity (84% vs. 68%, p = .032) and daily activities (85% vs. 69%, p = .032). The priority level for the ACS management differed significantly in the two countries (p = .006), with higher priority being reported in Cyprus.
Conclusion
The study showed that more education is needed for cancer nurses to better understand the ACS which can facilitate the better management of the syndrome in clinical practice.
Introduction
Current and novel anticancer treatments are improving survival. However, all these treatments can play a role in the development of adverse events including malnutrition and metabolic alterations in cancer patients. Hence, nutritional deficiency can become a common medical problem that affects 15%–40% of cancer patients (Arends et al., 2017). Disease-related malnutrition has been defined as a condition resulting from the activation of the systemic inflammatory response by cancer. This inflammatory response causes anorexia and tissue damage, which in turn, can cause weight loss, decreased body composition, and functional capacity and ultimately induce the Anorexia–Cachexia Syndrome (ACS).
ACS is a severe clinical consequence of almost all chronic diseases when reaching advanced stages. ACS has been defined as “a multifactorial syndrome defined by an ongoing loss of skeletal muscle mass (with or without loss of fat mass) that can be partially but not entirely reversed by conventional nutritional support” (Fearon et al., 2011). ACS prevalence can vary significantly depending on the tumor type and the disease progression. Its prevalence has been reported in the ranges of 50%–80% in advanced cancer. More aggressive forms of non-Hodgkin’ lymphoma, colon cancer, and other cancers are associated with a frequency of weight loss between 50 and 60% (Fox et al., 2009). Similarly, mortality rates of patients with ACS can range from 20%–80% in cancer patients. Several hypotheses have been advanced to explain a biologically plausible association between ACS and death. Among these hypotheses, a prominent one is the one that refers to the platelet pathway. According to this hypothesis, relative thrombocytosis potentially further enhanced by platelet function activation or other platelet aspect augmentation such as an increase in platelet volume, leads to a predisposition to thromboembolic events including cardiovascular or cerebrovascular events and sudden death (Kalantar-Zadeh et al., 2013). ACS results in a state of active inflammation whereby tumour-derived factors and the aberrant host response to these factors result in a catabolic state which subsequently can impact on clinical outcomes including overall survival, quality of life, and performance status (Donohoe et al., 2011). In the context of ovarian cancer, for example, Hess et al. (2007) found a significant relationship between weight change and survival—on multivariate analysis, the risk of death increased by 7% for each 5% drop of body weight.
In the industrialized world (North America, Europe, and Japan) where epidemiological data are to some degree available, the overall prevalence of cachexia is growing with the growth of the chronic illness prevalence, and it currently affects around 6–12 million people. About 1.5–2 million deaths are occurring in patients with cachexia per year. Recent studies showed that a total of 800,300 patients (15.8 per 10,000 of the total population of the EU) and 527,100 patients (16.5 per 10,000 of the total US population) suffer from cancer-related cachexia (Lainscak & Rosano, 2019).
There are numerous mechanisms of action for ACS and these can be categorized as being related to central (e.g., depression, pain) or peripheral mechanisms (e.g., tumors causing dysphagia, tumors leading to alterations in nutrients resulting in anorexia, most antitumour therapies exacerbate anorexia and worsen body weight loss). Regardless of the causes, the lack of awareness and knowledge about cachexia can also be a contributing factor to the exacerbation of the ACS. Furthermore, Lainscak (2019) has identified the lack of financial resources allocated to the coding of cachexia as a contributing factor (Lainscak & Rosano, 2019).
Mattox (2017) presented the latest criteria for the diagnosis of the ACS which include: (1) assessing quality of life and anorexia, (2) measuring caloric intake (3) determine nutrition impact risk factors and symptoms (4) measure weight and body composition and (5) check biological markers. Many of these criteria focus on the weight loss and appetite (Mattox, 2017). Later studies on ACS also acknowledged the role of the body composition and other metabolic alterations on the degree of clinical abnormalities and outcomes that accompanying weight loss (Watanabe et al., 2018).
Regardless of the management approach implemented, the role of educating patients and families on the causes and implications of cachexia and raising awareness remains essential. The importance of the education has also been highlighted by the Clinical Framework for Quality Care in Cancer Cachexia (Clara Granda-Cameron, 2018). Nevertheless, preceding studies showed that healthcare professionals often face challenges in communicating with patients and their families about malnutrition issues and cachexia (Hopkinson, 2015; Millar et al., 2013; Reid et al., 2013). Although earlier studies showed that healthcare professionals receive limited formal education on cachexia-related issues at both undergraduate and postgraduate levels and have limited understanding of the syndrome (Donald & Kotler, 2000), recent studies showed that healthcare professionals’ knowledge and awareness of cachexia has improved (Scott et al., 2016).
Nurses are well placed to support people with ACS as they interact with patients across the cancer continuum which places them in a unique position to systematically and consistently monitor patients’ conditions. While the understanding of the multifactorial pathogenesis of ACS and its detrimental impact is improving, this knowledge still needs to be shared more widely and applied in clinical practice in a more systematic way. The scarcity of studies with a specific emphasis on nurses training preparation and actual clinical practices translates into a limited understanding of the effective transference of the theoretical knowledge in the clinical practice. With the focus shifting towards the importance of early recognition and intervention, increasing nurses’ understanding of the role of nutrition in cancer care is essential. Preceding studies have demonstrated that the perception and clinical practices concerning the anorexia–cachexia syndrome vary among healthcare professionals worldwide while acknowledging that there is a gap in studies that aim to acquire the relevant knowledge of nurses working with cancer patients in relation to the anorexia–cachexia syndrome (Muscaritoli et al., 2016). Other studies have identified the specific country practices as a barrier to the proper management of the anorexia–cachexia syndrome that can include reimbursement and legislation. Changes to the National Health Insurance schemes to include cachexia as a specific pathology or comorbidity so that it allows specific funding for its management is a key aspect of the regulation of cachexia management (Senesse et al., 2017). Furthermore, the provision of cross-country exploration studies in relation to the anorexia–cachexia syndrome knowledge among healthcare professionals, can potentially provide the basis for the development of a core curriculum in this field. This can form the core basis of the training program along with the country-specific elements and conditions in this context. This aspect highlights, even more, the importance of cross-country comparisons in this field of study. Therefore, this study has been designed explicitly to explore the knowledge of nurses regarding the ACS within the cancer care context in Cyprus and Greece.
