
Abstract
Background
Mindfulness-based intervention (MBI) has not been evaluated for its feasibility and effectiveness in reducing stress and anxiety among family caregivers of patients on peritoneal dialysis (PD).
Objectives
(1) To evaluate the feasibility to include MBI during PD training for family caregivers. (2) To determine the effect of MBI on the caregivers’ levels of stress (perceived stress scale, PSS), anxiety state-trait anxiety inventory, STAI), QOL (short-form 36) and reactions to caregiving (caregiver reaction assessment, CRA). (3) To determine differences in the health-related QOL (Kidney Disease Quality of Life Instrument-Short Form
Methods
This feasibility study recruited family caregivers to receive either mindfulness training (MT) or treatment-as-usual (TAU) group. Both groups received 4.5-days of structured PD training, but only caregivers in the MT group received 4 days of MT sessions, audio-guided mindfulness practice at home and weekly telephone follow-up.
Results
Forty-four family caregivers participated in this study. Including MBI as part of the PD training was feasible. There was a trend towards lower scores for PSS and T-STAI in the MT group compared to the TAU group. The baseline score of both PSS and T-STAI were positively correlated with post-intervention outcome scores.
Conclusions
Mindfulness-based intervention has the potential to improve psychological symptoms among caregivers of patients with PD.
Keywords
Introduction
Worldwide, the number of patients dependent on dialysis is growing rapidly, driven by ageing populations and increased chronic diseases such as diabetes mellitus and hypertension. 1 The global prevalence of maintenance dialysis has increased 1.7 times from 165 patients per-million-population (pmp) in 1990 to 284 pmp in 2010. 2 In Singapore, the prevalence of patients requiring dialysis has increased from 689.3 pmp in 1999 to 1046.5 pmp in 2016. 3
Peritoneal dialysis (PD) is a home-based therapy that requires significant self-care at home and a dedicated caregiver, especially for older adults. 4 As a result, PD caregivers experienced both physical strains and high emotional stress due to their caregiving responsibilities.5-7 A recent study found that caregivers of PD patients had significantly higher rates of anxiety, depression and poor sleep quality than caregivers of patients who had a kidney transplant. 8 In addition, the caregiver burden was reported to be the highest for the continuous ambulatory peritoneal dialysis group. Consequently, caregivers of PD patients experienced a significantly reduced quality of life.8,9 A longitudinal study on PD caregivers in Singapore concluded a strong need for mental health support among PD caregivers. 7
Therefore, given the significant burden and stress experienced by PD caregivers, it is essential to empower PD caregivers with psychosocial interventions such as mindfulness-based interventions (MBI) for managing their caregiving challenges. MBI is a type of self-regulatory approach to reduce stress and manage emotions. It has been shown, albeit inconsistently, to alleviate physical and psychological symptoms associated with stress, improve the ability to regulate emotions and increase capacity for empathy and compassion.10,11
Background
Current support interventions for family caregivers for people with chronic kidney disease are multidimensional and often include psychosocial, educational and peer support components.12–14 MBIs targeting caregivers were introduced and evaluated more recently; however, most studies only focused on caregivers of patients with cancer or dementia. Meditation and imagery therapy were reported to reduce depression, anxiety and insomnia among family caregivers of dementia patients, but their quality of life (QOL) did not change after 3 months. 15 A randomised controlled trial of mindfulness-based stress reduction training on family caregivers of dementia patients found that perceived stress and depression were significantly reduced at 3 months but not at 6 months. 16 Overall, mindfulness training seemed to reduce dementia caregivers’ stress effectively, anxiety and depression but not QOL.15–18 Notably, the types of mindfulness-based interventions (MBIs), study designs and follow-up period varied between studies; thus, its effectiveness remains unclear. Only one study on family caregivers for persons with chronic conditions found that mindfulness training was more effective than self-help education in reducing depression, anxiety and perceived stress at 3 months of follow-up. 19 However, it was not specified which chronic diseases were targeted or whether the sample was homogenous.
