
Abstract
Little is known about informal caregivers' challenges in medically underserved communities. This qualitative study explores their perceptions/experiences of caregiving in a medically underserved community in Midwest United States. Two focus groups (n = 12) were conducted and themes were extracted and analyzed. Theme 1 included perceived barriers/unmet needs; most prevalent of which were lack of informational resources and support groups. A second unsolicited and unanticipated theme highlighted how caregivers constructed meaning through reappraising challenges to create enriching experiences for themselves, reinforcing their evolving dyadic relationship with care-recipient. Challenging and enriching aspects of caregiving coexisted and were rooted in caregiver–care-recipient dyad. Caregivers used meaning-making as a coping strategy for challenges. Prior research corroborates caregivers' challenges and meaning-making; this study contributes by delineating how both become interrelated. Policy makers can (a) alleviate challenges by increasing informational resources and support groups and (b) provide training to optimize caregivers' meaning-making, thus enhancing their positive experiences.
Keywords
Introduction
Informal caregivers shoulder several responsibilities including providing health, medical, emotional, household, transportation, and financial support (Anderson et al., 2013; Lund, Ross, Petersen, & Groenvold, 2015; Wolff et al., 2017). They often act as surrogate decision-makers and manage care for recipients as a whole. Most often, caregivers provide this valuable service at the expense of their own well-being (Arno, Levine, & Memmott, 1999; Galiatsatos, Nelson, & Hale, 2017). Several studies have shown that caregivers are more susceptible to detrimental physiological and mental health effects than demographically similar noncaregivers (Johnson, Hofacker, Boyken, & Eisenstein, 2016; U.S. Department of Health and Human Services, 2015; Vitaliano, Zhang, & Scanlan, 2003). Schulz and Beach (1999) found that even after adjusting for sociodemographic factors, burdened or strained caregivers experience a 63% increase in mortality risk compared with noncaregiver controls.
The burden is largely attributed to the numerous unmet needs and barriers that informal caregivers encounter (Bee, Barnes, & Luker, 2009; Clayton, Butow, & Tattersall, 2005; Hudson, Aranda, & Kristjanson, 2004; Lafortune, Huson, Santi, & Stolee, 2015; Tallman, Greenwald, Reidenouer, & Pantel, 2012). Two types of needs—“instrumental” and “emotional”—have been frequently reported in studies of informal caregivers in home care settings, across urban and rural populations (Bouldin, Shaull, Andresen, Edwards, & McGuire, 2017; Brazil, Kaasalainen, Williams, & Dumont, 2014). A subset labeled “informational” needs was paramount to family caregivers of adults with acquired brain injury (Gan, Gargaro, Brandys, Gerber, & Boschen, 2010; Longacre, Galloway, Parvanta, & Fang, 2015). Other subsets, such as “inadequate resources” (Johnson et al., 2016), “meager amounts of support on financial assistance,” and “respite care” (Jorgensen, Parsons, Jacobs, & Arksey, 2010), have also been cited as reasons for dissatisfaction of informal caregivers. While these are pertinent for caregivers of patients with general or specific disease conditions, those caring for older adults—frequently having multiple medical comorbidities—are likely to be faced with additional challenges.
The salience of instrumental and emotional needs differs somewhat between rural and urban informal caregivers. In general, informal rural caregivers appear to have greater unmet needs/barriers for instrumental activities of daily living, for example, administering medications, grocery shopping, and preparing meals (Brazil et al., 2014), and because of lower income levels, they are also more likely to have financial barriers than their urban peers (Bouldin et al., 2017). In spite of this, rural caregivers perceive and report fewer caregiving challenges than their urban counterparts (Brazil et al., 2014). Urban caregivers, in contrast, are more likely to report caregiving challenges of the emotional type (Bouldin et al., 2017; Ehrlich, Bostrom, Mazaheri, Heikkila, & Emami, 2015). The reason suggested is that rural caregivers may be more emotionally self-reliant (Easter Seals and National Alliance for Caregiving, 2006) and thus better able to use “approach-based” coping strategies such as positive reframing, seeking social support, and problem-solving (O'Connell, Germaine, Burton, Stewart, & Morgan, 2013).
