
Abstract
Acquired brain injury (ABI) is one of the most common causes of disability and death globally. Support from informal caregivers is critical to the well-being and quality of life of people with ABI and supports the sustainability of global health and social care systems. This study presents an in-depth qualitative analysis of the experiences of eight British informal caregivers supporting someone with ABI. Semi-structured interviews were conducted with narratives transcribed verbatim and analysed using interpretative phenomenological analysis (IPA). Three superordinate themes were generated: making sense of brain injury; being consumed by caregiving; and, the changing self. These data highlight the impact of caregiving on the caregiver’s illness perceptions and sense of self. By identifying negative and positive changes in the caregiver’s sense of self, and dilemmas regarding the care recipient’s behaviour, we address less understood aspects of caregiver experiences. Caregiving can pose both challenges to the caregiver’s sense of identity and an opportunity for self-growth. Some caregivers exhibit resilience throughout their journey, with post-traumatic growth more apparent in the later stages of caregiving. Illness perceptions shape caregiver well-being and family dynamics and indicate the need to address stigmatisation and discrimination faced by ABI survivors and caregivers. Although some caregivers acquired positive meaning and enrichment from their caregiving, previously described challenges of ABI caregiving are supported. Overall, our findings support the need for timely psychological/mental health support for caregivers, caregiver education, and the provision of short breaks from caregiving.
Keywords
Introduction
Acquired brain injury (ABI), that is, any injury to the brain occurring during someone’s lifetime, is one of the most common causes of disability and death in adults (Maas et al., 2022; Menon & Bryant, 2019), often requiring long-term rehabilitation, support, and care (Peoples et al., 2011). An ABI can be non-traumatic in origin, for example, an internal event such as stroke or brain tumour; or traumatic, for example, due to an external event such as an assault or vehicular accident (Feigin et al., 2010).
ABI can affect a person’s physical, cognitive, social, and/or emotional functioning, with some people being impacted in all these domains and some in fewer (e.g., Ellis et al., 2013; Quinn et al., 2014; Satink et al., 2015). Physical, cognitive, social, and emotional challenges can persist for months or years post injury (Jourdan et al., 2016) (sometimes a lifetime) and require specialised care and support (Kreitzer et al., 2018). ABI ranges in severity from mild (generally with time-limited, resolving symptoms such as dizziness, nausea, and headache) to moderate, severe (with long-term symptoms such as fatigue, sensory problems, seizures, and physical/cognitive impairment; e.g., Brickell et al., 2018; Merriman et al., 2019), up to catastrophic (expected to result in permanent loss of brain function; Neal et al., 2018). Individuals with catastrophic ABI are often excluded from research due to the profound nature of their impairments, leading most studies on the effects of brain injury to concentrate on those with moderate to severe brain injuries (Ponsford et al., 2014). Following moderate and severe brain injury, individuals may have executive function difficulties (Jourdan et al., 2016) and may experience significant functional limitations affecting their activities and participation (e.g., communication, mobility, and interpersonal relationships). Due to its long-term impacts, moderate–severe ABI is a chronic health condition (Kreitzer et al., 2018; Masel & DeWitt, 2010).
Given the serious impacts of moderate–severe ABI, survivors often rely on informal caregivers, that is, family members, friends, or neighbours, to provide unpaid help and support with various aspects of daily living (including psychological, nursing, or instrumental support) (Kreitzer et al., 2018; Quinn et al., 2014). The support provided by caregivers is critical given the growing trend for early discharge from hospital and treatment and rehabilitation at home (e.g., Department of Health, 2014; The Scottish Government, 2019). However, as the occurrence of ABI is typically sudden and unexpected, families are generally not prepared for their new role as a caregiver, and they experience a range of impacts (Bäckström & Sundin, 2010; Greenwood et al., 2010; Satink et al., 2015). Caregivers express uncertainty about this rapid and unexpected change to their life and many have little prior knowledge or understanding of ABI (Lond & Williamson, 2022). The consequences of stroke and other brain injury have largely been described in terms of changes to physical function; however, cognitive and emotional impairments are notable (e.g., Hackett et al., 2014; Merriman et al., 2019), whilst being less visible. Caregivers have to face a range of complex changes to someone: cognitive, emotional, behavioural, and physical (Chan et al., 2009; Merriman et al., 2019).
