
Abstract
Background
Nurses and midwives play important role in managing neonatal jaundice and provide nursing health education to mothers on preventive and remedial measures to neonatal jaundice. However, the Knowledge, Attitudes, and Practices of nurses and midwives towards neonatal jaundice is not well understood in the Northern Region of Ghana.
Aim of the study
The study assessed the knowledge, attitudes, and practices of nurses and midwives towards the management of neonatal jaundice.
Design and Method
This is a hospital-based descriptive cross-sectional study, conducted between the periods of January 2021 to August 2021 in the Tamale Teaching Hospital, Northern Region, Ghana. Descriptive analysis such as mean, standard deviation, frequencies, and percentages were performed to give general description of the variables. Simple Pearson Chi-square test and logistic regression models were performed to test the level of associations between the outcome and independent variables and predictors for neonatal jaundice. A p-value of <.05 was considered statistically significant for the test of association.
Results
Among the 202 nurses and midwives, the mean age was 30.6 ± 3.8 years and majority were females (71.3%). The overall good knowledge, attitudes, and practices score towards neonatal jaundice was 69.30%, 64.90%, and 62.90%, respectively. After adjusting for other variables, good knowledge (adjusted odds ratio [AOR] = 22.41(10.21–49.18) p < .001) and good attitude (AOR = 25(11.86–55.07) p < .001) were positively associated with practices towards neonatal jaundice.
Conclusion/Interpretation
The participants demonstrated substantial knowledge, attitudes, and practices towards neonatal jaundice. However, there still exist some gaps in their knowledge, attitudes, and practices towards neonatal jaundice that need to be addressed to improve neonatal health outcomes in the study setting.
Introduction
Neonatal jaundice (NNJ) is a common pediatric condition, affecting 60% and 80% of term and preterm neonates, respectively, globally (Khan et al., 2015; Salia et al., 2021). Clinically, NNJ is defined by the yellowish coloration of the skin and sclera of the eye, suggesting raised levels of unconjugated bilirubin in the blood circulation (Khan et al., 2015). Previous studies have indicated that NNJ is a common reason for neonatal readmission to the hospital post-delivery discharge (Lancet, 2008; Seneadza et al., 2022). NNJ has serious implications on the general health of the neonates including kernicterus, hearing loss, cerebral palsy, and death (Mwaniki et al., 2012; Pediatrics et al., 2004; Seneadza et al., 2022). The burden of NNJ is significant in developing countries, and it is coupled with poor health resources and skills to diagnose and deal effectively with NNJ when it occurs (Seneadza et al., 2022). The American Academy of Pediatrics recommends the physical assessment for NNJ 12 h post-delivery and the measurement of transcutaneous bilirubin (TcB) or total serum bilirubin (TSB) in the first 24 h of life (Bhardwaj et al., 2023). However, studies have shown that measuring bilirubin (TcB or TSB) is the most effective way to detect NNJ in the first 24–48 h of life among neonates (Bhardwaj et al., 2023; Mazrah et al., 2022).
Ghana has seen increasing trend of cases of NNJ from 2015 to 2019 with 3,031, 4,251, 5,338, 7,175, and 9,273 cases of NNJ, respectively (Ghana Health Service, 2019; Salia et al., 2021). A cross-sectional study in the Central Region of Ghana reported NNJ prevalence of 66.7% (Adoba et al., 2018). Another study found that the severe form of NNJ was a common presentation among children receiving care at a neurologic clinic in Ghana (Adei-Atiemo et al., 2015). In the Tamale Metropolis, another cross-sectional study reported a 9.7% prevalence of severe NNJ (Abdul-Mumin et al., 2021).
Most previous studies on knowledge, attitudes, and practices (KAP) towards NNJ across the globe have largely been limited to caregivers and mothers (Al-Zamili & Saadoon, 2020; Onyearugha et al., 2016; Saud et al., 2016). Similarly, in Ghana, studies on KAP towards NNJ have focused on mothers (Abdul-Mumin et al., 2021; Salia et al., 2021; Seneadza et al., 2022). These studies reported deficits in KAP towards NNJ. The important question is what is the KAP of health workers, particularly nurses and midwives towards NNJ? Studies conducted elsewhere that involved health workers reported varying proportions of KAP towards NNJ (Alemu et al., 2011; Issa et al., 2018; Mirza & Atrushi, 2019; Shehu et al., 2019). Nurses’ role in the quest to attain the Sustainable Development Goal-3 and towards reducing neonatal mortalities and morbidities is significant. In the case of NNJ, this role extends from managing the condition to providing nursing health education to mothers on preventive and remedial measures. It is a common knowledge that one can only give what he/she has and therefore, nurses and midwives can only offer what they have including their KAPs. However, the KAPs of nurses and midwives towards NNJ are not well understood in the only tertiary hospital that serves the northern parts of Ghana. The study therefore assessed the KAPs of nurses and midwives towards the management of NNJ at a tertiary health facility in the Tamale Metropolis, Northern Region, Ghana.
Literature Review
Knowledge, Attitudes, and Practice Towards NNJ
Nurses and midwives are expected to recognize risk factors and early signs and symptoms for jaundice in the early days of life (Adoba et al., 2018). Nurses and midwives’ role of interacting with mother–neonate pair places an obligation on them to demonstrate substantial knowledge, combined with satisfactory attitudes and good clinical practices (Opara et al., 2014).