In urban areas, access to health care is not uniform, and islands of medically underserved communities (MUCs) are communities in which household income levels can range from that of the lower middle class to below the national poverty line (U.S. Department of Health and Human Services, 2015). The present study uses the term medically underserved community to describe a community that exists within a federally designated medically underserved area/population (MUA/P). Health Resources and Services Administration (HRSA) designates MUA/Ps based on a calculated index of four criteria: population-to-provider ratio, percent of the population below the federal poverty level, percent of the older adult (65+) population, and infant mortality rate (HRSA, 2019). While MUAs can cover almost the entirety of a large urban area, MUCs are generally encompassed within the MUAs. The geographical focus of the MUC under study—specifically the South Side of Chicago—is vital for differing reasons. On one hand, the South Side, a large underserved community comprising a nearly 100 square mile area with a population of about 1,000,000 people, is also a designated health provider shortage area with a lack of access to health care, health education, and community health resources (HRSA, n.d.; U.S. Census Bureau, 2013). On the other hand, it includes a vibrant, resilient, and culturally rich collection of neighborhoods comprising 20 zip codes. Such divergent characteristics of place, facilities, and population over a vast urban area uniquely qualify the South Side as an MUC worth investigating.
So far, the barriers/unmet needs of caregivers in such urban MUCs have not been studied in detail (Fernandes et al., 2010; Galiatsatos et al., 2017). The present study explores caregivers' experiences in this MUC on the South Side of Chicago and is part of a project on geriatric training for health-care personnel and for informal caregivers of older adults (SHARE Network, 2015).
The specific aims of this study are to explore (a) barriers/unmet needs of caregivers and (b) experiences of caregivers while providing care for home-dwelling elders. The intent is to focus on the perceived needs and experiences of caregivers living in the same MUC as care-recipients; therefore, we chose to ask caregivers to describe their interactions with care-recipients. The care-recipients, in this study, were all home-dwelling older adults (>65 years of age).
Methods
Because the literature on caregivers in MUCs is sparse, qualitative methods were used to explore the unmet needs/barriers that informal caregivers experienced. Qualitative methods enable the uncovering of not just “what” factors are salient but also “why” and “how” they are salient. Focus groups are a method for gathering information that is inductive and naturalistic, that is, data are collected through the dynamic interaction among participants in which participants are both influencing and are influenced by other participants in the group (Krueger & Casey, 2014). Furthermore, focus groups allow participants to answer specific questions, as well as to share their experiences in unsolicited areas surrounding the general topic. Therefore, focus groups were used to access informal caregivers' perceptions of unmet needs/barriers and experiences in providing care for older adults. This method could also help highlight caregivers' unique issues in MUCs and help generate hypotheses about ways to alleviate them.
Sample
Caregiver Demographics (n = 12).

Data not provided by two caregivers.
Recruitment
Recruitment strategies included (a) creating and posting culturally appropriate, low-literacy-appropriate informational flyers to advertise the study in designated neighborhoods so as to ensure that participants are from the South Side MUC and (b) Snowball sampling wherein one potential participant provides leads to recruiting others. Up to three telephone call attempts were made to recruit and remind participants about the day/time of the focus group sessions.
Methodology
Two focus groups were conducted (November 2016, March 2017) at two different community locations in the MUC site. Sessions were about 2 hours in duration. Internal review board approval from the Biological Sciences Division of The University of Chicago was obtained prior to recruitment. A research assistant obtained written consent and demographic forms from participants before start of the sessions.
A semistructured moderator guide (online Appendix A) was designed to ask about caregivers' perceptions of, and experiences with, unmet needs/barriers while caregiving. The guide begins with general questions (e.g., frequency of caregiving), followed by specific questions (e.g., unmet needs and barriers). Generally, lead questions were followed by open-ended probes. The goal was to engage each participant on items of interest to them, facilitating the emergence of individuals' perceptions and experiences. Focus groups were conducted at a quiet location convenient to participants. They were facilitated by a professional moderator experienced in conducting medical focus groups. Sessions were audio-recorded and professionally transcribed. Random sections of the written transcripts of both focus groups were cross-checked for accuracy against audio recordings for 10% of each of the two transcripts. As per HRSA guidelines, no financial remuneration or incentives were provided to participants other than light refreshments.