Methods
Study Design
This was a descriptive-comparative study with participants been recruited from Cyprus and Greece.
Research Questions
What are the current management practices for ACS in clinical practice?
What are the differences in the knowledge of nurses regarding the ACS in Cyprus and Greece?
Sample and Sampling Planning
The sample consisted of 119 nurses (response rate 62% from eligible participants) working in oncology departments who attended the 8th Nursing Oncology Conference in Cyprus and 78 nurses (response rate 54% from eligible participants) who attended the 5th Symposium of Nursing Oncology in Greece. Both conferences took place in 2018. Recruitment and data collection continued through the duration of the two conferences. Participants were informed (oral and written) on the aim of the study and volunteered their participation in the survey with a written consent form. Following, the written consent, they proceeded to answer the questionnaires. The response time needed for each questionnaire was approximately 15–20 min. The questionnaires were placed in closed envelopes and anonymity was maintained.
Inclusion Criteria
The recruitment of the nurses was guided by the following inclusion criteria:
Registered nurses (with a diploma or bachelor's degree) Clinical experience ≥ 3 years in oncology settings Willingness to participate
Exclusion Criteria
Auxiliary nurses
Nurses who have not worked with cancer patients in the last 5 years
Nurses who refused to participate in the survey
Research Tool
The research data were retrieved with the “Investigation of anorexia–cachexia syndrome in Practice” questionnaire developed by Churm, (Churm et al., 2009). The questionnaire consisted of 8 questions about the ACS practices and 8 questions about nurse's demographic characteristics. The three domains covered by the questionnaire included: views of the characteristics of cachexia, assessment, and management of symptoms commonly associated with ACS. As part of this study, three additional questions were included to retrieve the perspectives of the nurses on: the use of guidelines for the management of ACS, whether their educational preparation was sufficient to manage ACS, and what is the level of priority (i.e., low, medium, high) assigned to the management of ACS in comparison to other symptoms. The questionnaire was presented to the participants in their native language (i.e., Greek). The nurses were able to complete and return the questionnaire through the conferences’ duration (one reminder was addressed to the conferees during the lunch break). The data were then coded and analyzed, to draw inferences.
Data Analysis
The demographic characteristics of the participants are presented as frequencies (N) and percentages (%) for the categorical variables (e.g., Gender, Education, Position, and Average and Standard Deviation for Continuous Variables (e.g., Age, Years of Service).
Qualitative data that derived from the open questions such as the question “In your practice, what features do you think characterize a patient with cancer cachexia?” were coded and analyzed by implementing thematic analysis in order to identify semantic themes within the data. Coding is a process of identifying a passage in the text or other data items, searching and identifying concepts, and finding relations between them (Bennett et al., 2018). Within this study, the authors employed an inductive coding which is a ground-up approach where the codes are derived from the data. This coding approach entails that no preconceived notions of what the codes should be are made but on the contrary it allows the narrative to emerge from the raw data itself (Questions et al., 2018). The processes of coding and analysis were undertaken by the SG, CC, TI and moderated by AC. According to Braun and Clarke (2006), the semantic level of themes refers “…within the explicit or surface meanings of the data and the analyst is not looking for anything beyond what a participant has said or what has been written.” (Braun & Clarke, 2006). These themes were then categorized and are presented as frequencies (N) and percentages (%).
The comparison between the perspectives among nurses from Greece and Cyprus was done with the Pearson Chi-square test. The Fisher's exact test was applied in cases where the sample size was ≤5 because applying the approximation method, which is the method where the chi-squared test relies on, is inadequate. The statistical analysis was done in SPSS v.25 and the statistical significance was set at p = .05.
Research Ethics
The study was carried out following ethical approval according to National law. The ethical issues underlying this research are related to the provision of written authorizations by the competent bodies, the preservation of data confidentiality, the preservation of privacy (i.e., confidentiality and anonymity), and their fair treatment. Before delivering the questionnaires, participants were informed about the aim of the study and their right to deny participation or withdraw from the study, without consequences. Participation to the study requested a written informed consent. The study is in accordance to the provisions of the Helsinki Declaration.