The prevention of NNJ is essential to save the lives of neonates, reduce related complications, and improve the general health outcomes of neonates especially in developing countries where neonatal mortalities and morbidities are high (Demis et al., 2021). Post-delivery early detection of NNJ in health facilities depends on nurses and midwives’ knowledge on the causes and associated risk factors of jaundice. Similarly, nurses and midwives’ role of educating mothers on NNJ will depend on their depth of knowledge of the condition. Poor knowledge and lack of better appreciation of NNJ is a precursor for poor clinical decisions including treat or not to treat, late medical care, and poor outcomes (Ayete-Nyampong & Udofia, 2020; Demis et al., 2021; Hannon et al., 2001; Opara et al., 2014). A decade and half literature on NNJ shows that much research focus on maternal knowledge on NNJ with little focus on healthcare providers (Adoba et al., 2018; Demis et al., 2021; Egube et al., 2013; Goodman et al., 2015; Lake et al., 2019; Ogunfowora & Daniel, 2006; Navabi et al., 2020; Said et al., 2018; Salia et al., 2021). However, there exist some studies on the knowledge of nurses and midwives on NNJ at varying levels (Alemu et al., 2011; Ekanem & Young, 1994; Ogunfowora & Daniel, 2006; Opara et al., 2014). A cross-sectional study conducted in Kurdistan, Iraq, among 166 nurses reported satisfactory knowledge on NNJ including phototherapy treatment (59.0%), causes (47.0%), and guidelines for management (75.3%). The study equally reported good knowledge of nurses on the clinical presentation of NNJ (98.8%), physical examination (82.5%), accompanying complications (47.0%), and nursing care practices (95.8%) (Mirza & Atrushi, 2019). Another cross-sectional study involving 60 staff nurses in Mysuru, India, showed an average knowledge (51.66%) of NNJ and significant association between participants’ knowledge and years of experience and unit where they work (Chandrasekhar et al., 2017). Ahmed and Hani’s (2017) cross-sectional study in Minia governorate, Egypt, found that among 41 nurses, 92.7% demonstrated good knowledge on NNJ. The study also revealed that 70.7% of participants had prior training in neonatal care, which likely contributed to their high level of knowledge. The study further demonstrated that knowledge of NNJ was significantly associated with the years of work experience (p ≤ .01), previous training (p ≤ .05), and age (p ≤ .005) of the participants (Ahmed & Hani, 2017). Another cross-sectional study conducted on a group of 91 healthcare providers revealed varying levels of knowledge on NNJ, as reported by Alemu et al. (2011). The findings showed that while the majority of participants (93.4%) were aware of NNJ and had been exposed to it in a hospital setting (66.8%), only a small percentage of participants (8.7%) demonstrated adequate knowledge on NNJ by correctly recognizing symptoms such as yellowish color of the skin and eyes, dark urine, itching, and convulsion (Alemu et al., 2011).
In the West African region, studies in Nigeria show that the level of knowledge on NNJ among healthcare providers in Nigeria varies widely, with some studies reporting suggestively good appreciation while others report poor knowledge (Ekanem & Young, 1994; Ogunfowora & Daniel, 2022; Opara et al., 2014; Orimadegun & Ojebiyi, 2017). While some healthcare providers correctly identify causes and treatment options for NNJ, others have misconceptions and use inappropriate treatments (Ekanem & Young, 1994; Ogunfowora & Daniel, 2022). These findings suggest a need for continuous education and training on current approaches to NNJ treatment and risk factors. The sources of information on NNJ for healthcare providers include school, seminars, working area, and the media (Alemu et al., 2011; Shehu et al., 2019). Overall, there has been little improvement in knowledge levels over the past decade, highlighting the need for more concerted efforts to improve awareness and understanding of NNJ among healthcare providers.
There is limited research on the knowledge of NNJ among healthcare providers, specifically nurses and midwives in Ghana. Most of the existing scholarships on NNJ in Ghana focus on mothers, with low levels of awareness reported. Adoba et al. (2018) found that only 17.3% of 150 mothers surveyed were aware of NNJ and 90% of them were unaware of the effects of NNJ on neonatal organs. Salia et al. (2021) reported that 45.5% of 202 mothers had good knowledge of NNJ, with education and previous awareness associated with higher odds of good knowledge. A study at the Tamale Teaching Hospital showed that only 17.1% of 76 mothers had knowledge of NNJ and 11.8% were able to identify the condition. These low levels of knowledge among mothers could be attributed to a lack of knowledge among nurses and midwives providing education during antenatal care (ANC) and postnatal care (PNC) visits or could reflect the priority areas for health education among expectant mothers and mothers at ANC and PNC.