There is compelling evidence that caregiving is a social determinant of health (Public Health England, 2021). Research has shown that caregivers of adults with a range of chronic health conditions may experience depression, fatigue, burden, burnout, anxiety, lower subjective well-being, and poorer levels of physical health compared to non-caregivers (Brickell et al., 2018; Manskow et al., 2017; Saban et al., 2016), and this is shown in studies of those caring for someone with an ABI (Feigin et al., 2010; Lond & Williamson, 2022). Compared with caregivers providing care to people with other chronic conditions (such as dementia), ABI caregivers typically report comparable or lower quality of life and mental health outcomes, and similar or higher levels of burden and grief (Jackson et al., 2009; Marwit & Kaye, 2006). The grief experienced by ABI caregivers is multifaceted (with caregivers often expressing the feelings of ambiguous loss) and develops over time (Gamgee et al., 2023; Holloway et al., 2019). A qualitative meta-synthesis of 39 studies exploring the impact of ABI caregiving on caregivers’ health and well-being identified a range of physical and psychosocial challenges that caregivers face (e.g., physical tiredness) and evidenced that ABI caregivers find it difficult to maintain a personal life alongside their caregiving role (Kokorelias et al., 2020). Given the care required by individuals with ABI, caregivers face persistent negative health consequences tied to the extended caregiving duration (Iwata & Tadaka, 2023).
Caregiver burden can impact upon the recovery of brain injury survivors, that is, brain injury survivors whose daily life is characterised by strained relationships and by unsupportive family members show less improvement on disability rating, level of functioning, and employability scores (Sady et al., 2010; Sander et al., 2002). Research shows that distressed caregivers can diminish the effectiveness of post-acute rehabilitation for care recipients (Sander et al., 2012). A mixed-method systematic review of 117 studies (Gaugler, 2010) focusing on the experiences of stroke caregivers showed that although caregiver depression, stress, and health status did not significantly change over time in quantitative evidence; the qualitative studies inferred a more dynamic view of ABI caregiving (see also, for example, Whiffin et al., 2015). Bermejo-Toro et al. (2020) also found that factors such as the time since injury and the level of dependence of those with ABI can predict caregiver challenges over time, that is, over time patients’ dependence levels change, and caregiver challenges may also shift. Therefore, recognising the dynamic challenges and support needs of caregivers of brain injury survivors following discharge to home is important both in terms of addressing caregiver well-being and in supporting care recipient’s recovery.
Research demonstrates that caregiving can also have benefits, such as a sense of pride derived from the role or increased resilience/strength in the face of adversity (Quinn & Toms, 2019); however, studies identifying positive experiences for ABI caregivers are limited (e.g., Las Hayas et al., 2014; Mackenzie & Greenwood, 2012). For instance, a quantitative study conducted with Spanish ABI caregivers evidenced that caregiving can be a source of satisfaction and was significantly related to the quality of life and post-traumatic growth of the caregiver (Las Hayas et al., 2014). A mixed-method systematic review of nine studies (Mackenzie & Greenwood, 2012) exploring positive experiences of stroke caregivers concluded that caregivers did identify positive experiences of caregiving, providing a more balanced view of their role. It has been also shown that factors such as social support and the survivor’s level of awareness of deficit may be important for rehabilitation outcomes (Ownsworth & Clare, 2006) and for caregiver satisfaction in their role (Ergh et al., 2002, 2003); that is, in caregivers with low social support, the survivor’s unawareness of deficit was adversely related to caregiver satisfaction. The literature regarding ABI caregivers’ outcomes (e.g., burden or gains) mostly quantifies these various phenomena in terms of incidence of psychological disorders or scores on scales to measure perceived outcomes; such studies assume the specific challenges or gains that hold significance for caregivers. However, there is dearth of literature that explores how ABI caregivers make sense of their own experiences (e.g., Gamgee et al., 2023; Ghosh-Cannell et al., 2023; Townshend & Norman, 2018; Whiffin et al., 2021).