Results
Sample Characteristics by Country
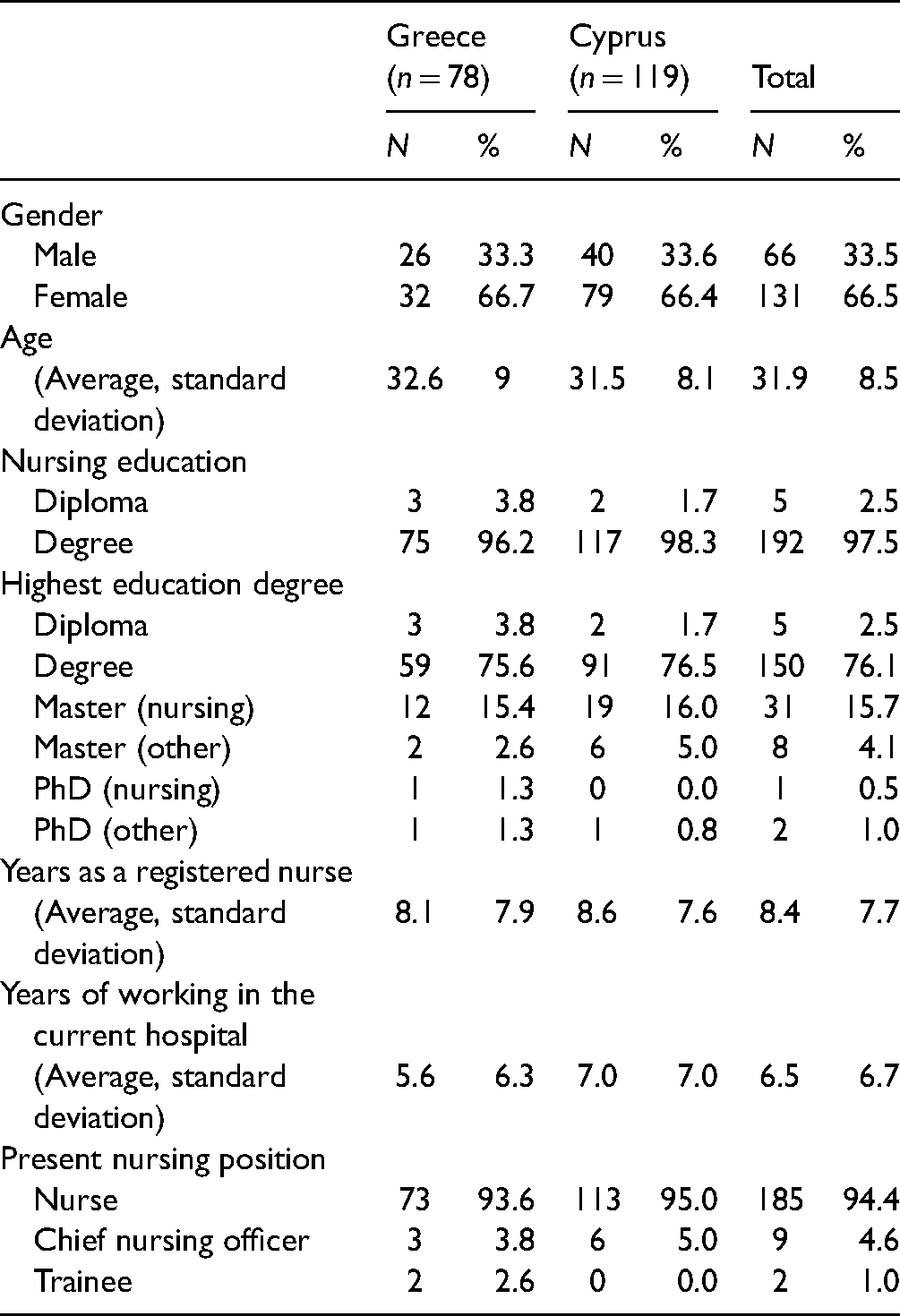
The study included in total 197 nurses; 119 from Cyprus and 78 from Greece, with a mean age of 31.9 years (typical deviation of 8.5 years) and the majority (N = 131 or 66.5%) being women. As far as basic nursing education is concerned, 192 (97.5%) had a degree and 5 (2.5%) had a diploma. The highest educational qualifications in both countries were: Degree (76.1%) and Masters (19.8%). They had an average of 8.4 years (typical Deviation of 7.7 years) working as Registered Nurses, and an average of 6.5 years (standard Deviation of 6.7 years) working in their present workplace. 185 (94.4%) were nurses, 9 (4.6%) chief nursing officers, and 2 (1%) trainees. No statistically significant differences (p > .05) were observed between the demographic characteristics of the participants in the two countries. A detailed description of the sample's demographic characteristics appears in Table 1.
Demographic Characteristics.
Current Management Practices for ACS in Clinical Practice
Utilization of a Nutrition Assessment Tool for Patients
189 nurses (95.9%) in total (Cyprus: 97.5%, Greece: 93.6%, p = .176) do not currently use a tool for assessing the nutritional status of patients as part of their standard practice. In Greece, 3 nurses stated that they use laboratory and blood tests for the nutritional assessment, 1 nurse reported that there was a questionnaire utilized as a part of the nursing history retrieval and 1 nurse routinely reported the recording of fluid balance. In Cyprus, 2 nurses reported that there was a questionnaire utilized as a part of the nursing history, and a nurse reported that a nutrition data tool was routinely utilized—a tool that was created by a doctor in his/her own workplace and was not validated.
Routine Assessment of Nutritional-Related Symptoms and Information
In their clinical routine, over 90% of the nurses (N = 177) asked the patients about the following: appetite, diarrhea, constipation, nausea and/or vomiting, pain, and food intake. Early satiety (when eating), and hiccough, were found to be evaluated by almost one in two nurses (p = .001 and <.001 respectively). Table 2 and Figure 1 provide a detailed analysis on the nutritional-related symptoms and information retrieved by the nurses on a routine basis per country.