Developing a positive attitude towards a subject is essential in shaping an individual's mindset, preconceptions, opinions, and thoughts concerning it, including topics related to healthcare and medicine, as stated by Ortmeyer (1949). Therefore, it is crucial for nurses and midwives to cultivate positive attitudes towards NNJ to improve neonatal outcomes. Additionally, nurses and midwives perform essential roles, such as coordinating communication, informing other units, staff, and parents on neonatal outcomes, as highlighted by Stark and Lannon (2009) and Yost (2017). In NNJ, nursing care during phototherapy is also critical as proper care practices significantly impact the effectiveness of treatment and reduce or eliminate complications. The nursing care practices involved in phototherapy comprise performing a thorough assessment, protecting the eyes and genital area, and carefully monitoring the baby's body temperature (Stark & Lannon, 2009; Yost, 2017). Effective delivery of light, correct positioning of the baby, adequate skin exposure, maintaining proper hydration, daily weighing, and promoting interaction between parents and the neonate are also important nursing care practices for managing NNJ (Ghada et al., 2016; Stark & Lannon, 2009; Yost, 2017). Mirza and Atrushi (2019) conducted a study in Kurdistan, Iraq, among 166 nurses and found that only 12.7% had a positive attitude towards NNJ, while the majority (87.3%) held a neutral attitude. According to Ahmed and Hani (2017), among 41 nurses in Minia, Egypt, the common nursing care practices towards NNJ included phototherapy, proper covering and shielding of gonad, appropriate positioning of neonates, and assessment and regulation of thermoregulation device. Similarly, Orimadegun and Ojebiyi (2017) conducted a study in Nigeria and reported that 46.4% of nurses engaged in incorrect practices towards NNJ. The study also found that community health workers, who are professionally trained, had higher odds of engaging in incorrect practices compared to community birth attendants, who are registered but non-professionally trained (Orimadegun & Ojebiyi, 2017). Orimadegun and Ojebiyi (2017) further added that only 35.5% of the nurses in their study correctly described the methods used to assess NNJ. The most commonly reported practices included examination of the eyes (96.7%), skin examination (71.1%), and examination of the palms and soles of the feet (52.1%) (Orimadegun & Ojebiyi, 2017). In Southwest Nigeria, Opara et al. (2014) reported that among 200 community health nurses, physical assessment of NNJ commonly included the eyes (94%), skin (77%), urine color (62%), and palms and soles of the feet (31%). However, Orimadegun and Ojebiyi (2017) reported that community health nurses were more likely to treat NNJ with drugs (50.2% vs. 21.2%), exposure to sunlight (23.8% vs. 9.8%), and glucose water (22.0% vs. 8.8%) compared to community birth attendants. Additionally, Ogunfowora and Daniel (2022) found that community health workers involved in neonatal care employed less effective drugs (13.4%), sunlight exposure (10.4%), and herbal preparations (3%) in the management of NNJ.
Studies on KAPs of NNJ among healthcare providers including nurses and midwives in Ghana appear dearth. Studies that have attempted to look at knowledge of NNJ in Ghana have much concentration on mothers (Adoba et al., 2018; Oppong et al., 2019; Owusu et al., 2018). As illustrated by Adoba et al. (2018), only 17.3% out of the of 150 mothers indicated awareness of NNJ. Their major source of information on NNJ comprised school (34.6%), with a great number (90%) of them having no idea NNJ has an effect on organs of the neonate (Adoba et al., 2018). Salia et al. (2021) revealed similar findings among 202 mothers in a teaching hospital. About 45.5% of mothers showed good knowledge of NNJ. Additionally, mothers with previous awareness and education on NNJ demonstrated higher odds of good knowledge on NNJ compared to those with none (Salia et al., 2021). A study at the Tamale Teaching Hospital involving 76 participants reported of maternal knowledge on NNJ to be 17.1% and their ability to identify the condition to be 11.8% (Abdul-Mumin et al., 2021). It reveals a low knowledge on NNJ among mothers in Ghana's context and may be a reflection of the kind of information expectant mothers receive during ANC and PNC clinics. Expectant mothers and mothers receive healthcare-related education and information from nurses and midwives during their ANC and PNC visits. The low level of knowledge could also reflect a seemingly lack of knowledge among nurses and midwives. Similarly, it may also reflect the priority areas for health education among expectant mothers and mothers at ANC and PNC.
Methods
Study Design and Setting
This is a hospital-based descriptive cross-sectional study, conducted between January 2021 and August 2021. The study was conducted in the Tamale Teaching Hospital, situated in the Tamale Metropolis, Northern Region, Ghana. The units/ included in the study were Child Welfare Clinic, Postnatal Clinic, Obstetrics Theater, Neonatal Intensive Care Unit, and the labor ward. These units were used because they are directly involved in the care of neonates. The Hospital has a bed capacity of 800, and serves as the only tertiary health facility in the northern parts of Ghana. The Hospital's annual deliveries are about 8000, and the Neonatal Intensive Care Unit admits approximately 3000 neonates per year (Tamale Teaching Hospital Profile, 2021).
Study Population
The accessible population for this study were nurses and midwives at the Tamale Teaching Hospital.
Inclusion and Exclusion Criteria for Nurses and Midwives
Participants were selected if they were either a nurse or midwife at the Tamale Teaching Hospital and at any of the following units of the Hospital; Child Welfare Clinic, Postnatal Clinic, Obstetrics Theater, Neonatal Intensive Care Unit, and the labor ward, and provided consent to participate in the study. Participants also needed to have a minimum of one-year clinical experience working in pediatric or obstetric care. Participants were excluded if they did not work in the Tamale Teaching Hospital and in the selected units (Child Welfare Clinic, Postnatal Clinic, Obstetrics Theater, Neonatal Intensive Care Unit, and the labor ward). Participants with less than a year clinical work experience and on clinical rotations were equally excluded.
Sample Size and Sampling Technique
Using a finite sample size estimator, the sample size was determined by employing the Yamane (1967) sample size estimator given as n = N/N + 1(e)2. Using the five units (Child Welfare Clinic, Postnatal Clinic, Obstetrics Theater, Neonatal Intensive Care Unit, and the labor ward), total nurse and midwifery population of 235, the estimated sample size was (n) = 235/(1 + 235(0.052) = 147.4. Estimating a 10% nonresponse rate of 147, 147 was multiplied by 0.10 (which is equivalent to 10/100 or 1/10) = 0.10 × 147 = 14.7. Therefore, the estimated sample size was 161.2 (14.7 + 147.4) = 161.2, approximately 162 participants.