The concept of self or identity defines who or what an individual is (Stets & Serpe, 2013). The only existing informal caregiver identity theory (Montgomery & Kosloski, 2009; Savundranayagam & Montgomery, 2010) conceptualises caregiving as a series of transitions emerging from a change of roles and identity (e.g., an adult child becoming a caregiver for their parent). Although this theory provides an important theoretical lens to help understand the role of self/identity in informal caregiver experiences, caregivers’ sense of self has rarely been studied (Hughes et al., 2013; Zarzycki et al., 2022).
Illness perceptions and how these influence coping and health outcomes have typically been studied in patient samples (Dempster et al., 2015; Rogan et al., 2013). Understanding of caregivers’ perceptions of their care recipients’ illness and the importance of these perceptions to caregiver outcomes is limited. There is some evidence (predominantly quantitative, and not within the ABI caregiver population) that illness perceptions play a significant role in caregiver stress (e.g., Pakenham, 2001), well-being (e.g., Bassi et al., 2016), and positive aspects of caring (Parveen & Morrison, 2012).
Within the field of ABI, research has mainly focused on the patient outcomes, with fewer investigating the experiences of their unpaid, typically family, caregivers. It is important to gain a deeper qualitative understanding of caregiver perceptions of self and of the illness and their effects, in the context of ABI so that support can be put in place. This paper reports findings from a qualitative study exploring these factors.
Method
Design
In line with the exploratory and inductive nature of the study, a cross-sectional qualitative design with semi-structured interviews aligned to the interpretative phenomenological analysis (IPA) framework was employed. IPA was chosen as it is committed to an idiographic level of analysis and is appropriate when exploring experiences within specific small samples and in developing knowledge from a ‘bottom-up’ approach. Richness of the data rather than the sample size is prioritised as it allows the interpretation of the participants’ experiences (Larkin et al., 2011; Smith et al., 2009).
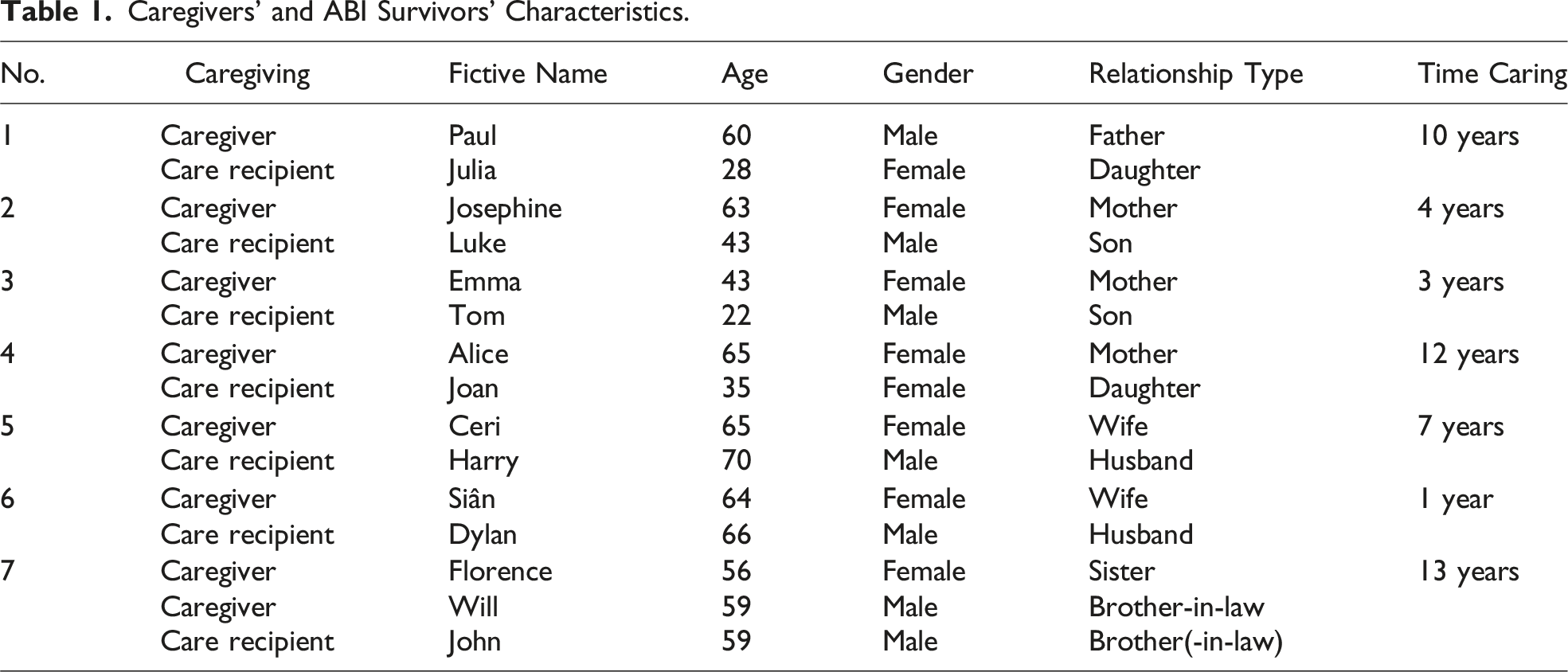
Participants
Caregivers’ and ABI Survivors’ Characteristics.
Data Collection