Peritoneal dialysis is a lifelong therapy that can be physically and emotionally demanding for patients and their family caregivers managing the PD. Hence, it is crucial to empower caregivers with self-management skills to manage their daily stress and other caregiving challenges. Furthermore, interventions that can improve the well-being of PD caregivers are also likely to enhance compliance and effectiveness of PD therapy. MBI has not been evaluated on the family caregivers of patients with PD.
Study aim
This study aimed to examine the feasibility and effectiveness of MBI on family caregivers of patients receiving PD therapy.
Objectives
1. To evaluate the feasibility to include MBI during PD training for family caregivers. 2. To determine the effect of MBI on the caregivers’ levels of stress (perceived stress scale, PSS), anxiety state-trait anxiety inventory, STAI), QOL (short-form 36 including physical component summary, SF-36 PCS and mental component summary, SF-36 MCS) and reactions to caregiving (caregiver reaction assessment, CRA). 3. To determine differences in the overall health-related QOL (Kidney Disease Quality of Life Instrument-Short Form, KDQOL PCS and SF-36 MCS) of care recipients with caregivers receiving MBI at 1 month, 3 months and 6 months when compared to those with caregivers receiving routine training. 4. To gather caregiver’s feedback on the MBI.
Method
This feasibility study was conducted at an acute care teaching hospital in Singapore (August 2016 to January 2019). Family caregivers who were new to PD therapy and scheduled to attend PD training were invited to participate in this study. Caregivers were eligible if they were the family caregivers (unpaid) assisting patients with their daily PD therapy (automatic or continuous PD) and understood English. Family caregivers had to be at least 21 years old and above.
Eligible family caregivers were randomly assigned to receive either the mindfulness training (MT) or treatment-as-usual (TAU) using a random number generator. The randomisation process was done by a research coordinator (RC) who was not involved in the study, and the allocation list was sealed in an opaque envelope. The randomisation was based on the planned sample size hence the reason behind the unequal distribution of the sample size when we had to stop the study due to limited funding.
Sample size
Utilising data from similar studies examining the effects of a mindfulness training program on caregivers and their perceived stress scale (PSS) score, to achieve an estimated minimum clinically relevant difference of four points (SD=7.5) on the PSS score, a two-sided test with α of 0.5 and power of 80%, 57 caregivers per group was required. To account for 20% dropout, which had been commonly reported in similar mindfulness trials, a total of 138 caregivers were to be recruited, with 63 per group. However, recruitment was unexpectedly low due to eligibility issues, and there was a high dropout rate (see CONSORT Flow Chart). Thus, the planned sample size was not met.
Treatment-as-usual
The family caregivers in the Treatment-as-usual (TAU) group served as controls; therefore, they received only the standard 4.5 days of structured PD training. The purpose of the PD training was to equip the family caregivers with the skills and knowledge to care for their loved ones. The content of the PD training includes managing the Tenckhoff catheter, performing dialysis bag exchanges and exit-site dressing, troubleshooting the APD machine, monitoring and documentation of the dialysis intake/output chart.
Mindfulness training
The Mindfulness training (MT) was developed and delivered by a clinical psychologist (KD) trained in mindfulness. Details of the teaching content are outlined in supplemental material. The family caregivers in the MT group also received the structured routine PD training. At each session, the caregivers spent an hour of learning and practising a mindfulness technique. At the end of each session, caregivers were instructed to practice the mindfulness exercises in the evening at home and to provide feedback on their practice the next day. They were guided on the practice daily during the session to ensure they could fully immerse themselves in the practice. Caregivers were recommended to practice breathing exercises in the morning and the body scan in the evening. During the PD therapy, caregivers were taught the techniques to incorporate mindfulness into their senses as they performed the various steps to set up and remove the PD apparatus. Finally, to foster compassion for themselves and their loved ones, they were taught a loving-kindness and gratitude exercise.
