
Abstract
Background
Age and multiple comorbidities have been reported to influence the case fatality rate of COVID-19 worldwide, so also in Malaysia; however, to date, no scientific study among the local population has been published to confirm this. This study aimed to determine the overall demographics and clinical characteristics of COVID-19 non-survivors in Malaysia, stratified by age (< 65 vs. ≥ 65 years old). The mortality was also compared between two half-year periods: March–August 2020 and September 2020–March 2021.
Method
Daily reports containing demographics and medical history of COVID-19 non-survivors from March 2020 to March 2021 were obtained from the Malaysian Ministry of Health website. All information was extracted retrospectively and analysed using descriptive and inferential statistics with SPSS.
Results
Of 1192 COVID-19 non-survivors, the overall mean (SD) age was 64.8 (15.7) years, with 64.7% male. Death was seen mostly among 50- to 64-year-olds (33.1%) and 65- to 74-year-olds (24.8%). The presence of underlying hypertension (61.8%) and diabetes mellitus (48.2%) were the most common comorbid diseases encountered in the COVID-19 non-survivors. Underlying hypertension, stroke, heart disease and dyslipidaemia were significantly higher among COVID-19 non-survivors who were ≥ 65 years old compared to those < 65 (p < 0.05). Mortality was a lot higher in September 2020–March 2021 compared to March 2020–August 2020 (91.3% vs. 8.3%).
Conclusion
Older age, male gender and the presence of multimorbidity (hypertension, diabetes mellitus, stroke and heart disease) are risk factors that contribute to mortality due to COVID-19 in Malaysia, especially among those ≥ 65 years old.
Introduction
In December 2019, an outbreak of novel coronavirus SARS-CoV-2 started in Hubei Province in the People’s Republic of China and spread to many other nations. Due to the rapid spread and severity of the virus, the World Health Organization (WHO) declared COVID-19 as a pandemic on 11 March 2020. 1 The causative agent of COVID-19 disease is the novel coronavirus known as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). 2 The pathogenic coronavirus, including SARS-CoV-2, belongs to the Betacoronavirus genus, group 2. 3 Novel coronavirus SARS-CoV-2 is a single-stranded, enclosed RNA virus that transmits from animals to humans. 4 Their source is probably bats or pangolins, which was first discovered in Wuhan, China. 5 However, a study reported that the highly pathogenic viruses of SARS-CoV-2 can be transmitted through air droplets and aerosols from human to human. It is suspected that it travels from person to person through respiratory droplets by inhalation and ingestion. 6 In addition, direct contact by touching an infected subject also can transmit the virus to another person. Furthermore, the virus can be transmitted through faecal-oral transmission. 7
The clinical manifestation of COVID-19 disease varies from flu-like symptoms to severe respiratory illness that leads to death. COVID-19’s clinical manifestations are divided into three major patterns: mild illness with upper respiratory tract-presenting symptoms, non-life-threatening pneumonia and severe pneumonia with acute respiratory distress syndrome (ARDS). 8 Common symptoms of COVID-19 illness are similar to flu-like symptoms such as fever, headache, nausea, sore throat, tiredness and cough. Other symptoms may include mild to severe pneumonia, loss of sense of taste and smell, myalgia and dyspnoea. 4 Besides, there are also asymptomatic individuals who do not develop any symptoms or do not feel unwell. 9 The symptoms usually appear 2–14 days after exposure to the infection. 6
COVID-19 can affect all ages, but older people and those with comorbidities such as hypertension, diabetes mellitus and cardiovascular disease are at the highest risk of getting severe disease leading to death. According to the U.S. Centres for Disease Control and Prevention (CDC), the case fatality rate in the elderly group is higher compared to children and working-age adults. 10 A spike in the number of new cases and rapid spreading of the virus has led to an increase in mortality. Globally, COVID-19 has infected over 219 million people, and there have been more than four million deaths associated with COVID-19 as of 9 October 2021. 11 Around 215 countries worldwide are affected and struggling with COVID-19. The United States of America, Brazil and India remain the three countries with the highest number of deaths due to the COVID-19 outbreak. 12
COVID-19 status in Malaysia
Malaysia reported its first imported case on 25 January 2020. It involved three Chinese nationals who had previously been in Singapore and had close contact with an infected person. 13 On 24 January 2020, they arrived in Malaysia through Singapore. 14 On 4 February 2020, the first Malaysian who was confirmed with COVID-19 was a 41-year-old man who had just returned from Singapore, who became ill with symptoms of fever and cough. 15 Following new cases of COVID-19, the Malaysian Ministry of Health (MOH) took strict action to prevent the spread of COVID-19 around the country by creating standard operating procedures (SOPs) to manage the outbreak. This involved the implementation of Movement Control Orders (MCOs) (2020) after the persistent increase in COVID-19 cases, requiring the closure of all businesses except those providing essential services. On 9 July 2020, Malaysia recorded two consecutive days of zero local transmissions of COVID-19, 16 indicating the success in implementing MCOs in terms of flattening the curve of COVID-19 cases.