Prior to recruitment, full ethical approval was obtained from the University Ethics Committee at Bangor University (reference number: 2019-16561-A14834). Informed consent was obtained from all participants. Interviews were conducted in an authorised room at the university with one exception where, at their request, one caregiver was interviewed in their own home. Respite care and travel expenses, where these were incurred, were reimbursed for the participants. The first author (MZ) conducted all of the interviews. Congruent with gathering information about individuals’ lived experiences, interviews were participant-led, exploring topics that were personally significant, that is, an interview guide with prompts was used to help frame the discussions (e.g., feelings about caring). Interviews were recorded using an encrypted voice recorder, transcribed verbatim, and further supplemented by reflective process notes. Interview length ranged from 60 to 180 min (M = 112 mins).
Analysis
Interviews were analysed using IPA, following the broad analytical steps described by Smith and colleagues (2009). Transcripts were read and re-read to enable immersion in the data. Line-by-line analysis noted descriptive, linguistic, and conceptual elements of the data which facilitated the next stages of identifying emergent themes and identifying connections between them within one person’s account. Analysis continued consecutively across the remaining transcripts, before identifying patterns across transcripts to develop superordinate themes. Analysis was iterative and continued throughout the write-up.
The first author (MZ) conducted the analysis, meeting frequently with the other authors (DS, MP, and VM) to discuss the focus, organisational structure, and quality of the analysis. Authors discussed themes to ensure that the analysis satisfies the quality criteria for qualitative research (Tracy, 2010), including, for instance, ensuring the credibility of the results generated (e.g., that themes were well represented in the transcripts), resonance (e.g., the applicability of findings presented in relation to policy and practice contexts), and coherence (i.e., with the research design, methods, and presentation of findings aligned cohesively).
Reflexivity
During the research process, reflexivity was considered and discussed. Reflections of the first key author (MZ) can be found in S1 Supplemental Material.
Findings
Three superordinate themes provided rich interpretative phenomenological insights into the experiences of the ABI caregivers. 1. Making sense of brain injury 2. Consumed by caregiving 3. Changing self
The superordinate themes and their subthemes are presented, with illustrative quotes from the participants (pseudonyms are used).