Coding and Analysis
Following Glaser and Strauss' (1967) principles of grounded theory, data collection and coding/analysis were conducted iteratively, that is, coding/analysis of the first focus group for emergent themes was initiated before the second focus group was conducted. This enabled us to assess whether we had reached “theme saturation” on completing the second focus group. “Theme saturation” was first defined as the point at which no additional data are found in a qualitative data set to develop properties of a category (Glaser & Strauss, 1967, p. 61). More recently, Guest, Namey, and McKenna (2017) defined a similar concept, termed “data saturation as the point in data collection and analysis when new information produces little or no change to the codebook” (p. 5). This concept of theme or data saturation has become the gold standard by which sample sizes for qualitative studies, including focus groups, are determined. In a recent methodological study, Guest et al. (2017) showed that as few as two focus groups (using a homogenous population and a semistructured guide) reached saturation, that is, linking the themes of two consecutive focus groups did not yield any additional categories or themes while capturing the most prevalent themes within the data set.
Our four-member team with expertise in medicine, social work, public policy, and psychology had ongoing discussions on reflexivity (Gilchrist & Williams, 1999) so as to bring to light awareness of any dormant biases that could potentially cloud the analysis. Team members (J. G., R. G-B.) played the role of a research assistant to the moderator in each of the focus group sessions. They were instrumental not only in obtaining consent forms but also in taking field notes and recording any nonverbal signals of participants, for example, nods, pauses, and so forth, to endorse a participant's viewpoint from other members of the focus group session, and these were taken into consideration in the analysis. Transcripts of focus groups were imported into Dedoose, web-based software Version 7.6, and, using a thematic analysis approach, two team members (R. G-B., J. G.) coded the transcripts, first independently and then collaboratively, to arrive at major themes. One set of themes derived from focus group questions (online Appendix A) were coded deductively, that is, codes from the guide were applied to the data collected, and the second set of themes that emerged unsolicited were coded inductively, that is, codes and themes were generated from the data collected (Blackstone, 2012). A codebook was developed using an iterative process in which modifications were made to the themes that arose from the first transcript (Morgan, 1996). On reviewing themes from the two focus groups, we found no new themes had emerged in the second focus group, indicating that we had reached theme saturation.
Following earlier research (Gorawara-Bhat, Wong, Dale, & Hogan, 2017), we used five major steps to analyze the data: (a) sorting and organizing the data into categories; (b) assigning these categories provisional descriptive labels; (c) performing iterative coding; (d) proposing/initializing major themes and subthemes; and (e) interpreting findings. Consensus discussion meetings occurred biweekly, as well as on an ad hoc basis among the four-member team. Discrepancies between analysts were discussed until agreement was reached on labeling of themes/subthemes and assigning illustrative quotes to them.
Results
Twelve informal caregivers participated in focus groups: Five were spousal caregivers, four adult children caring for a parent, and three informal caregivers who did not have a biological relationship with the care-recipient. As depicted in Table 1, two-thirds of caregivers (8) were themselves older adults ( > 65 years of age), with the remaining four equally split between age groups of 45 to 64 years and <44 years. Care-recipients were all older adults (>65 years of age) suffering from a variety of geriatric syndromes including functional and cognitive impairments. This was an exploratory field study and data collected included caregivers' age, gender, and relationship to care-recipient (presented in Table 1 and earlier text). As noted in the Introduction section, the focus was to understand caregivers' barriers, unmet needs, and experiences as they provided care for their loved ones. The data they provided about care-recipients' functional or cognitive impairments were secondary for this qualitative study and are used only to highlight how it supplemented caregivers' perspectives and experiences.
Major Themes
Two main themes emerged from the focus groups: (a) encountering unmet needs/barriers and (b) constructing meaning from caregiving challenges. Unmet needs/barriers have been the focus of many earlier studies both in urban and rural locations (Beach & Schulz, 2017; Bee et al., 2009; Jennings et al., 2015; Lafortune et al., 2015; Lund et al., 2015; Tallman et al., 2012; Tjia, Ellington, Clayton, Lemay, & Reblin, 2015). However, to the best of our knowledge, there is a dearth of studies investigating caregivers' needs/barriers in MUCs. Therefore, in the focus group sessions, we specifically asked caregivers about their needs/barriers while providing caregiving (see online Appendix A). On the other hand, constructing meaning from caregiving challenges has only infrequently been identified (Carbonneau, Caron, & Desrosiers, 2010; Cherry et al., 2017; Grover, Mehra, Malhotra, & Kate, 2017; Yu, Cheng, & Wang, 2018; Zarit, 2012) in the caregiving literature, and primarily so in the context of patients with dementia, hence was not specifically asked about in this study. Nonetheless, constructing and deriving meaning from the challenges of caregiving emerged as a salient dimension of caregiving—unsolicited and unanticipated. While Theme 1 has to do with external challenges that caregivers encountered, Theme 2 is about caregivers' internal processes of constructing meaning through caregiving challenges they encountered. We found both themes occurring together and evolving dynamically over care-recipients' progression of aging/disease as explicated later.