To facilitate caregiver’s understanding and practice of MT, they were provided with reading and audio materials to guide practice at home. A logbook was given to record their practice. They were recommended to practice the body scan daily and mindfulness breathing at the start of every PD therapy. To encourage participation, the RC contacted the caregivers via telephone every week for 4 weeks and monthly for 6 months to check in on their daily practice, that is, how long they practice, the issues or problems experience during the practice and their feedback on the interventions.
Outcome measures
The outcome measures were taken at baseline, 1 month, 3 months and 6 months post-randomisation. All assessments were carried out at the outpatient clinic by an RC.
Perceived stress scale (PSS) is a self-reported questionnaire that measures how the individuals appraise the situations in their lives as stressful (i.e. unpredictable, uncontrollable and overloaded) during the previous month. 20 PSS contains 14 items, 7 of them positive and 7 negative, and responses range from 0–4 (0 = never; 1 = almost never; 2 = sometimes; 3 = fairly often; 4 = very often). The higher the total score, the higher the perceived stress. Reported Cronbach’s alpha ranged from 0.75–0.89, indicating good reliability. 21
The state-trait anxiety inventory (STAI) is the leading measure of personal anxiety worldwide. 22 STAI form Y was used. It consists of 40 items that measure the state and trait anxiety. State anxiety assesses how the individual completing the survey feels at the present moment, while trait anxiety is a measure of general stress. Total scores range from 20 to 80, with higher scores indicating increased levels of anxiety. Measures of internal consistency for the STAI average >0.89, and test-retest reliability is high.23,24
The 36-items of short-form 36 (SF-36) was a generic health-related quality of life (HRQoL) tool used to assess the caregiver’s QOL. However, we used the SF-36 v2 Singapore version as the scoring of the items were weighted to be more representative of Singaporean assessment of their QOL. 25 The SF-36 v2 comprised of eight health domains, and higher scores reflected better-perceived health.
The 24-items of the caregiver reaction assessment (CRA) measured the effect of caregiving on the caregiver’s schedule, finances, family support, health and esteem, providing scores on each of these five domains/subscales. 26 The CRA tool had also been validated in Singapore. 27
For the care recipients, the kidney disease quality of life instrument-short form (KDQOL-SF) was used to assess the functioning and well-being of people with kidney disease and on dialysis. 28 It consists of 36 items that specifically measure patients’ QOL on dialysis. 29 KDQOL-36 subscale scores ranged from 0 to 100, and lower scores indicated the worse self-reported QoL. It was a reliable and valid tool to assess the HRQOL of patients with ESKD in Singapore. 30 The KDQOL-SF (Version. 1.3) was measured at 3-months and 6-months post-randomisation.
Statistical analyses
The demographic and baseline values of the caregivers in both groups.

MT: mindfulness training; TAU: treatment-as-usual; PSS: perceived stress scale; S-STAI: State-Trait Anxiety Inventory – State Anxiety; T-STAI: State-Trait Anxiety Inventory – Trait Anxiety; CRA: Caregiver Reaction Assessment; SF36 PCS: Short-form 36 Physical Component Summary; SF36 MCS: Short-form 36 Mental Component Summary.
The demographic and baseline values of the care-recipients in both groups.