Making Sense of Brain Injury
This superordinate theme reflects on caregivers’ perceptions of brain injury and includes three subthemes: understanding brain injury; living with limitations and losses; and living with an ‘invisible’ condition.
Understanding Brain Injury
Caregivers provided varying explanations of care recipients’ changed behaviours. There was a strong sense of caregivers’ dilemma in considering whether their care recipient’s behaviour was purposeful, arising from their personality, or whether it was an unintended consequence of their brain injury. For example, tiredness could be considered as dispositional laziness and forgetfulness as due to cognitive impairment or as intentionally manipulative. Such caregiver perceptions indicate a deeper struggle in interpreting and distinguishing between the effects of ABI and, for example, possible manipulative tendencies of ABI survivors. And I’ve just phoned you 10 minutes ago, why didn’t you put it in your prompts? “You know I’ve got brain injury!” So, she, she uses it as a tool. […] I know what she’s like and manipulative as well. (Paul) It just feels like sometimes he knows what he’s doing and that’s again frustrating because he knows what he’s doing to get away with it. (Florence) Okay, if they can’t understand something, keep finding other ways, you know, it’s not their fault. It’s your fault. And so, I guess that kind of understanding helps, whereas my husband didn’t have that at all. And then I think he thought I was naive and just didn’t realise Tom was being lazy. And I know he is a bit lazy as well, but he was struggling, and it was a lot. (Emma)
Living with Limitations and Losses
The cognitive and physical consequences of ABI were widely acknowledged by caregivers. Reflecting on their experiences, caregivers reported that these limitations and losses elicited a variety of intense emotions, including anger, sadness, grief, surprise, fear, and shame.
Often it was the neurocognitive consequences of the brain injury, not the physical/functional consequences (such as impaired mobility), that were emotionally challenging. For example, Siân found the damage to Dylan’s executive functioning frustrating and disruptive to her own life (e.g., interfering with daily planning); Paul had to deal with Julia’s unpredictable mood swings (‘depressive cycle’), and John’s lack of appetite control, acquired Brown’s syndrome (a disorder of ocular motility, i.e. rapid eye flickers or wandering gaze), and other problems with behavioural control meant that Florence and Will monitored him constantly as he could eat improperly/inappropriately or could not control his gaze in social situations. Also, he will take food, waste bins, dust bins and even animal’s food. He won’t ask for food. He will steal food. It doesn’t matter whether it’s mouldy or in a dustbin. He will take it and eat it. (Florence) So, there’s no no control with the hunger. And having no taste and no smell doesn’t help either. (Will) I mean, his limited mobility is bound to have an effect. You know, when before we were working, we had this dream of getting a camper van. He always wanted to have a camper van to go for the weekends and stuff. We haven’t got a camper van and it’s probably me not [being] so keen because he needs help at home. (Ceri) I think certainly in the early days, especially because he wasn’t himself, he is a lot more now, a lot more now, which makes me feel extra bad about feelings that had been, because it just wasn’t him. It was just somebody else stumbling around the house. And you know, just looking at him and looking at everything he lost was really, really hard. (Emma)
Living With an Invisible Condition
The responses of others (including those of strangers) and their perceived lack of awareness and understanding of living with a brain injury featured heavily in caregiver accounts. Whilst not all of their care recipients had an invisible condition, the invisibility of many symptoms, such as cognitive impairments which underpinned behavioural changes (as seen above), was considered contributing to a lack of public understanding.