A year after the first case of COVID-19 in Malaysia, on 24 January 2021, 183,801 total confirmed cases had been reported, with 678 deaths related to COVID-19. 17 To date, Malaysia has battled with three waves of COVID-19. The first wave was from 25 January to 15 February 2020, where a total of 22 cases were reported, with no deaths and complete recovery in all cases. The second wave was from 27 February 2020 until 30 June 2020 with 8639 cumulative cases and 121 deaths. 18 The largest contribution to the second wave of COVID-19 was a cluster linked to a religious procession organised by the Tablighi Jamaat in Sri Petaling, Kuala Lumpur. 19 This led to a significant increase in local cases as well as the export of cases to neighbouring countries. A sudden increase in new cases as well as a number of deaths led the government to implement MCOs in order to break the chain of COVID-19. The third wave is from 3 October 2020 until the present, with 14,638 confirmed cases on 8 October 2020 and a peak on 28 August 2021 with 263,903 active cases and 15,802 cumulative fatalities. The case fatality rate has risen in line with the number of new cases of COVID-19. As of 18 October 2021, Malaysia had suffered 27,921 deaths (1.2% overall case fatality rate) associated with COVID-19. 20 To date, the infectious rate of COVID-19 or R-Naught in Malaysia is 0.88, with a total of 2.38 million cases reported. 21 Despite that, scientific reports on the characteristics of local patients dying from COVID-19 are not available. Thus, this study aims to determine the demographics and clinical characteristics of COVID-19 related deaths in Malaysia within the first year of the pandemic (March 2020–March 2021). The second aim of this study is to compare the mortality among different age groups (< 65 years old vs. ≥ 65), and the third is to compare mortality in Malaysia in two half-year periods (March–August 2020 vs. September 2020–March 2021).
This information is useful to understanding the Malaysian population who have been severely affected by the SARS-CoV-2 virus, leading to death, which will allow further action to be taken to resolve this issue.
Research Methodology
Data Collection
Reports from the MOH with information on COVID-19 mortality were used to obtain the information on the prevalence of COVID-19 mortality and the clinical characteristics of COVID-19 non-survivors. These reports are updated daily and can be assessed by the public any time at http://covid-19.moh.gov.my Flowchart of data selection and collection.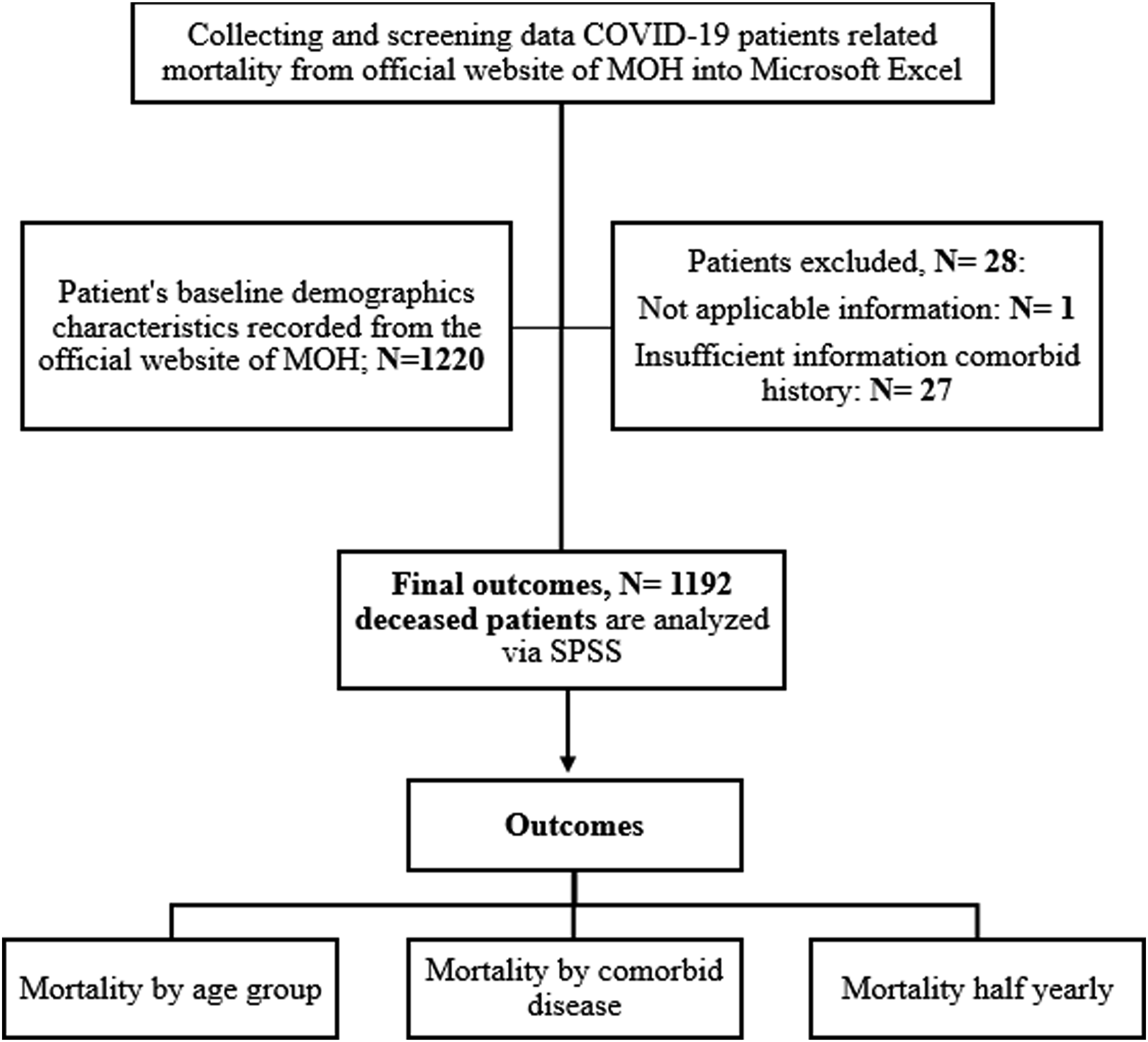
Statistical analysis