Theme 1: barriers and unmet needs of caregivers
Caregivers described two main types of unmet needs/barriers while providing care:
1A. Instrumental—refers to the utilitarian aspects of caregiving. For instance, Sarah 1 echoed the instrumental barriers: “there are a lot of household things that I had to move into … paperwork, cooking … ” (R1)
And, Jane shared the physical challenges she faced: “ … caregiving can really take it out of you; it became a hundred percent of my time literally for a couple of years … I would say the biggest challenge … I was exhausted … I'd get called away from work … ” (R2)
1B. Emotional—refers to the personal or interpersonal aspects of caregiving. For instance,
Patricia recounted the emotional impact: … the person who you are giving the care for has to have a venue to vent their anger … and you (caregiver) are the one who gets it … , … you lose some of your own personality in the process, you start changing … (R6)
The earlier quotes, extracted from our focus group sessions, highlight the physical/instrumental and emotional challenges informal caregivers face. The subtypes of barriers captured deductively from transcripts include the following:
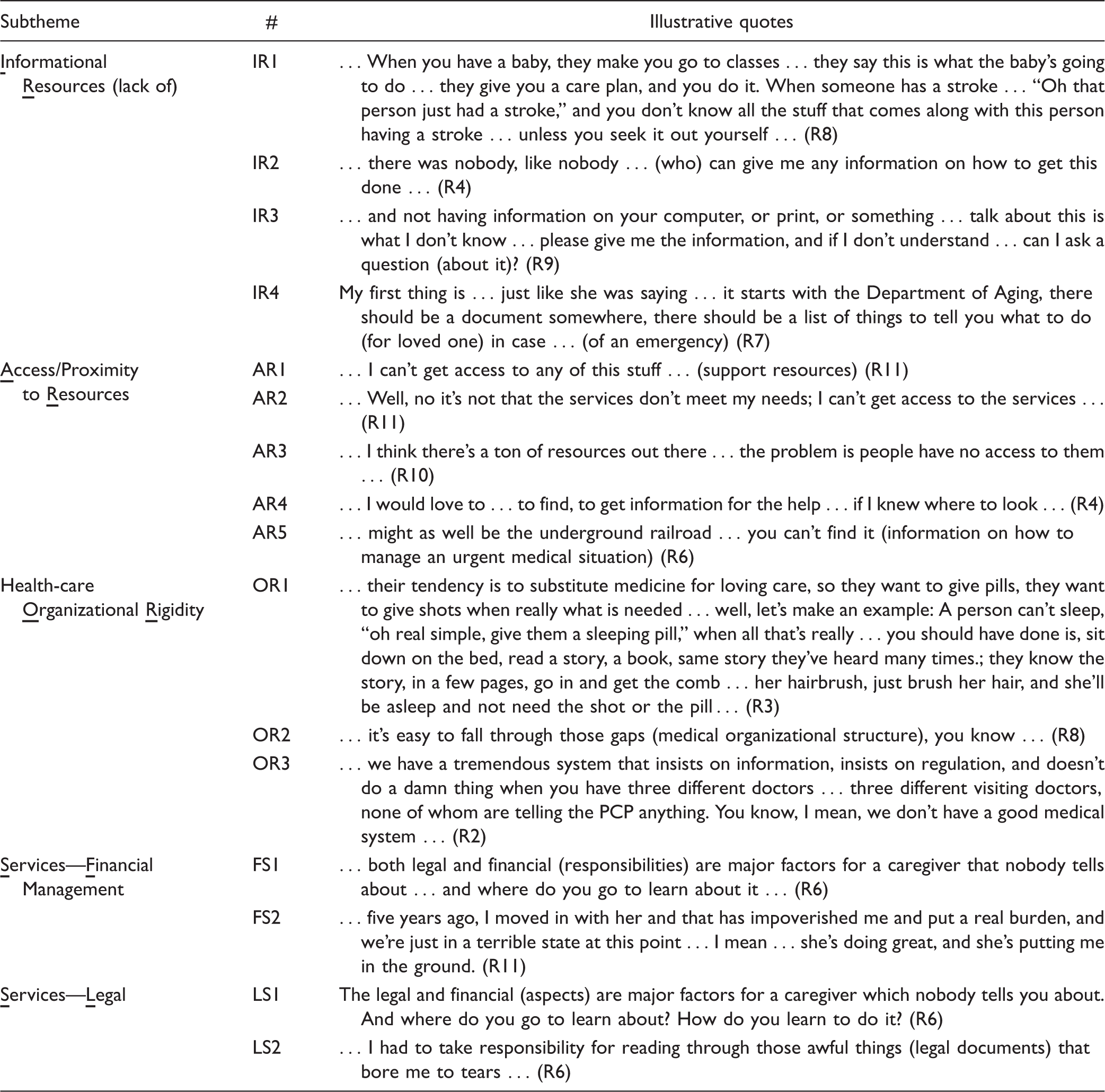
1A. Instrumental types of barriers/unmet needs
Health Information Resources—lack thereof (e.g., Internet/technology resources for managing type 2 diabetes) Access/Proximity to services—challenging (e.g., caregivers' inability to access services) Organizational Rigidity—bureaucratic barriers in health-care organizations Financial—Financial management (e.g., lack of funds for providing caregiving) and Legal Management (e.g., lawyers' consulting fees)
1B. Emotional types of barriers/unmet needs
Care-recipients' nonadherence—(e.g., with physician recommendations) Communication issues with recipients/extended family (e.g., challenging communication) Role reversal with recipient (e.g., caregiver role flipped with that of care-recipient) Caregiver support groups—lack thereof (e.g., support services)
Instrumental Barriers and Unmet Needs Perceived by Caregivers.
Emotional Barriers and Unmet Needs Perceived by Caregivers.

Theme 2: constructing meaning from caregiving challenges