Eligible participants were selected through simple random sampling by means of Excel-generated random numbers using the list of nurses and midwives as a sampling frame.
Data Collection Tools and Collection Process
An electronic structured questionnaire (Google form) was created to collect data from participants. The form was developed to allow only one data submission by a participant by activating the one submission per a device option in the Google form setting. The questionnaire was developed after a careful review of four other related studies (Adoba et al., 2018; Aggarwal et al., 2017; Egube et al., 2013; Lake et al., 2019). The questionnaire had four main sections: sociodemographic characteristics, knowledge, attitude, and practices on the management of NNJ and designed to ensure participants attempted all questions and items. Questions and items that were not applicable were allowed the option of skip.
A generated link for the Google form was shared with participants who met the inclusion criteria via emails and WhatsApp contact where applicable. Participants were encouraged not to share the link of the electronic questionnaire with anyone or to other public platforms.
Using the mean scores as the cut-offs, the KAPs were categorized as “good” and “poor.” A correct response attracted a score of 1 and an incorrect response attracted a score of 0. The sum of the variables included in the computations for the scoring and means were determined. Based on the mean scores, participants were categorized as having “good knowledge and poor knowledge,” “good attitude and poor attitude,” and “good practices and poor practices.” The method of scoring and categorization has been employed in other related studies (Abdul-Wahab et al., 2021; Salia et al., 2021).
As an illustration, knowledge towards NNJ has 10 questions with 27 variables and was computed for the mean score of 13.5. A participant with a mean score of 13.5 (≥50%) or more was considered as having “good knowledge” towards NNJ. Participants who scored below the mean score of 13.5 (<50%) were categorized as having “poor knowledge” towards NNJ.
There were five questions on attitudes towards NNJ with nine variables. The mean score computed for attitudes towards NNJ was 4.5. Participants who scored 4.5 (≥50%) or more were considered as having “good attitude” towards NNJ. Participants who scored below the mean score of 4.5 (<50%) were categorized as having “poor attitudes” towards NNJ.
There were four questions on practices towards NNJ with 14 variables. The computed mean score was therefore 7. Participants who scored 7 (≥50%) or more were categorized as having “good practices” towards NNJ. Participants who scored below the mean score of 7 (<50%) were categorized as having “poor practices” towards NNJ.
Data Validity and Reliability
The content validity and instrument reliability were assessed through:
Expert review: The research instrument was reviewed by experts in the field of pediatrics and neonatal health to ensure that the questionnaire covers key and relevant items to achieve the objectives of the study.
Pilot testing: The questionnaire was pretested in a related health facility in the Tamale Metropolis among 20 nurses and midwives. This was to ensure that the questionnaire was clear, understandable, and relevant to the research questions. The outcome of the pretest was used to modify the data collection tool where necessary to meet the research objectives.
Face validity: Researchers conducted a subjective evaluation of the instrument to ensure that it appears to measure the intended objectives.
Test-retest reliability: Subsequently, the authors re-administered the instrument to the same group of individuals involved in the initial pilot study and compared the results to ensure consistency.
Ethical Consideration
The ethical and administrative approvals to conduct the study were obtained from the Institutional Review Board of the University for Development Studies, Tamale Campus (UDS/RB/ 004/21) and the Research and Development Department of the Tamale Teaching Hospital (TTH/R&D/SR/045), respectively. In addition, written informed consent was obtained from all participants prior to recruitment. Participants were assured of the confidentiality and privacy of information they provide and non-use of direct identifiers, including names or initials to trace their responses.
Data Management, Statistical Analysis, and Presentation
The online submitted data was downloaded and converted into a Microsoft Excel File. The data was subsequently cleaned and checked for completeness before exporting onto Statistical Package for Social Science (SPSS) version 25. A total 202 participants were selected and included in the data analysis. The 202 participants were selected to increase the statistical power to demonstrate a true effect and show precise estimates of the population parameters, such as means and standard deviations. The increased sample size equally improved the generalizability of the study population.
A descriptive analysis, including mean, standard deviations, frequencies, and percentages, was performed to give general description of the variables. Simple Pearson Chi-square test, Fisher's test, and logistic regression models were performed to test the level of associations between the outcome and independent variables and predictors for NNJ. The tests of associations were confirmed at 5% level of significance. A p-value of <.05 was considered statistically significant. The data summary was presented in tables for clarity.
Results
Sociodemographic Characteristics of Nurses and Midwives
A total of 202 nurses and midwives participated and were included in the data analysis. The mean age of participants was 30.6 ± 3.8 years, and majority were in the age category of 21–30 years (53.0%) and females (71.3%). Majority of the participants were with diploma in nursing/midwifery educational background (59.9%), staff nurse/midwife (56.4%), had ≤5 years of work experience (89.1%), and were in Neonatal Intensive Care Unit (25.2%) (Table 1).
Sociodemographic Characteristics of Nurses and Midwives.