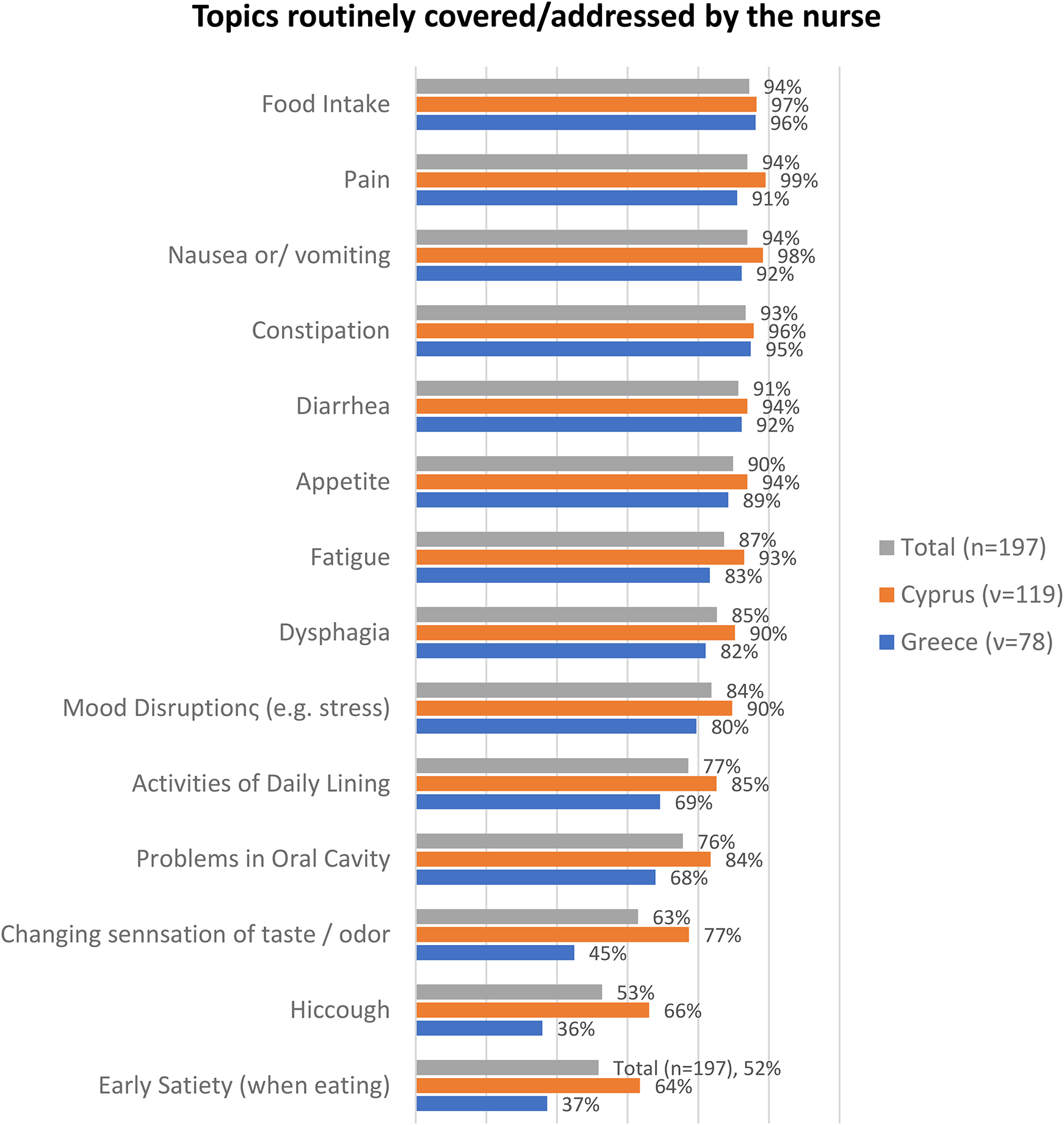
Routine assessment of nutritional-related symptoms and information.
Routine Assessment of Nutritional-Related Symptoms and Information.

Comparisons Between Greece and Cyprus
Nurses in Cyprus ask more frequently than nurses in Greece for early satiety (when taking food) [Cyprus 64% vs. Greece 37%, p = .001], hiccough [66% vs. 36% p < .001], alteration of the taste/odor sensation [77% vs. 45%, p < .001], problems in the oral cavity [84% vs. 68%, p = .032] and daily activities [85% vs. 69%, p = .032].
Features That Characterize a Patient With ACS
Table 3 shows the ACS features that were reported by the respondents in Cyprus and Greece. The features that were most frequently reported included: (1) weight loss by 75 nurses (p = .04); (2) anorexia by 82 nurses (p = .65); 3) weakness by 67 nurses (p = .44), 4) fatigue by 40 nurses (p = .50), (5) pain by 23 nurses (p = .96), (6) depression by 24 nurses (p = .50) and (7) palliative care by 18 nurses (p = .28). Table 3 shows the characteristics of the ACS categorized by query and country of origin.
Characteristics of ACS.

*Fishers’ exact test.
Differences Between the Characteristics Identified in Cyprus and Greece in Terms of the Features Present in a Patient With ACS
Nurses in Greece reported anorexia (Cyprus 40% vs. Greece 44%) and depression (14% vs. 11%), more often than the nurses in Cyprus. In Cyprus, nurses reported more often weight loss (44% vs. 29%), weakness (36% vs. 31%), fatigue (22% vs. 18%), and pallor (11% vs. 6%). The only pain was equally reported in both countries (12%). The statistical significance for weight loss was found to be p = .04 (Supplementary Figure 1). There was no statistically significant difference among the variables since the nurses’ responses were similar except for weight loss as shown in Supplementary Figure 1.
Actions for the Management of Dry Mouth
The most common actions reported for the management of dry mouth included: oral hygiene/solutions/washing/brushing (N = 108), fluid intake/hydration (N = 88), candies and chewing gum (N = 17), oral gels (N = 12), antifungal medicines (N = 12), intravenous fluids (N = 8) and lemonade/lemon/honey/glycerin (N = 8). Table 4 shows in detail the actions reported by nurses in Greece and Cyprus.