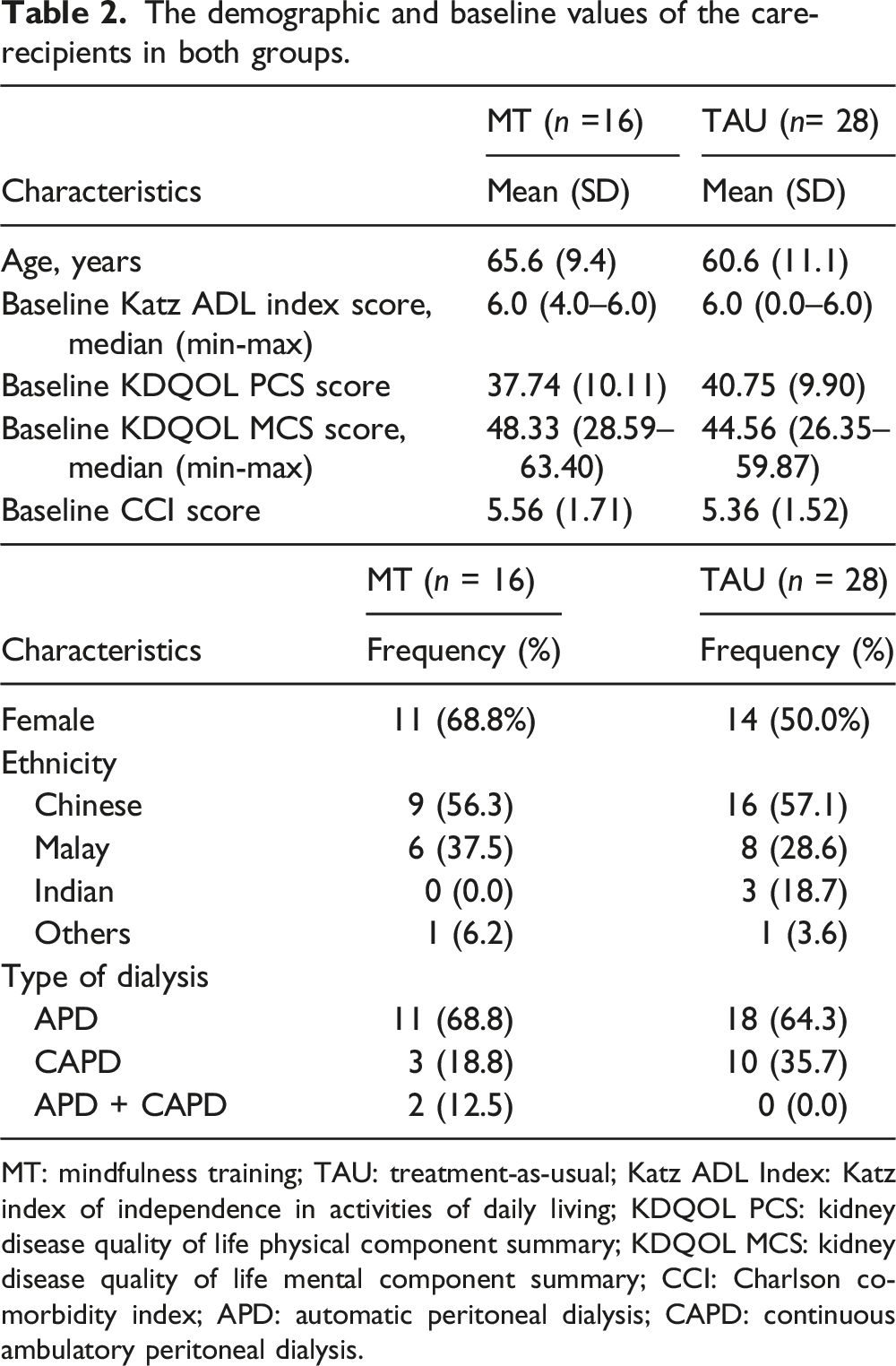
MT: mindfulness training; TAU: treatment-as-usual; Katz ADL Index: Katz index of independence in activities of daily living; KDQOL PCS: kidney disease quality of life physical component summary; KDQOL MCS: kidney disease quality of life mental component summary; CCI: Charlson comorbidity index; APD: automatic peritoneal dialysis; CAPD: continuous ambulatory peritoneal dialysis.
A linear mixed model (LMM) was used for repeated measures over time with Bonferroni adjustment for multiple comparisons to analyse the impact of the mindfulness intervention on the score at the three-time points (1-month, 3-months and 6-months). Except for the caregiver’s SF-36 PCS, SF-36 MCS and CRA score were obtained only at 3-months and 6-months. In this model, fixed covariates included time, group and the respective baseline score. The interaction between time and group was removed when no significance was detected.