While Theme 1 was deduced from responses to moderator's questions, Theme 2 was inductively extracted from transcripts and is described in detail later. Frequently in their verbalized narratives, caregivers reappraised barriers/unmet needs and constructed meaning from them by reframing them in three major ways:
Broadening the context in communication, Applying personal values or religious beliefs to caregiving tasks, and Conceptualizing role reversal to invoke empathy.
Broadening the context in communication
The ways in which communication unfolds is crucial to both caregiver and care-recipient. A few examples illustrate the case:
Patricia (caregiver, wife) and Don (care-recipient, husband with dementia) were “having regular fights about Don should not be driving anymore.” And, Don refused to comply with the physician's recommendations that he should give up driving, until one day we took a camera to the doctor's office and the doctor and my husband sat and talked, and the doctor explained to him why he could not drive (road safety for oneself and others), and … (subsequently) every time my husband would yell at me … it was on the camera, I showed it to him, and I'd say … “it's not me, I can't make those rules … it's your Dr.” … it took a huge bump out of our relationship … (R6)
Max, a 90-year-old caring for terminally ill wife Sharon, shared his experience: … (doctor provided) full information (disclosure about remaining time to live) … as much as you can get ahead of time … it is because of that … the six (final) months that we spent together were some of the most precious of our marriage, … we had conversations that we never had as married people … we could talk to each (emphasis added) other … I have those in me today … these are the gifts that I have due to her, that I'm extremely fortunate for, … that are helping me a lot … (R3).
Applying personal values/religious beliefs to caregiving tasks
Caregivers shared ways in which their own existential goals surfaced during their caregiving role. Max recounts the circumstances under which he found himself reconstructing his own future reality while managing caregiving tasks: … a year before all this (wife's terminal diagnosis) … (I realized) I've got to start learning what the hell “care” is … my first teacher was, of course, my wife who was beginning to … (deteriorate), and … I'm trying to realize … but (am) very slow … since we're going to lose her … who's going to take care of me? … (R3).