Actions for the Management of Dry Mouth.

*Fishers’ exact test.
Differences Between Cyprus and Greece
Nurses in Cyprus stated that in their clinical practice they more often utilize oral hygiene measures/solutions/washing/brushing oral gels (65% vs. 40%), antifungal medicines (8% vs. 3%) and lemon/honey/glycerin (5% vs. 3%; Supplementary Figure 2). Nurses in Greece stated a lower utilization of oral hygiene measures compared to nurses in Cyprus (40% vs. 65%; x2 = 10.7, p < .001). Nurses in Greece reported that in their clinical practice they more frequently utilize fluid intake/hydration (51% vs. 40%; x2 = , p = .12) candies/chewing gum (12% vs. 7%; x2 = 0.84, p = .36) and intravenous fluids (10% vs. 0%). No other statistically significant differences were explored due to small sample sizes.
Actions for the Management of Early Satiety
The actions utilized by nurses in Greece and Cyprus in relation to the management of early satiety differed considerably. The most frequent actions reported by nurses in Cyprus were oral solutions (N = 53), fluid intake (N = 46), systemic oral hygiene (N = 25), and oral moisturizing gels (N = 10). Any other measures were utilized in a percentage of 1% (Supplementary Figure 3.1).
The most common actions to manage early satiety mentioned by nurses in Greece were: frequent meals (N = 29), nutritional supplements (N = 3), encouragement (N = 2), taking liquids (N = 2). Any other measures used, were mentioned at a lower frequency (Supplementary Figure 3.2).
Differences Between Cyprus and Greece for the Management of Early Satiety
The nurses’ views on the management of early satiety between the two countries differed significantly. As shown in Supplementary Figures 3.1 and 3.2 the nurses in the two countries utilize different methods (or with a different percentage of utilization of the same practices) within their practices the management of early satiety.
Nurses in Cyprus reported that in their clinical practice they more often utilize oral hygiene measures/solutions/washing/brushing oral gels (10% vs. 0%), antifungal medicines (8% vs. 3%) and lemon/lemon/honey/glycerin (5% vs. 3%). Nurses in Greece reported lower utilization of oral hygiene measures compared to nurses in Cyprus (40% vs. 65%; χ2 = 11.8, p < .001). Nurses in Greece reported that in their clinical practice they more frequently utilize oral fluid intake/hydration (51% vs. 40%), candies/chewing gum (12% vs. 7%), and intravenous fluids (10% vs. 0%). No other statistically significant differences were observed (p > .05).
Actions for the Management of Reduced Appetite
The most common actions taken by nurses to manage the reduced appetite included: small and frequent meals (N = 95), patient's food choices (N = 29), nutritional supplements (N = 21), nutritionist referral/light diet/cold meals/meals plan (N = 16) and fluid intake (N = 14). There were other measures used with a lower frequency as shown in Table 5.
Actions for the Management of Reduced Appetite.

*Fishers' exact test.
Differences Between Cyprus and Greece
Nurses in Cyprus reported that they more often provide to patients small and frequent meals (67% vs. 19%; χ2 = 43.47, p < .001). They also reported that they tend to utilize more diet/light diet/cold meals/meal plan/fatty meals (9% vs. 6%), fluid intake (12% vs. 0%) within the patient's nutritional plan (χ2 = 7.18 p = .004).
Nurses in Greece reported a higher percentage of providing food according to patient's preferences (19% vs. 12%; χ2 = 2.09, p = .14), the administration of medication (12% vs. 3%; χ2 = 3.78, p = .049) and the use of food supplements (15% vs. 8%; χ2 = 1.66, p = .19). In both countries, nurses encouraged their patients to increase their food intake in a percentage of 6%.
In Cyprus, nurses reported much more frequently, the use of small and frequent meals (67%), liquid intake (12%), and choice of food by the patient (12%) as means to manage the presence of reduced appetite. In Greece, they reported much more frequently the utilization of small and frequent meals (19%) choice of food by the patient (19%) and food supplements (15%; Supplementary Figure 4). No other statistically significant differences were found (p > .05).
Healthcare Professionals Involved in the Care of Patients With ACS
To the question, “Have other healthcare professionals joined the care of patients with cachexia?”, 157 nurses (79.7%) from both Greece and Cyprus responded positively. The data showed that nurses in Cyprus were more likely to involve other healthcare professionals in the care of patients with ACS compared to their colleagues from Greece. [Greece 70.5%, Cyprus 85.7%, χ2 = 6.7, p = .009].
Out of the 157 nurses that responded positively, the specialties of professionals that were involved in the care of patients with ACS included: nutritionists (Ν = 111), psychologists (Ν = 68), other nurses (Ν = 32), physiotherapists (Ν = 23) and oncologists (Ν = 13). Additional specialties have been reported at a lower frequency (Supplementary Figure 5).
Differences Between Cyprus and Greece
In Cyprus, nurses reported much more frequently the involvement of nutritionists were involved in the care of patients with cachexia than in Greece (78% vs. 56%, χ2 = 8.4 p = .003; Table 6).
Healthcare Professionals Involved in the Care of Patients with ACS.

*Fishers' exact test.