We used LMM as this procedure avoided the loss of subjects through listwise deletion due to missing data in follow-ups. In our LMM, as the variance-covariance structure for the repeated measurements, we selected ‘Compound Symmetry’ as this was robust to the misspecification of the model in terms of correlation of repeated measurements.
Results
Figure 1 showed the CONSORT flow diagram. A total of 44 caregivers were randomly assigned to the MT group (n = 16) and the TAU group (n = 28). Of the 44 caregivers randomized; 34 (77.3%) were followed up at 4-weeks, 27 (61.4%) at 3-months, and 19 (43.2%) at 6-months. At the end of 6-months, attrition rate in the MT group was 75.0%, in the TAU group 46.4% (χ2 = 3.39, d.f. = 1, p = .066). No statistically significant difference was detected in age, gender, employment status and educational level between those who completed and those who dropped out in either group. The mean age of the caregivers was 47 years, and there were more female caregivers (70.5%; n = 31) than male (29.5%; n = 13). Most caregivers were Chinese (56.8%; n = 25), followed by Malay (29.5%; n = 13), Indian (9.1%; n = 4) and others (4.5%; n = 2). The relationship between the care recipient and caregiver was primarily either spousal (45.5%; n = 20) or parent-child (47.7%; n = 21). CONSORT flow diagram.
Effects of mindfulness-based intervention on the caregiver
The effect of intervention on primary outcomes of caregiver’s PSS, STAI, SF-36 (PCS and MCS) and CRA over time.
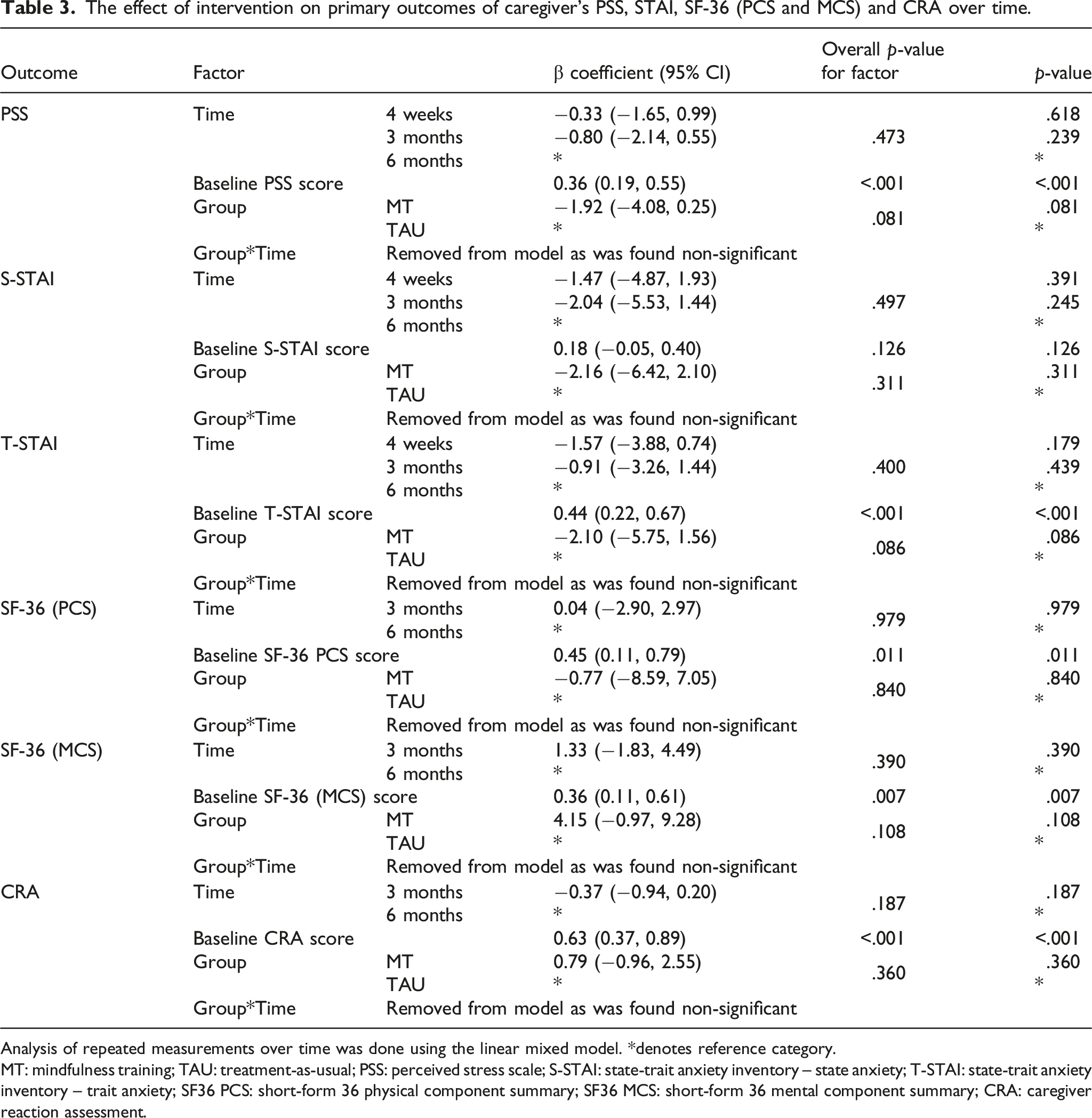
Analysis of repeated measurements over time was done using the linear mixed model. *denotes reference category.
MT: mindfulness training; TAU: treatment-as-usual; PSS: perceived stress scale; S-STAI: state-trait anxiety inventory – state anxiety; T-STAI: state-trait anxiety inventory – trait anxiety; SF36 PCS: short-form 36 physical component summary; SF36 MCS: short-form 36 mental component summary; CRA: caregiver reaction assessment.