Sasha, a caregiver for a male friend, continued providing care despite the many barriers … from the goodness of my heart, I don't have to, I'm not mandated, I'm not required, I'm not getting paid, I don't have to be here in this capacity … but … this was something for me to do, in order to … you know, just be an assistant to someone … hopefully, when my time comes, there will be someone who will look after me … and that's primarily why I did it … (R10)
Conceptualizing role reversal to invoke empathy and enhance communication
Caregivers described constructing meaning and sustaining motivation in their caregiving role through another unique means: conceptualizing role reversal with, and invoking empathy for, their loved ones. Maria, after many frustrating attempts to seek “reciprocity” in her caregiving relationship with husband (care-recipient), became more empathic toward him, when her own broken leg injury led to a 2-month hospital rehabilitation and she understood his difficulties from an insider's perspective: … little by little he got more and more shut up in his world … he didn't relate to me anymore … like his wife. I was just somebody that he needed. And to adapt to that was one of the challenges … to realize it's not him, (rather) it's his mind deteriorating, and that he cannot do any more than he did … (R9). One thing that helped me greatly was when I broke my leg and was in a wheelchair myself, making experience on the inside … what it is for my husband for years now … not seeing this from the outside, but being able to switch roles … and to have the possibility to bring these images together and talk with somebody who can help develop empathy … (R9). … it was helpful for me to be able to recharge when I got C. Diff and I was hospitalized for five days …, I think that it's really helpful to do a role play, … I did find that that enabled me to … recognize how it felt to be on the inside … (R11).
Discussion and Conclusions
Discussion
With respect to the limited sample size, using common recruitment techniques of posting flyers and snowball sampling without supplementing them with any additional strategies may have contributed to the recruitment challenges we faced in this field study in an MUC. However, some methodology theorists (Guest et al., 2017) argue that theme saturation can be reached in as few as two focus groups using a homogenous data set and a semistructured guide. And, indeed we reached theme saturation using two focus groups in our sample of 12 caregivers from the MUC. Given that our MUC sample demographics show most caregivers themselves were older (8 of 12), retired (7 of 10), and female (10 of 12), some strategies to consider for optimizing response rates are suggested. First entails providing transportation to/from site for caregivers, that is, arranging for formal or informal rides. And, second making arrangements for respite care for their care-recipients can alleviate the financial burden of informal caregivers, who themselves are not paid for caregiving tasks they provide.
Now to the main findings, the structured questions asked of caregivers during the focus group sessions in our study highlight instrumental and emotional types of barriers/unmet needs similar to those identified by others (Bouldin et al., 2017; Brazil et al., 2014; Gan et al., 2010; Jorgensen et al., 2010; Longacre et al., 2015). Specifically, MUC caregivers perceived instrumental barriers commonly reported by informal caregivers in rural settings; however, they perceived emotional barriers similar to those reported by urban caregivers (Tables 2 and 3). This is not surprising because while MUC caregivers were located within an urban geographic location (identified by their zip code), they shared other characteristics, for example, lower socioeconomic status, similar to rural households. Furthermore, the ways in which they coped with challenges included developing strategies such as “constructing meaning” and approach-based strategies such as “positive reframing” similar to those used by rural caregivers (Easter Seals and National Alliance for Caregiving, 2006; Ehrlich et al., 2015; O'Connell et al., 2013). These differences/similarities between MUC caregivers' vis-à-vis urban and rural caregivers bear implications for policy makers.
In addition to responses to structured questions, focus group sessions brought forth unsolicited and unanticipated perspectives of caregivers, specifically about how they constructed meaning and coped with barriers. “Constructing meaning,” sometimes referred to as “meaning” or “meaning-making,” can be conceptualized as an interpretive psychological tool that is particularly important in the context of stress and coping (Park, 2010, 2013). “Meaning” has been broadly defined at two levels: “Global” meaning refers to individuals' general internal view of many events, while “situational” meaning refers to their internal view regarding a specific instance (Park & Folkman, 1997). In this study, “construction of meaning” at the “situational” level is most appropriate as caregivers cope with specific stresses of caregiving in MUCs. They are similar to concepts of “uplifts” (Kinney & Stephens, 1989) “inner growth,” (Pearlin, Mullan, Semple, & Skaff, 1990) and “meaning-focused coping strategies,” (Folkman, 1997, 2008) and those generally embedded in positive aspects of caregiving (Carbonneau et al., 2010; Cherry et al., 2017; Grover et al., 2017; Quinn & Toms, 2018; Totman, Pistrang, Smith, Hennessey, & Martin, 2015; Yu et al., 2018; Zarit, 2012). MUC caregivers in this study constructed meaning mainly through making positive reappraisals of caregiving challenges as explained later.