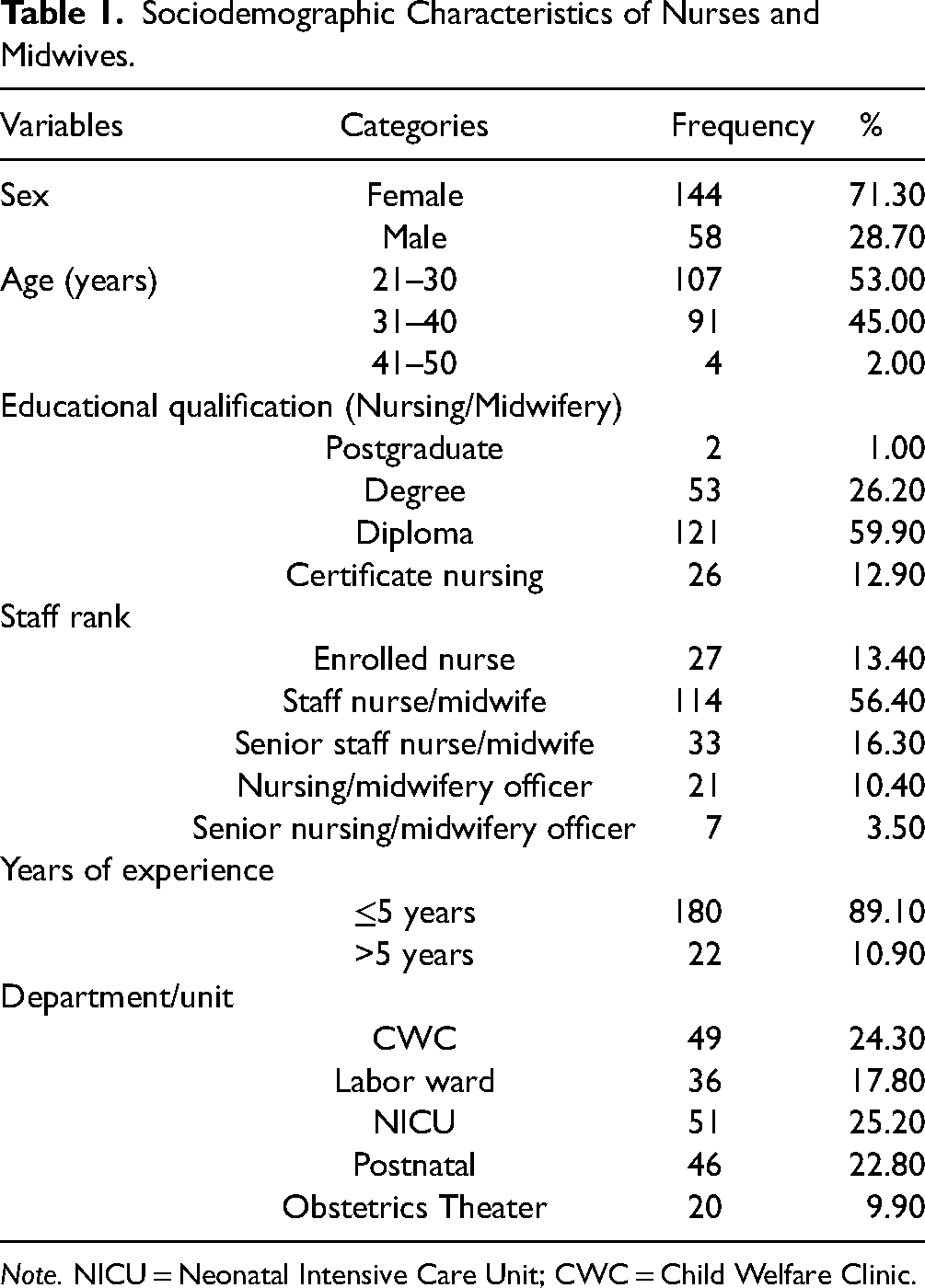
Note. NICU = Neonatal Intensive Care Unit; CWC = Child Welfare Clinic.
Knowledge of Neonatal Jaundice Among Nurses and Midwives
The overall knowledge score was good knowledge (69.30%) and poor knowledge (30.70%). Out of the 202 participants, 65.80% defined NNJ as yellow discoloration of sclera of the eye and 34.20% defined NNJ as yellow discoloration of the skin of the neonate. Common causes or risk factors of NNJ indicated comprised massive RBCs destruction (56.90%), low levels of albumin (53.50%), and short lifespan of RBCs (48.00%). Majority indicated that NNJ can be detected at serum bilirubin levels of 5–7 mg/dl or greater (96.50%). Most of the participants indicated that the blood group implicated in NNJ was mother ARH (+), father ORH (+) (49.0%). Commonly mentioned signs and symptoms of NNJ included discoloration of the skin, nails and eyes (100.00%), poor feeding (55.90%), seizures (43.10%), and arching of the back (37.60%). The most common source of information on NNJ was on the job training (57.90%) (Table 2).
Knowledge of Neonatal Jaundice Among Nurses and Midwives in the Tamale Metropolis.

Note. NNJ = neonatal jaundice.
Not included in the scoring.
Nurses and Midwives’ Attitudes Towards Neonatal Jaundice in the Tamale Metropolis
Overall, good attitude towards NNJ was 64.90%. Majority of the participants (81.20%) indicated nurses and midwives are responsible for the care of NNJ and such care includes cover neonate's eye during phototherapy (92.60%), assess the neonate skin for early detection of the condition (75.70%), and encourage mothers to initiate breastfeeding immediately after birth (81.20%). Majority of the participants indicated that NNJ can be prevented (88.10%) and (99.50%) asserted that NNJ cannot be treated with oral water and sugar. Less than half of the participants indicated that physiological jaundice can be treated at home with early morning sun (27.20%) (Table 3).
Nurses and Midwives’ Attitudes Towards Neonatal Jaundice in the Tamale Metropolis.