Effect of mindfulness-based intervention on care recipients
The changes of care recipients’ KDQOL PCS and MCS score over time at 4 weeks, 3 months and 6 months.

*Denotes reference category.
MT: mindfulness training; TAU: treatment-as-usual; KDQOL PCS: kidney disease quality of life physical component summary; KDQOL MCS: kidney disease quality of life mental component summary.
As for SF-36 PCS, SF-36 MCS and CRA were evaluated only at the two follow-up time points (3-months and 6-months), there was also no significant difference over time in both groups combined (SF-36 PCS, p = .979; SF-36 MCS, p = .390; CRA, p = .187). Additionally, care recipients in the MT group did not demonstrate a significant difference from the TAU group on any of the outcomes (SF-36 PCS, p = .840; SF-36 MCS, p = .108; CRA, p = .360).
Caregiver’s feedback on the mindfulness-based intervention
Four out of the 16 caregivers in the MT group dropped out even before the first follow-up. Therefore, only 12 caregivers reported their home practice time at 4 weeks. The mean practice time was 33 ± 24 minutes per week, ranging between 2.5 to 95 minutes per week. There was no significant correlation between cumulative minutes of practice and PSS at 1-month post-randomisation (r = 0.004; p ≥ .05). There was no statistically significant difference between those who had completed the program versus the dropouts.
The most common reasons for dropping out was because the caregivers were uncontactable, that is, after five phone calls. Followed by caregivers who no longer needed to perform the dialysis as patients could perform the PD independently or patients had switched to haemodialysis, therefore do not require the caregiver’s help. Three patients demised; hence their caregivers were dropped out from the study.