Three ways in which caregivers reappraised barriers and constructed meaning from them are detailed in the Theme 2: Constructing Meaning From Caregiving Challenges section. We now suggest the application of Fredrickson's (2001) cognitive psychological theory of emotions—“ broaden-and-build theory” to our MUC data to explain the gestalt of informal caregivers' coping strategies. Fredrickson's theory, originally developed to explain the role of positive emotions in general (Fredrickson, 2001; Fredrickson & Joiner, 2002), is empirically supported by a series of experiments (Fredrickson, 2001; Fredrickson & Branigan, 2005). The major tenets of the theory are (a) positive emotions (past or imagined future) “broaden” and shape individuals' thinking and actions; (b) broadening perspectives and actions, prime individuals' to “build” lasting personal resources (physical, intellectual, psychological, and social); and (c) individuals personal resources subsequently evolve as psychological adaptations for coping with stressful situations. These three steps provide guidance on how to support individuals to build an emotional environment to achieve the goal of enriching them. In the following paragraphs, an attempt is made to explain the ways in which strategies adapted by MUC caregivers, to cope with chronic physical and emotional stresses, are consistent with the earlier three tenets.
In his caregiving role, Max (see Broadening the Context in Communication section) draws upon his past positive emotional bond with Sharon; invokes this resource to broaden the context of his communication over a lifetime; reappraises it, from “regular” to “precious” in the past 6 months; cherishes what remains with positive affect; and adaptively copes with the present challenges of caring for Sharon. It is apparent that Max's thinking and actions, grounded in “positive reappraisal” of communication, follow the “broaden-and-build” theory.
In the example from the Applying Personal Values/Religious Beliefs to Caregiving Tasks section, caregiver Sasha's religious beliefs and moral responsibilities acted as a personal resource in challenging times; they helped her make the decision to continue providing care for her friend based in the belief of “you reap what you sow” and acted as a coping mechanism for the challenges she faced. Here again, we see how Sasha's thinking and decision follow tenets of the “broaden-and-build” theory. It is worth noting that spirituality and religious beliefs are known to be one of the potentially most valuable resources for reappraising negative aspects of caregiving and a coping mechanism for challenges encountered (Heo, 2014; Hodge & Sun, 2012; Quinn, Clare, & Woods, 2012; Roff et al., 2004; Shim, Barroso, & Davis, 2012).
Consider the example of Maria (see Conceptualizing Role Reversal to Invoke Empathy and Enhance Communication section) in which she recognizes that her spousal relationship had become “asymmetrical” over the years. Her strong bond with her husband (care-recipient) of many years (positive affect) prompted her to reappraise her burden by reversing her role with her husband “from the inside” (when she needed to be hospitalized for a broken leg) and renew her intrinsic motivation and empathy to care for his progressively deteriorating condition. Through invoking role-play, Maria understood her husband's deteriorating condition, accepted their present asymmetrical situation, and decided to continue providing care, thus finding meaning in returning love received from him in the past. It is known that renewing intrinsic motivation for caregiving (through role-play as in earlier case) promotes meaningful experiences for caregivers (Quinn et al., 2012).
Caregiver–care-recipient dyad and its evolution
In constructing meaning from, and coping with barriers, caregivers also reintegrated care-recipients into an evolving dyadic relationship unit, that is, any change to one component of the dyad seemed to have an influence on the second. The cross-sectional nature of the present study did not allow for exploring the evolving nature of the dyad over time; however, caregivers shared ways in which their dyadic relationships evolved over the progression of care-recipients' disease stages. Examples from the three types of dyads in our data—(a) caregiver–spouse; (b) caregiver–parent, and (C) caregiver–friend—highlighted in online Appendix B—illustrate how the caregiver–care-recipient dyad acts as a unit over the caregiving phase with the caregiver–spouse dyad showing the greatest strength, followed by caregiver–parent and caregiver–friend indicating the least, as evidenced in the degree of dedication/commitment expressed in their verbalized narratives.
The caregiver–care-recipient dyad acted as the context in which challenging and enriching aspects in the caregiving experience occurred in tandem. While the salience of mutuality in caregiver–care-recipient dyad has been studied earlier (Andren & Elmstahl, 2005; Butcher & Buckwalter, 2002; Narayan, Lewis, Tornatore, Hepburn, & Corcoran-Perry, 2001), this study is one of the few (Yu et al., 2018) to show that the dyad evolves as central in the caregiving experience. Thus, from the policy-making perspective, the dyad is best understood as the pivotal construct that enables a comprehensive understanding of the gestalt of caregiving. To enhance the caregiving experience therefore, it is imperative to alleviate the barriers/unmet needs and to simultaneously amplify the meaning-making facets of caregiving so as to improve caregivers' overall adaptation/coping process.