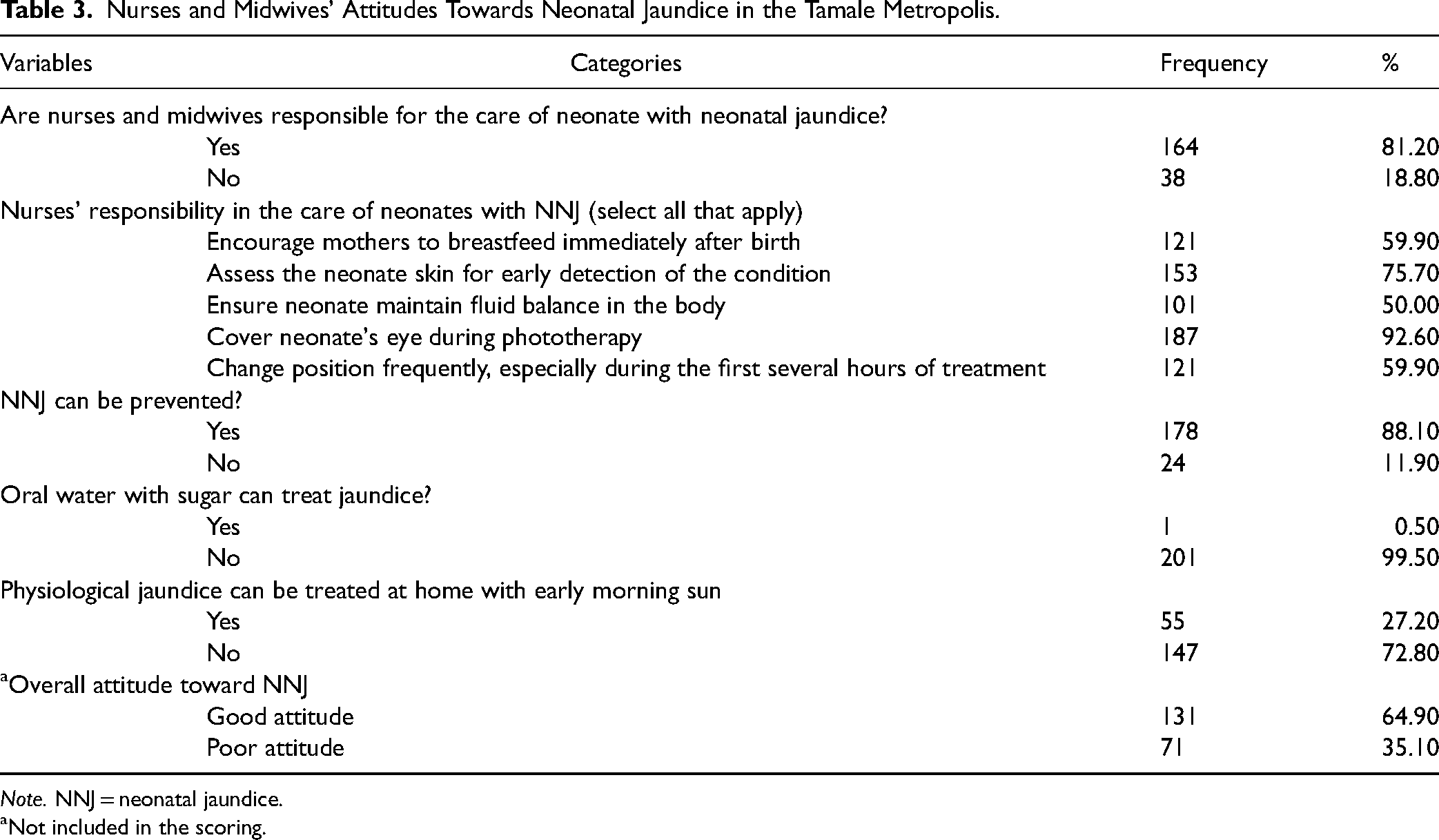
Note. NNJ = neonatal jaundice.
Not included in the scoring.
Nurses and Midwives’ Practices Towards Neonatal Jaundice in the Tamale Metropolis
The overall good practices towards the management of NNJ were 62.90%. Majority of the participants have less than five years of work experience (196, 97.00%) with more than half indicating involvement in the care of NNJ (57.40%). To check for babies for NNJ, common practices employed included checking for the yellow color of the skin, nail and sclera of the eye (100.0%), and looking at the palms or soles of the foot (47.00%). Common nursing care practices during phototherapy includes covering eyes with eye patches to prevent eye injury (95.0%), eye patches should be loose enough to avoid pressure (74.30%), and close eyes before applying eye patches (72.80%) (Table 4).
Nurses and Midwives’ Practices Towards Neonatal Jaundice in the Tamale Metropolis.