Descriptive statistics were used to determine the number of patients who died as well as their demographic and clinical characteristics. Comparisons between two age groups (< 65 vs. ≥ 65 years old) were tested using a chi-square test. Categorical variables were presented in counts and percentages, and continuous variables were presented as mean (SD) after normality testing was performed. All analyses were conducted using the Statistical Package for the Social Science (SPSS). Statistical significance is taken to be when the p value < 0.05.
Ethical Approval
This study was approved by the UiTM Research Ethical Committee. Permission to collect data from MOH was not required as it involved data in the public domain (Reference number: REC/06/2021 (UG/EX/352) issued on 21 June 2021).
Result
Demographics of COVID-19 mortality, N (%) in the overall population and stratified according to age categories of < 65 years vs ≥ 65 years.

When compared to different age group categories, death was mostly seen among the 50- to 64-year-olds’ (33.1%) category, followed by that of 65- to 74-year-olds (24.8%) (Figure 2). Patients < 17 years old were less likely to die (0.4%) from COVID-19 than other age groups (Figure 2). In terms of gender, it can be seen that males (64.7%) are more likely to die due to COVID-19 than females (35.3%). Regarding comorbid diseases, hypertension (61.8%) and diabetes mellitus (48.2%) were the most common diseases encountered in deceased patients. This is followed by kidney disease (22.9%), heart disease (21.1%), dyslipidaemia (14.4%), stroke (10.6%), lung disease (8.1%) and obesity (4.8%). The least prevalent comorbid diseases in deceased patients were tuberculosis (1.4%), liver disease (1.2%) and hyperthyroidism (0.6%) (Figure 3). As seen in Table 1, when compared between age groups < 65 years old and ≥ 65 years old, males were more likely to die due to COVID-19 compared to females in both age categories. Hypertension (68.2% vs. 55.5%; p =< 0.001), heart disease (25.0% vs. 17.1%), dyslipidaemia (17.6% vs. 11.3%; p < 0.001) and stroke (13.9% vs. 7.2%; p < 0.001) were significantly more prevalent among deceased COVID-19 patients in the ≥ 65 years old category compared to the < 65 years old category. However, obesity is significantly more prevalent in the younger age category compared to the ≥ 65 years old category (8.1% vs. 1.6%; p =< 0.001). There is no significant difference in other types of comorbidities like diabetes mellitus, kidney disease and lung disease between both age groups. In terms of the proportion of deaths due to COVID-19 stratified by 6-month intervals (September 2020–March 2021 vs. March–August 2020), it is apparent that mortality was much higher in September 2020–March 2021 than in March–August 2020 (91.3% vs. 8.3%). Proportion of mortality by age group. Percentage of mortality by comorbid disease (total percentage is more than 100% because some patients are with multiple comorbidities).