Management of ACS Incidents in Your Department According to Specific Policies
Participants were requested to answer whether the management of patients with ACS in their department is done according to a specific policy (e.g., guidelines in place). Thirty-three nurses (16.8%) responded positively and 164 (83.2%) answered that the management of these patients is not guided by any specific policy. There were no statistically significant differences between Greece and Cyprus on this matter. [Positive Response Greece 20.5%, Cyprus 14.3%, χ2 = 1.3, p = .252]
As far as policies utilized, in Cyprus, nurses stated using the “Determinant Importation into the Chamber” (N = 7), nutritionist referral (N = 3), special diet (N = 3), and psychological support (N = 1). In Greece, the following policies were reported: treatment of chemotherapy side effects (N = 7), check with the Norton ladder (N = 1), medical and paramedical staff (N = 1), nutritional group (N = 1), protocols (N = 1), and nutritionist referral (N = 1).
Education in Relation to ACS
To the question, “Do you think you have been given the necessary training to be able to effectively manage patients with ACS?” only 45 nurses (22.8%) responded positively, whereas 152 nurses (77.2%) responded negatively. There were no statistically significant differences between nurses from Greece and Cyprus [Positive Response Greece 24.4%, Cyprus 21.8%, χ2 = 0.16, p = .68].
Of those who responded negatively, we retrieved their perspectives on what they thought is needed to improve the management of anorexia–cachexia incidents. Nurses in Cyprus reported that measures should include: conferences (N = 9), education (N = 7), protocols (N = 4), expert meetings (N = 2), interdisciplinary approach (N = 1), and interdisciplinary team collaboration (N = 1). In Greece, the nurses reported the following measures: education (N = 4), seminars (N = 4), protocols (N = 2), conferences (N = 1), clinical nursing experience (N = 1), and a better understanding of patient's preferences (N = 1; Supplementary Figure 6).
Differences Between Greece and Cyprus
In Cyprus, the provision of conferences as a means to increase the better management of anorexia–cachexia incidents were reported more often (35%) than in Greece (5%; p = .019). Moreover, in Greece nurses reported seminars and information, while in Cyprus they did not report these. Furthermore, in Cyprus, nurses reported expert meetings, interdisciplinary approach, and cooperation with the interdisciplinary team, while in Greece nurses did not identify these means. No other statistically significant difference was found (p > .05).
Priority Level Attributed to the Management of ACS in Relation to Other Symptoms
To the question “What do you think is the priority level attributed to anorexia–cachexia management in relation to other symptoms, more than half of the nurses reported “Moderate Priority.” Specifically, 30 nurses (15.2%) reported “Low Priority,” 118 nurses (59.9%) reported “Moderate Priority” and 49 nurses (24.9%) reported “High Priority.”
The level of priority appeared to be differentiated between Greece and Cyprus (p = .006) wherein Cyprus the level of “High Priority” was reported by 39 nurses (32.8%) compared to 10 nurses (12.8%) in Greece as shown in Table 7 and Supplementary Figure 7. No other statistically significant differences were observed (p > .05) as shown in Table 7.
Priority Management of ACS.
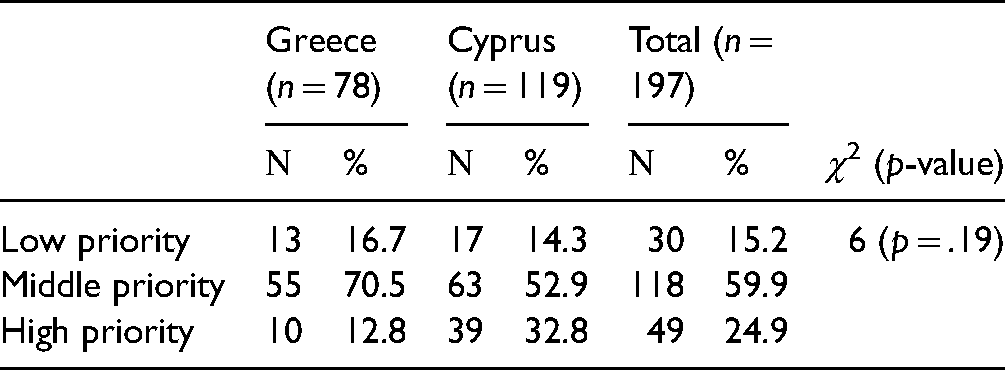
Supplementary Figure 7 presents the percentages in Cyprus and Greece as regards to the priority level given for the management of ACS. There was a statistically significant difference between Cyprus and Greece since in Cyprus the “High Priority” level was 32.8% and in Greece 12.8% (39 nurses vs. 10 nurses, p = .006). “Moderate priority” was reported by 63 nurses (52.9%) in Cyprus and 55 nurses (70.5%) in Greece. “Low priority” was reported in Cyprus by 17 nurses (14.3%), as opposed to Greece where 13 nurses (16.7%) reported it.