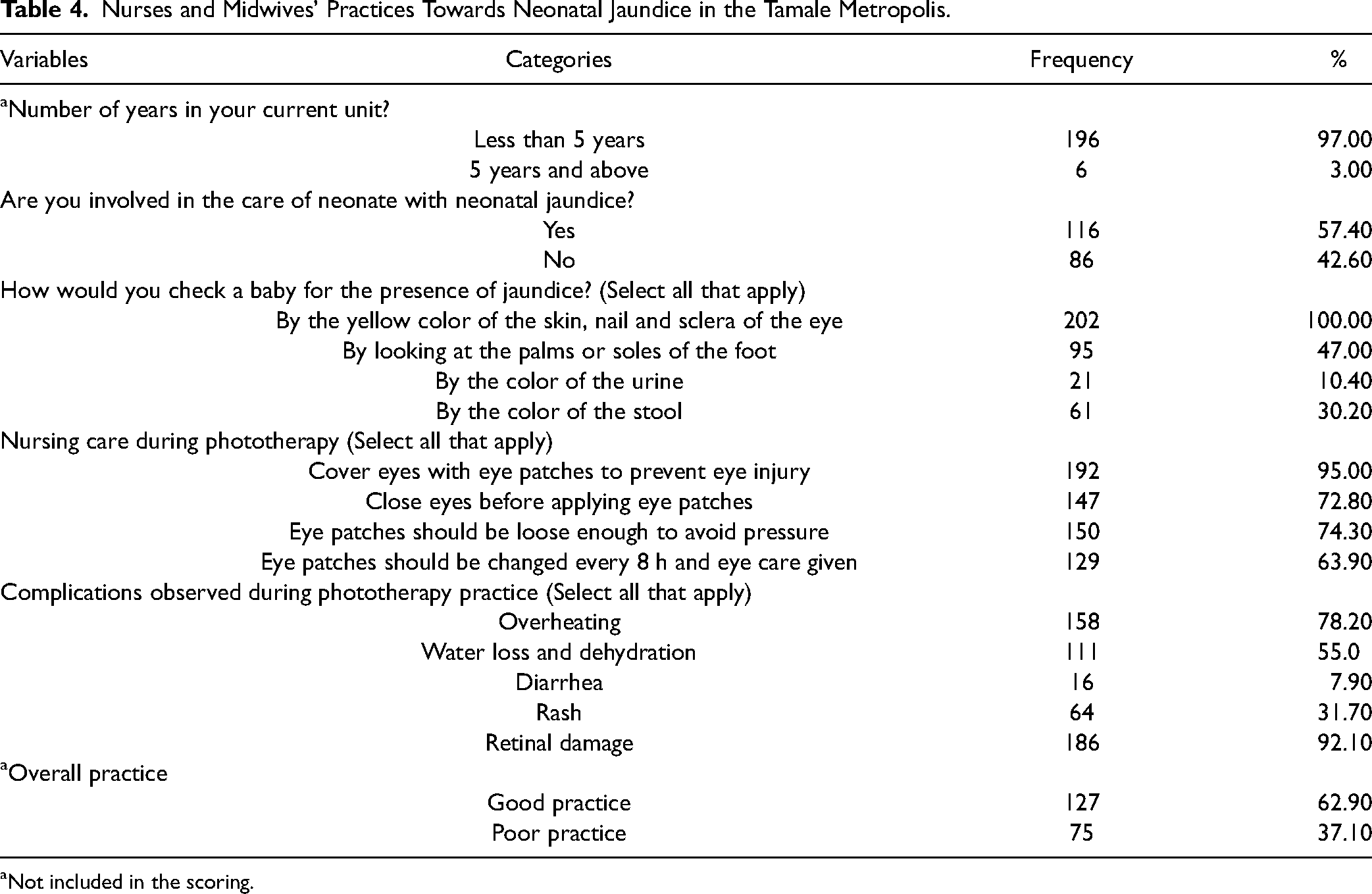
Not included in the scoring.
Association Between Knowledge, Attitude Towards Neonatal Jaundice, and Sociodemographic Characteristics
The study found significant differences between knowledge and age (p < .001), educational qualification (p = .024), rank (p < .001), and current unit (p = .02). With Attitudes, there were significant differences between attitudes and age (p < .001), education qualification (p = .013), rank (p < .001), and current unit (p = .018) of study participants as shown in Table 5.
Association Between Knowledge, Attitudes and Sociodemographic Characteristics.

Predictors of Practice Towards NNJ Management
Independently, age (p < .001), rank (p < .012) and current unit (p = .044), overall knowledge (p < .001), and overall attitude (p < .001) were statistically significant with the practices of study participants towards NNJ. After adjusting for other variables, good knowledge (adjusted odds ratio [AOR] = 22.41(10.21–49.18) p < .001) and good attitude (AOR = 25(11.86–55.07) p < .001) were positively associated with practices towards NNJ (Table 6).
Predictors of Good Practices Towards Neonatal Jaundice Management.

Note. AOR = adjusted odds ratio, COR = crude odds ratio, Ref*= Reference category.
Discussion
The study assessed the KAP of nurses and midwives towards NNJ in the Tamale Teaching Hospital. The overall knowledge of NNJ among the study participants was proportionally significant. This finding is particularly important as nurses and midwives play an important role in the provision of care to mothers and their neonates in the first week of life, including predischarge assessment, education on jaundice detection, and post-discharge follow-up. Their adequate knowledge towards NNJ is hence essential to assess and prompt immediate and appropriate management to prevent complications associated with the disease (Maisels, 2006).
The burden of NNJ is significant and is associated with mortality and morbidity in developing countries. A major challenge that leads to serious complications (kernicterus and death) in these settings is the inability of providers to assess and detect jaundice early and institute timely treatment. The high knowledge among participants is therefore important in aiding early diagnosis to reduce the incidence of severe NNJ in the study setting (Abdul-Mumin et al., 2021) and the complications accompanying it. However, it is imperative to address the poor knowledge observed in some of the participants in the study, as this could impact negatively on the care they provide to neonates and lead to poor outcomes (Ayete-Nyampong & Udofia, 2020; Demis et al., 2021; Hannon et al., 2001; Opara et al., 2014).