Among the feedback of the caregivers who completed the mindfulness program, they felt that the intervention made them feel relaxed, focused and calmer when performing the dialysis. ‘At first, I thought I wouldn’t have time to practice cos I will be busy helping my mum with the dialysis, but after trying it and daily practice, I was able to feel more relaxed and positive. I usually do the breathing practice every morning for about 5 minutes’ [MT02, Son]. Another caregiver reported, ‘I felt the sessions were beneficial…It helped my husband, and I feel a bit calmer when doing the dialysis at home’ [MT05, Wife]. ‘The breathing exercise helped me feel energised and focused every morning' [MT09, Wife]. ‘The mindfulness practices have helped me a lot in managing my stress level as I got to work and also helped my mother with her dialysis’ [MT07, daughter]. We also gathered a patient’s feedback, who was also practicing with her daughter. She said, ‘I felt happy and loved every time *the main caregiver* did the loving and kindness practice cos it helped her be aware of the importance of looking at her well-being too’
Discussion
This is the first study to examine the feasibility and effectiveness of MBI on family caregivers for patients receiving PD therapy. Although it was feasible to incorporate MBIs as part of the structured PD training, the MBIs did not reduce the family caregiver’s perceived stress and anxiety. However, we found a trend suggesting lower scores of PSS and T-STAI among caregivers in the MT group compared to the TAU group, although it was not statistically significant. Notably, the baseline score of PSS and T-STAI positively predicted its post-intervention outcome scores; the higher the baseline scores of PSS and T-STAI, the higher the scores of PSS and T-STAI at the end of the program despite receiving MBI. This is a useful insight as it highlights the importance of early assessment and management of caregiver stress even before initiating a lifelong therapy such as peritoneal dialysis. It also highlighted the need to adopt additional strategies to help caregiver better cope and adapt to the challenges of caregiving.
A possible reason for the high PSS baseline score of the caregivers could arise from the intensive caregiving needs, such as transferring, mobility and toileting, as evident by the high score on the activities of daily living (ADL) even before starting the PD therapy. Studies have shown that a higher stress appraisal and low ratings of subjective well-being among caregivers are consistently associated with the duration and intensity of care provided. 31 Anecdotally, we observed that most low-income families would delay starting PD therapy until they are at a critical stage as healthcare in Singapore is primarily self-funded. Henceforth, patients are more dependent on caregivers at that stage, and the financial burden will add to caregiving stress.
Interestingly, high ADL scores of the care recipients did not seem to affect the caregivers’ PSS, and anxiety was an unexpected finding as it goes against conventional wisdom, that is, the more ill the patient was, the more care was needed; hence, it was more stressful for the caregivers. Perhaps, this unusual finding could be explained by the caregiver’s social support, family functioning and stress management; however, these were not explored in this study. Future research should consider examining the caregiver’s informal support, that is, the social relationships of the caregiver with extended family, friends and neighbours; family function, that is, how the family worked as a unit; and stress management, that is, how the caregiver managed stress when dealing with problematic situations, which would provide a more holistic view of the caregiving situation and accounting the potential confounders that would affect the study outcomes.
Mindfulness-based intervention has been demonstrated to promote better stress management; however, most studies have found that it requires several weeks of continuous practice before experiences any trait-like change in their well-being. 32 Caregivers were recommended to practice body scan and focused breathing daily for up to 6 months in this study; however, this was subjected to their compliance in practice which was self-reported and may not be rigorous. Therefore, future studies should consider leveraging technology that provides an objective measurement system in examining the effect of adherence on home practice. 33
Carmody and Baer found that the amount of time participants engaged in a mindfulness program was negatively associated with their reported symptoms of stress and well-being, 34 which might explain the reduction in symptoms of perceived stress and improved psychological well-being. However, in this study, we did not find any correlation between the cumulative practice time and reduction of stress.
The high dropout rate in this study demonstrates the difficulties with engagement and retention in a mindfulness program. Low compliance and high dropout rates for mindfulness program are, therefore, typical. For example, Kabat-Zinn and Chapman-Waldrop reviewed compliance in a standard 8-weeks mindfulness programme; found 15% dropping out after the beginning of the programme, usually within the first few weeks 35 ; a similar pattern is observed in this study. The caregiver’s feedback on their low compliance is because they often forgot to practice as they were busy. This demonstrates the need to use a reminder system to increase participation at home. Therefore, future study should incorporate a reminder system and a more intensive follow-up with the caregivers to avoid attrition.