Discussion
This was a study aiming to explore cancer nurses’ knowledge on the ACS as well as any differences in the two European countries. The findings showed that nurses are not appropriately educated to recognize, prevent, and manage the ACS and therefore, developing appropriate skills were deemed necessary for those involved in the treatment of such patients. The lack of formal education (77.2% responded negatively) combined with the lack of a standardized evaluation tool (83.2% responded negatively) contributed to the inability to cope consistently with the patients’ complex needs. Preceding studies showed that formal and informal education on anorexia–cachexia has led to improved understanding and provided healthcare professionals with the knowledge and confidence that was required to identify and discuss anorexia–cachexia, and its implications, with patients and their families (Millar et al., 2013; Scott et al., 2016). Studies showed that healthcare professionals received limited formal education about cachexia at both undergraduate and postgraduate levels and consequently had limited understanding of the syndrome. The implementation of techniques such as motivational interviewing, solution-focused brief therapy, and cognitive behavioral therapy may help healthcare professionals achieve this aim (Hopkinson & Richardson, 2015; Millar et al., 2013). An aspect to be considered in this context is that education and training alone are not sufficient to introduce change in relation to the ACS management. In the literature, barriers have been identified in terms of the organizations providing the care as well as barriers to implementation of ACS management interventions (e.g., nutritional advice). With regards to the former, studies show that insufficient reimbursement policies can impact negatively on the effective management of ACS. Equally important (and related) are the regulatory barriers to the management of ACS. The nonrecognition of ACS as a specific pathology or comorbidity will prevent the adoption or corresponding guidelines and protocols to be introduced in clinical practice whilst it will also place financial constraints in the ACS managing efforts (Senesse et al., 2017). The nonrecognition of ACS as a specific pathology or comorbidity creates another barrier as it negatively impacts the mentality and perceptions of the organization's healthcare professionals towards the importance of the syndrome and the necessity to address it in the clinical context. This also creates a poor integration of the ACS within the clinics/departments managers’ priorities across the care and treatment continuum which in turn is transferred to the bedside care leaving the syndrome underdiagnosed and undertreated. With regards to the former, it is worth highlighting the power of behavior among cancer patients and their informal caregivers with reference to the importance of ACS and the adherence to corresponding interventions. This primarily can be cultivated by the healthcare professionals and in the event that is poorly addressed then this results to a corresponding behavior by cancer patients and their informal caregivers. Studies show that this can be an attributing factor to poor adherence to nutritional advice (Nasrah et al., 2020).
A finding that further demonstrates the need for appropriate training on all the features (i.e., holistic) of ACS is that although most of the nurses in this study were familiar with risk factors for malnutrition and signs of existing malnutrition, it appeared that their knowledge was not consistently applied in practice (or poorly applied), or used incorrectly. According to the results, in Cyprus and Greece, nurses in their practice tend to address some common features for the recognition of the ACS, such as anorexia, weight loss, and weakness, as the main features presented by patients, however, these were not statistically significant (p > .05). This finding also highlights the need for complementing theoretical training with clinical practice. Scott et al. (2016) found that nurses were able to recognize the symptoms of the syndrome because they had previously gained experience in clinics treating patients with ACS. However, different contexts contributed to inappropriate learning opportunities both within and between different professional groups.
The above finding also stresses the need to move beyond the standard educational practices in relation to ACS and place emphasis in the personalized educational needs of the nurses working with patients at risk of ACS. Bjerrum et al. (2012), referred to procedures for screening and registration and only mentioned signs of malnutrition such as weight loss, but not other obvious signs such as lethargy, and they only sporadically mentioned risk factors for malnutrition, for example, unintentional weight loss (Bjerrum et al., 2012). The demand for focus on, for example, nutrition physiology is noteworthy, as it was part of the training program developed by Bjerrum et al. (2012). One explanation could be that nurses still want standard solutions. Nurses also referred to the reduced time of workload to attend scheduled supervision. Their knowledge of nutrition, in general, indicates a need for academic concepts, as they do not articulate concrete nurse-specific initiatives, but their training program projects demonstrated their knowledge on a concrete level, as they worked with posters and pamphlets addressing the patients.
Without comprehensive theoretical knowledge and appropriate clinical training, nurses are unable to provide appropriate nutritional care across the cancer continuum. Although nutritional issues are taught during basic nursing education (i.e., degree level/4-year university study), many trained nurses complain that they do not have adequate nutritional knowledge. However, nurses in this study recognized deficiencies in their knowledge and welcomed the idea of further education. Globally, it is acknowledged that in order to ensure the best possible care there is a need to recognize cachexia as a specific syndrome requiring specific and multimodal care and our results suggest that it may be beneficial to incorporate cachexia education into teaching at both preregistration postregistration levels.
The results also showed that 95.7% of nurses in Cyprus and 93% of nurses in Greece, were not utilizing an assessment tool to evaluate patients’ nutritional status as a standard practice. This is not an infrequent finding, as the lack of a universally accepted cancer cachexia-specific assessment tool is identified in the literature. Often, this is substituted by other malnutrition screening tools that help to determine the degree of malnourishment and where nutritional support is indicated. As it was demonstrated in the findings of the current study, nurses utilize laboratory and blood tests as well as centre-specific questionnaires (i.e., there is no evidence on their validity) for the assessment of the patient's nutritional status. However, despite the availability of alternative tools (not cancer-specific) these are not regularly utilized in clinical practice (at least not to the precachexia stage). The absence of formal education and understanding coupled with the lack of a standardized assessment tool contributes to the inability to consistently address the needs of cancer patients with cachexia (Churm et al., 2009).
With reference to the inclusion of other healthcare professionals in the care of cancer patients with ACS, the results showed that the nurses referred patients primarily to a nutritionist (N = 111 nurses). Previously Churm et al. (2009) found that the involvement of a nutritionist contributes to the better management of ACS (Churm et al., 2009). Α position paper by the European School of Oncology Task Force on the management of malnutrition and cachexia concludes that given the multifaceted nature of the problem, the solution is likely to lie in a multi-modality approach (Macdermid et al., 2014). Furthermore, the findings of (Parmar et al., 2017) demonstrated that a multidisciplinary rehabilitation program for cancer cachexia can improve quality of life by improving the management of all facets of the cancer cachexia syndrome. Preceding studies have demonstrated that some barriers to proper management of cachexia include global practices like the lack of human resources and the specific country practices among which reimbursements and legislation (Dechaphunkul et al., 2013). It, therefore, becomes apparent that any strategy to comprehensively manage patients with ACS will require an appropriate financial investment in the form of training and reimbursement.