Attitudes demonstrated by health workers have both positive and negative implications for healthcare delivery. Positive attitudes of healthcare workers have been described to influence good health seeking behaviors of mothers, pregnant women, and health service delivery (Al-Mutair et al., 2014; Andersen, 2004; Dapaah, 2016; Sokoloff et al., 2020). The findings showed that majority of the study participants had good attitudes towards NNJ. This is important to ensure appropriate management of the condition especially in the study area. Some essential attitudes towards NNJ documented in the study included the indication that nurses and midwives are responsible for the care of NNJ, acknowledgement of the key role of nurses and midwives in early detection of NNJ through physical examination, and covering the neonate's eye during phototherapy. The recognition and acceptance of nurses’ responsibilities and roles in the care of neonates with jaundice will have a positive treatment outcome. Another important attitude highlighted in this study by participants comprised the encouragement of mothers to breastfeed their neonates immediately after delivery. This finding is important in improving hydration and passage of stools, and hence reducing risk of severe jaundice (Abie & Goshu, 2019; Mary et al., 2022). However, more than one-fourth of the participants showed poor attitudes towards NNJ. This can affect the quality of care provided to neonates presenting with jaundice in the study area, if not addressed. Previous studies in Ghana have highlighted the poor attitudinal behaviors of health workers, including nurses and midwives, towards patients of all age groups (Amponsah et al., 2019; Asare et al., 2022; Dapaah, 2016; Lamptey, 2022; Sokoloff et al., 2020). For example, Andersen (2004) reported in a study on the differential treatments of patients that most nurses and midwives attend to patients with low level of education unprofessionally compared to persons with higher educational qualifications. The finding on poor attitudes of nurses and midwives and that of previous studies should be addressed through multiple approaches including in-service training on good clinical practices and professional conducts.
Detection of NNJ should be followed by immediate and appropriate management to prevent associated complications. The practice score towards the management of NNJ was significant among the study participants. The good practices of the participants have the potential to affect positively the quality of care given to neonates and their mothers in the study setting. This is important as harmful practices in the management of NNJ are common among healthcare workers and these practices may be taught to parents following birth.
To conceptualize interventions to address the poor KAP, important factors such as age, educational qualification, rank and current unit of nurses and midwives should be taken into consideration. For example, the sociodemographic characteristics of the participants showed that most had less than five years of work experience. It is therefore important to assign nurses and midwives with less experience to more senior and experienced colleagues for the purposes of nursing mentorship especially towards the care for NNJ. Similarly, nurses and midwives with higher educational qualification and in the senior rank positions can be used to train staff with qualifications lesser than first degree and in the junior rank categories. A previous study highlighted positive association between senior healthcare cadre and level of knowledge and skills (Ameh et al., 2016). Adjusting for other variables, the findings showed that good knowledge and good attitude were positively associated with practices towards NNJ. These findings explain the need to place much emphasis on lifelong learning among nurses and midwives in healthcare facilities.
Strengths and Limitation
The study provides maiden data on the KAP of nurses and midwives towards NNJ in the study setting. The gaps identified, including the poor knowledge, poor attitudes, and poor management practices towards NNJ, give enough basis for targeted interventions such as in-service training and mentorship. This is a cross-sectional study, and therefore making cause and effect inferences is not applicable. Again, the study was conducted in a single facility and therefore, making generalizations on the findings and conclusions among nurses and midwives countrywide is limited. However, the study has demonstrated a need to build capacity on nurses’ KAPs towards the management of NNJ.
Implications for Practice
NNJ is a common condition that affects many newborns, and it can lead to severe complications if not managed properly. The KAP are important factors that influence the quality of care provided by nurses and midwives, especially when it comes to managing NNJ.
Knowledge forms the foundation for providing effective care. The study highlighted gaps in knowledge on NNJ. It is therefore important to provide nurses and midwives with comprehensive understanding of NNJ including the causes, risk factors, signs and symptoms, potential complications, and appropriate management strategies in the study setting.
Positive attitudes are essential for providing compassionate and patient-centered care. Substantial number of the participants demonstrated poor attitudes towards NNJ. The study highlights the need for nurses and midwives to be given training on how to maintain a supportive and empathetic attitude towards parents and their newborns affected by jaundice.
Appropriate practice is the application of the knowledge and attitudes in clinical settings. Nurses and midwives should be given the required NNJ training, and by targeting individuals with less experience as highlighted in this study to implement evidence-based protocols and guidelines for the screening, assessment, and management of NNJ.
Conclusion
The participants demonstrated substantial KAPs towards NNJ. However, there exist some gaps in all three domains that need to be addressed to improve neonatal health outcomes in the study area.
Footnotes
Acknowledgments
The authors wish to thank the management of the Tamale Teaching Hospital and the study participants for the permission to conduct and acceptance to be part of the study.
Author Contributions
Authors DRD and AAM conceived the study and designed the study protocols in collaboration with Authors EKD and SZ. Authors DRD, EKD, and MNA wrote the first draft of the manuscript. Authors MNA and EKD performed the data analysis. Authors AAM and SZ supervised the study and performed the critical review of the study. The final manuscript was read and approved by all authors.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Consideration
The ethical and administrative approvals to conduct the study were obtained from the Institutional Review Board (IRB) of the University for Development Studies, Tamale Campus (UDS/RB/004/21) and the Research and Development Department of the Tamale Teaching Hospital (TTH/R&D/SR/045), respectively. In addition, written informed consent was obtained from all participants prior to recruitment. Participants were assured of the confidentiality and privacy of information they provide and non-use of direct identifiers, including names or initials to trace their responses.
Data Availability
Data will be available upon request to the corresponding author via doreen.donkorone@gmail.com and edzantor21pg@sph.uhas.edu.gh.