Discussion
This retrospective study described the demographic and clinical characteristics of 1192 patients who died from COVID-19 from March 2020 to March 2021 in Malaysia. The demographics of deceased COVID-19 patients were largely consistent with previous research, 22 whereby mortality increases with age especially those aged 50–64 years. 23 The case fatality rate related to COVID-19 is several times higher for the elderly than for the young. One of the factors that contribute to the increased risk of death in the elderly is the presence of comorbidities, as the average number of comorbid conditions grows gradually with age. 24 Generally, elderly populations have several medical problems in addition to changes in their physiological system. Studies from China show the median age of death is higher (72 years) than the Malaysian population (mean age, 65 years), probably because the proportion of older age population is greater in China.25,26 Older age has been identified as a major mortality predictor in COVID-19 patients since the outbreak began. According to early Chinese statistical data, the case fatality rate rises sharply beyond the age of 60, reaching 14.8% in individuals over the age of 80. 27 A similar pattern was seen in other COVID-19 affected nations. Several studies have found that advanced age is a major risk factor for COVID-19 death.28,29 A study from Jakarta, Indonesia, also stated that the majority of deaths due to COVID-19 were among the elderly. 30 The median age of deceased patients was lower than the current study, namely, 58 years old, where most (78%) of the deceased patients were ≥ 50 years old. More than half (62%) of the elderly who died had a history of comorbidity: 30% had 1 comorbidity and 32% had > 1 comorbidities, specifically hypertension, diabetes, cardiac disease, chronic kidney disease and liver disease. 30
Although epidemiological studies reveal a difference in mortality rates between men and women among people diagnosed with COVID-19, the reasons behind the gender difference in mortality remain unknown.31,32 This is because a combination of biological, behavioural and psychosocial factors results in the difference in health issues. While both men and women are susceptible, men (64.7%) are more likely to die from COVID-19, according to the current study. A study from Italy also reported the number of deaths related to COVID-19 were mainly among males (70.6%).33,34 Similarly, two studies from China indicated the deaths related to COVID-19 were mostly males.35,36 There are a number of possible reasons for this. Women, who carry the X chromosome, have a high density of immune-related genes, resulting in a biological difference which could contribute to faster pathogen clearance than in males. 37 Women have higher innate and adaptive responses, resulting in better immune responses than men. 38 This could be the possible reason for females being less likely to be affected by COVID-19. Furthermore, the level of the plasma angiotensin-converting enzyme 2 (ACE2) receptor responsible for the entry of the virus into the host cell is higher in males than females, which could also potentially explain this difference in mortality rate between genders. 39 Another possible reason is men’s high-risk behaviour (alcohol consumption and smoking) and occupational exposure, with men being more exposed to the disease at work. 40
In this study, it can be seen that significantly more deaths occur in patients with underlying diseases, especially hypertension, diabetes mellitus, kidney disease and heart disease. When death is stratified according to different age groups (≥ 65 years old vs. < 65 years old), a similar pattern can be seen whereby underlying hypertension (68.2% vs. 55.5%; p = < 0.001), heart disease (25.0% vs. 17.1%), dyslipidaemia (17.6% vs. 11.3%) and stroke (13.9% vs. 7.2%) are significantly more prevalent among the elderly. There are other factors that influence the fate of COVID-19 patients that are independent of age. The existence and number of comorbidities, in particular, is a crucial factor in predicting death in both the elderly and the young. 41 According to a study by Surendra et al., 30 COVID-19 patients who died (median age = 58 years old) were commonly associated with a history of comorbidities, especially hypertension (42%), diabetes mellitus (29%), cardiac disease (22%) and kidney disease (9%). A similar study finding was observed in China, where the most prevalent comorbidity was hypertension (50%), followed by diabetes (25%)and ischaemic heart disease (18.5%), as seen in deceased patients with a median age of 70 years. 42 According to the Centers for Disease Control and Prevention (CDC), adults of any age who have a history of medical conditions are more likely to become severely sick as a result of COVID-19. 43 Severe sickness implies that a COVID-19 patient may require hospitalisation or even die. Thus, the presence of underlying medical conditions is associated with the high risk of death due to COVID-19.