One of the reasons for our low recruitment rate was because most of the caregivers were foreign domestic helpers (FDHs), thus not eligible to participate in this study. Generally, FDHs are hired to provide physical care to our Singaporean patients at home; however, family caregivers are still responsible for financial, emotional support and medical decision-making. 36 In this study, the family caregiver who attended and participated in the program was not always the primary caregiver providing the PD but were involved in the PD training because they were the primary decision-maker in the family. Hence, this study shows that even without the physical demands of caregiving, family caregivers do experience stress and anxiety. Therefore, MBI could be a valuable skill for family caregivers.
Limitations
In order to reinforce and encourage the mindfulness practice, we provided all caregivers with a CD to guide home practice in addition to the weekly telephone follow-up to check on their practice. However, we could not verify the extent of actual mindfulness practice as it was self-reported. Also, we could not assess the quality of mindfulness practice, which may influence the study outcomes. Future studies should consider a more objective measurement system in measuring compliance with mindfulness practice.
This study was underpowered to detect any significant effect of mindfulness practice due to the small sample size and high dropout rate. Future research would need to consider the challenges in recruiting and retaining family caregiver of PD patients in a mindfulness study trial. The caregivers in this study understood English; hence future researchers may consider designing and implementing the mindfulness program in different languages.
Conclusion
It is feasible to include MBI as part of PD training; however, it is challenging for family caregivers to continue the mindfulness practice beyond 4 weeks. The MBI as taught did not significantly affect caregiver’s perceived stress and anxiety; however, the null findings could be due to the small sample size. A larger study with simpler and more focused mindfulness techniques that include the care recipient may be necessary in the future when designing a pragmatic MBI trial.
Supplemental Material
sj-pdf-1-psh-10.1177_20101058211054913 – Supplemental Material for Evaluating the feasibility and effectiveness of a mindfulness-based intervention on stress and anxiety of family caregivers managing peritoneal dialysis
Supplemental Material, sj-pdf-1-psh-10.1177_20101058211054913 for Evaluating the feasibility and effectiveness of a mindfulness-based intervention on stress and anxiety of family caregivers managing peritoneal dialysis by Fazila Aloweni, Kinjal Doshi, Nurliyana Agus, Stephanie Fook-Chong, Sin Yan Wu, Lau Peng Kong, Marjorie Foo, Elena M Ayob and Truls Ostby in Proceedings of Singapore Healthcare
Footnotes
Acknowledgements
We would like to acknowledge all staffs from Peritoneal Dialysis Centre in Singapore General Hospital for their support in recruiting the participants. We like to thank Ms Ang Shin Yuh for her advice and support during the conduct of this study. Also, Dr Fan Qianqian, Dr Lim Siew Hoon and Ms Chew Suet Mei for their statistical support.
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest concerning the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received funding from SingHealth Research Foundation Grant (SHF/HSR094/2015). The funding source had no role in the study’s design, conduct, or reporting.
Authors’ contributions
FA conceived the study, and subsequently, KD, TO, WSY, MF and EMA involved in the protocol planning and development. NL and FA were involved in the application of ethics. WSY, NL, LPK in patient recruitment and data collection. KD performed the intervention. Data analysis and interpretation were done by FA, KD, MF, TO and SFC. FA, KD, TO, and SFC wrote and revised the manuscript. All authors reviewed and edited the manuscript and approved the final version of this manuscript.
Availability of data and materials
The datasets generated and/or analysed during the current study are available from the corresponding author.
Ethical approval
This study was approved by the Institutional Review Board (ref no: 2016/2395) and complied with the ethical guidelines of the Declaration of Helsinki. Informed consent was obtained from all caregivers.
Informed consent
Informed consent was obtained from all the family caregivers who were assisting patients with their daily PD therapy (automatic or continuous PD) and understood English. Family caregivers had to be at least 21 years old and above.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.