The absence of management guidelines for the ACS (both in Greece and Cyprus) in cancer patients has been demonstrated by the findings. Evidence in the literature stresses that the ACS remains a significant challenge in the management of cancer patients partly because there is no clear standard of care (Advani et al., 2018). Another contributing explanation for the nurses’ seemingly vague knowledge could be that their area of responsibility had not been specified, which is in line with previous studies showing an imprecise distribution of duties for nutritional assessment and planning among nurses and physicians (Bjerrum et al., 2012). The researchers also found that even though the nurses felt responsible for and were aware of the importance of nutrition, they still gave nutrition care low priority because of workload (Bjerrum et al., 2012). Another barrier that has been identified in the literature that contributed to the low priority ascribed to ACS by cancer nurses included the uncertainty of the effectiveness of the nutritional care they delivered, with uncertainty not only about the adequacy of training but also patient motivation to follow advice (Martin et al., 2014). This barrier factor is also influenced by the type and severity of cancer (i.e., diagnosis) and the critical state of other symptoms the nurses are treating. Nutritional support for example was not deemed as a priority in patients with more advanced disease, with the emphasis been attributed to more pressing symptoms (Cooper et al., 2015). On the topic of the priority level assigned to ACS management, this differed significantly in the two countries (p = .006) with higher priority being reported in Cyprus. This finding could be partially explained by the fact that the Cypriot nurses recruited in the study had more years of experience with cancer patients and hence managing ACS. This is also reflected in the relevant literature which demonstrates that more years of experience can contribute to the better management of ACS. For example, the study by Scott et al. (2016) concluded that despite not having a significant level of formal education about the care of patients with cachexia the consequences of this knowledge gap were mitigated by the experiential knowledge that was systematically gained through placements in a specialist clinic. Furthermore, although the level of training between the participants in the two countries was comparable, the content of the training curriculum might not have been. For example, the training curricula in Cyprus might attribute more attention to the nutritional challenges that cancer patients face across the cancer continuum creating an increased level of awareness among nurses.
Strengths and Limitations
Limitations of the study include the relatively small study sample and the chosen sampling method. In terms of the sampling method, the authors acknowledge that the study relies on the nurses with the willingness to participate which might have an impact on the generalizability of the findings. This is due to the fact that the nurses interested in the study were probably those who recognized their shortcomings related to ACS and the novel information intrigued them to participate. Nevertheless, the recruitment strategy that was utilized provided a rather representative sample of the nurses working with cancer patients in the two countries. Purposively targeting the nurses who attended the largest cancer nursing conferences in the two countries provided a balanced mix of the cancer nursing workforce allowing for conclusions to be drawn based on the findings. However, the researchers acknowledge the limitation that the participants had to complete the questionnaire during the conference. The conference setting might have been distracting and not optimal in providing well-thought responses to the questions. However, providing adequate time to the participants to provide their responses (8 h in total) has mitigated this problem. Despite its limitations, this study is the first attempt to capture the perceptions and practices of cancer nurses in Greece and Cyprus in relation to the understanding and management of the ACS within the cancer context.
Implications for Practice
The study has demonstrated that in order to achieve an increased level of nurses’ awareness for a broader part of nutrition care, we need a prolonged focus on nutrition care and treatment in the clinical practice, sustained efforts from the management to promote nurses into taking responsibility as well as an appropriate financial investment channeled in educational programs and the reimbursement policy. The management of this complex syndrome requires healthcare professionals of different specialties, to cooperate to avoid omissions related to the syndrome. Effective management demands an advanced level of awareness of the problem, together with appropriate and consistent assessment.
Conclusions
This study investigated Cypriot and Greek nurses' knowledge on ACS within the cancer care context. The results demonstrated that the knowledge background of the nurses working in this context is not sufficient to meet the complex needs of patients with ACS. This becomes more complex as currently a tool to facilitate the recognition of the ACS does not exist whilst there are limitations to recommend clinical management guidelines. This study was undertaken on the basis of clinical and empirical data that ACS is currently inadequately recognized and managed, leaving patients experiencing symptoms that may respond to available treatments and contribute to the better management of the syndrome and improved quality of life.
The study revealed that there are challenges regarding the management of the ACS within the cancer care context. Dietary care and nutritional assessment are important in the management of the syndrome. The role of the nurse and the results of the nursing care provided by the nurse in ACS are unclarified and need to be further investigated. Although, there are barriers such as the lack of a robust evidence base to support nutritional practices and the unmet need for nutrition education in cancer, additional research will reveal the potential role of the specialist cancer nurse in dietary care. This study will act as a trigger for cancer nurses to deal with the problem of ACS and find ways to ensure optimal cancer care for their patients.
Supplemental Material
sj-docx-1-son-10.1177_23779608211035208 - Supplemental material for Nurses’ Knowledge in Relation to the Anorexia–Cachexia Syndrome in Cancer Patients: A Cross-National Comparison in Two European Countries
Supplemental material, sj-docx-1-son-10.1177_23779608211035208 for Nurses’ Knowledge in Relation to the Anorexia–Cachexia Syndrome in Cancer Patients: A Cross-National Comparison in Two European Countries by Georgia Socratous, Constantina Cloconi, Ioanna Tsatsou and Andreas Charalambous in SAGE Open Nursing
Footnotes
Acknowledgments
The authors would like to thank all the nurses who participated in this study and provided their insightful perspectives on the topic.
Ethics Approvals
The licenses granted for the implementation of the study included: Assessment and approval by the Bioethics Committee of Cyprus—EEBK/EP/2018.01.138 (29th of August 2018). Authorization to conduct the survey by the Ministry of Health of Cyprus (medical and nursing services; September 14, 2018).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.