Strengths and limitations
This study used focus groups to solicit informal caregivers' experiences of, and challenges encountered in, caring for their home-dwelling older adults. As such, it has limitations of responses being clouded by social desirability—a bias attributable to any qualitative data collection. Second, the study sample is small; however, we reached theme saturation, and hence assume that emergent themes are valid and reliable. Nonetheless, the small sample presents limitations. For instance, the small, mixed caregiver cohort and predominantly female sample precluded us from comparing the role of gender and familial relationship for the differential ways that caregivers may have constructed meaning from specific situations. Furthermore, sample size deterred understanding differences that physically or cognitively impaired care-recipients may have had on caregivers' strategies for coping with challenges. Third, the study was conducted in one MUC in urban Midwest United States, and the findings may not be generalizable to other regions. Despite these limitations, the findings of this study corroborate the caregiving literature (Yu et al., 2018) and go beyond these to emphasize the need to transition from simply alleviating caregivers' instrumental, external challenges to implementing training/services for making an organic, internal impact on caregivers through enriching emotional aspects in their caregiving experiences.
Conclusions and Implications
1. Two themes emerged from MUC caregivers' reports:
a) Caregivers' barriers/unmet needs in caregiving included—(a) instrumental challenges encompassing a lack of informational resources on medical aspects and (b) emotional challenges comprising a lack of support groups, and b) Constructing meaning—an unsolicited and unanticipated theme—highlighted how caregivers “constructed meaning” from the previously mentioned barriers through reappraisals, creating enriching experiences, and coping with challenges. 2. Caregivers reappraised barriers and constructed meaning from these in three major ways:
a) Broadening the context of communication; b) Applying personal values or religious beliefs to caregiving tasks; and c) Conceptualizing role reversal to invoke empathy. 3. “Broaden-and-build” theory (Fredrickson, 2001) can be invoked to explain the gestalt of caregivers' strategies for enriching their experiences and coping with challenges. 4. Challenging and enriching aspects were coexisting and rooted in the caregiver–care-recipient dyad, and implications for one component of the dyad seemed to have consequences for the other.
Given that caregivers in MUCs experience both negative and positive aspects of caregiving within the caregiver–care-recipient dyad, it is imperative that policy is shaped to address both these aspects. Thus, the study implications include the following:
Increasing informational resources and targeting programs commensurate with needs of both caregivers and care-recipients in MUCs through use of technology and relevant outreach programs. Building caregivers' and health-care workers' competencies in MUCs for managing care-recipients medical conditions (e.g., through geriatrics workforce enhancement programs). Providing training/interventions to support the caregiver–care-recipient dyad, such as programs for improving caregiver communication skills vis-à-vis care-recipients and for making positive reappraisals of caregiving challenges to cope through difficult phases of caregiving.
Supplemental Material
Supplemental Material1 - Supplemental material for Informal Caregiving in a Medically Underserved Community: Challenges, Construction of Meaning, and the Caregiver–Recipient Dyad
Supplemental material, Supplemental Material1 for Informal Caregiving in a Medically Underserved Community: Challenges, Construction of Meaning, and the Caregiver–Recipient Dyad by Rita Gorawara-Bhat PhD Jeffrey Graupner MPH Jason Molony AM Katherine Thompson MD in SAGE Open Nursing
Supplemental Material
Supplemental Material2 - Supplemental material for Informal Caregiving in a Medically Underserved Community: Challenges, Construction of Meaning, and the Caregiver–Recipient Dyad
Supplemental material, Supplemental Material2 for Informal Caregiving in a Medically Underserved Community: Challenges, Construction of Meaning, and the Caregiver–Recipient Dyad by Rita Gorawara-Bhat PhD Jeffrey Graupner MPH Jason Molony AM Katherine Thompson MD in SAGE Open Nursing
Footnotes
Acknowledgments
The authors gratefully acknowledge the time and effort of caregivers for participating in the present research and sharing candid views on the barriers/unmet needs they face every day and their experiences while providing care for their loved ones in an MUC.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the HRSA of the U.S. Department of Health and Human Services under grant # U1QHP28728 (K. T.) under their “Geriatric Workforce Enhancement Program.” The funding source had no direct input into any of the research processes, and investigators retained full independence in this research.
Supplemental Material
Supplemental material for this article is available online.
Note
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.