This study revealed that in Malaysia, the rate of mortality was higher in September 2020 to March 2021 compared to March to August 2020 (91.7% vs. 8.3%). The increase in mortality in the later period might have been influenced by the rise in the cumulative number of COVID-19 cases and SARS-CoV-2 mutation over time. This is evidenced by the discovery of many new strains of the coronavirus found in Malaysia. For example, new variants of COVID-19 from India, the United Kingdom, Brazil, South Africa and several other countries, which are more virulent, have been found in Malaysia during the third wave of COVID-19. 44 In addition, on 9 October 2020, the D614G-type mutation was discovered in virus samples by Malaysia’s Institute of Medical Research (IMR). The D614G genotype is easily spread and has a greater infection rate. 45
Rapid spreading of the COVID-19 virus among Malaysians led to a spike in mortality rate between September 2020 and March 2021. Another possible factor that contributed to the higher mortality rate from COVID-19 in this period is political issues. On 18 November 2020, Malaysia’s former Prime Minister, Tan Sri Dato' Haji Muhyiddin bin Haji Mohd Yassin, confirmed that the September state election in Sabah was the cause of the country’s newest wave of COVID-19 infections. 46 To be exact, multiple factors relating to the agent, host and environment are responsible for the increasing number of new cases as well as number of deaths related to COVID-19. Thus, to flatten the curve, Malaysia has implemented prevention measures such as isolation and social distancing. 47 For example, Movement Control Orders (MCOs) were implemented where the infection rate was high, especially in red zone areas. During MCOs, restrictions on movement, assembly and international travel, as well as closure of businesses, industries, public sector and educational institutions, were enforced. Furthermore, strict Enhanced Movement Order Controls (EMCO) were implemented in areas that contributed to the largest infection rate for 14 days. During EMCOs, restrictions were made whereby all residents within the area were banned from leaving their homes, non-residents and visitors were not allowed to enter the areas, all businesses were closed and all roads were blocked. In these 14 days, adequate food supplies were given by authorities to all residents, and medical bases were established within the areas. 48 In addition, individuals who needed to cross district or state borders for specific reasons had to first acquire permission. Apart from that, the government imposed entry and movement restrictions on all foreign nationals. 49
Following the dynamic transmission of new variants of COVID-19, it is essential for the community to follow all the standard operation procedures set by the government, including wearing a mask in public, social distancing, avoiding crowded places and seeking medical advice if they have any symptoms related to COVID-19. Furthermore, the government has also enhanced the vaccination rate among Malaysians to achieve herd immunity. As of 17 October 2021, at least 93.8% of Malaysian adults (21,960,911) had received complete vaccination doses, 50 resulting in a decline in number of COVID-19 cases (as of 17 October 2021: 6145 daily cases) and death rates (7 cases of daily death).
This study has some limitations: 28 out of 1220 patients were excluded because information on their medical history was not available from the Ministry of Health website. Apart from that, this study compared the case fatality rate of COVID-19 between March 2020 to March 2021, and hence, the most current mortality comparison (Oct 2021) was not available.
Conclusion
The risk factors associated with COVID-19 mortality in Malaysia are advanced age and the presence of comorbidities. Hypertension and diabetes mellitus are comorbidities that are seen in deceased COVID-19 patients. This emphasises the importance of effective prevention strategies, such as encouraging acceptance of the COVID-19 vaccination and adhering to standard operating procedures (SOPs) to reduce the infection and mortality rates among the high-risk population.
Footnotes
Acknowledgements
The authors would like to acknowledge Faculty of Pharmacy UiTM, lecturers, family and friends for their endless support in completing this manuscript. Also, to all the doctors, nurses, healthcare providers and front liners who have been tirelessly managing these COVID-19 patients during their hospital stay. Last but not least, to Malaysian Ministry of Health, who have made these data available in the public domain.
Author Contributions
Supervision: HHZ; Conceptualisation: HHZ; Methodology: LCM and HHZ; Project administration: HHZ; Data curation: SNAI, IAHZ, ZN, NSMH, LCM and HHZ; Formal analysis: SNAI, IAHZ, ZN, NSMH, LCM and HHZ; Writing - original draft: SNAI, IAHZ, ZN, NSMH and HHZ; Writing - review and editing: LCM and HHZ.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
This study was approved by the UiTM Research Ethical Committee. Permission to collect data from MOH was not required as it involved data in the public domain (Reference number: REC/06/2021 (UG/EX/352) issued on 21 June 2021).
Data Availability
All data have been presented in this manuscript.