The invisibility of the brain injury and its consequences was often thought to be the reason why the caregiving role was questioned by people in the community, with some challenging the existence of the care recipients’ health condition and consequent need for care (e.g., an assumption that if the brain injury survivor does not display physical symptoms of disability, they do not need any care). The behavioural consequences of an invisible health condition were a source of stigma or discrimination against the care recipient, as expressed by caregivers Josephine and Alice. Challenges to the need for caregiving and stigma/discrimination towards the care recipient were perceived as unjust. ... And then trying to explain to people the same thing and if you’ve got something physical people can see but you can’t see it in him. I’m not just mad, all the people I’ve seen – they’ve got stressed and angry [with him]. You see this in all different kinds of places. He can walk away in the middle of the conversation because he’s got brain injury. (Josephine) If you say that he’s going through food bins, eating, they say, “Well, obviously, they’re not eating ...” ... that he’s being starved [by us]. So again, it looks like we’re not looking after him, we’re not caring for him, all we’re there [for] is taking his money. (Florence)
Consumed by Caregiving
Caregiving was found to be all-consuming, with a negative impact on the caregivers’ physical health and mental well-being. For some, this generated an expressed need for short breaks from the caregiving role.
Consumed by the Caring Role
Prioritising the brain injury survivor’s needs led to feelings of exhaustion and helplessness, impaired self-care, and impacted negatively upon relationships within the wider family network. Siân depicted this by saying that “all is based around caregiving,” leaving little or no space for the life beyond the caring role. Alice, herself suffering from diabetes, stated that: It’s [my diabetes] never been easy. But suppose you shove it to the back of your mind. This [caregiving] is more important than ... you know. I know people say you’re supposed to put yourself first because if you’re not well you can’t help anybody else. But I think I’ve stuffed the diabetes for now. I’ve got more important ... Joan’s [the care recipient] more important than the diabetes. (Alice) But there were moments where you almost couldn’t move because you’re just hit by a big – not even a wave – it would just be like a big thump of overwhelming combination of nothingness and depression, all in one go probably just because you can’t take all the feelings and they just, you know, hit you like that. (Emma) And it still makes the future shaky, because it still leaves me thinking: Well, you know, I still need to be there. I still could have to stop everything anytime. (Emma) We’re actually more tied because of John and he thinks, “So?”, you know ... he doesn’t realise or whether he does realise, and he doesn’t care – we don’t know because he won’t say – he just … he says, “So?” and he just carries on, he doesn’t realise how much William and I have given up and we’ve tried to tell him. (Florence)
Recognising the Need for a Break From Caregiving
Although the caregivers made sacrifices and often neglected their own mental and physical health, they realised that they needed breaks from caregiving to attend to their own needs (e.g., have quality time alone and sleep more) and to sustain their caring role. Caregivers found different ways to have breaks. Breaks could arise from receiving relief support from family or from the care recipient engaging with activities (e.g., gym). [You] recharge your batteries, because you’re completely drained and so tired … er, we went on a cruise, and I think we slept more than we ... instead of just sunbathing, we actually stayed in our room and slept. (Will) I’ve been trying to just do more for me, you know, less thinking about what will make all the children happy and what’s good for them [including the care recipient] and just thinking a bit more about, you know, what I might want to do, what makes me happy? And I’ve been trying to do a bit more of that. (Emma) ... and in 13 years I think we’ve only [had] 3 holidays without him. (Will) Because we still take him at times as well. But when we go abroad with him, you know, we have to book basically, a separate villa, with its own little pool and things like that. Because it’s about staring with the kids and stuff. So, that’s a big problem … (Florence)
Changing Self
Here, we reflect on the impact of caring for someone who has experienced ABI on the caregiver’s sense of self: firstly, caregiving viewed as a threat to self (subtheme ‘Identity shift’); and secondly, caregiving as an opportunity for self-growth (expansion of self; subtheme ‘Post-traumatic self-growth’).
Identity Shift
Some caregivers spoke about the different ways the care recipient’s brain injury had influenced the feelings, attitudes, or beliefs they held about themselves. For example, Emma and Josephine questioned their self-identity and their roles as mothers as well as their moral convictions about sustaining life and dying. It was seen that conflict around sustaining life and dying delves into existential and moral dilemmas. These types of dilemmas challenged some carers’ core beliefs and values, such as the ‘maternal instinct’ to protect one’s child at all costs. Internal debate between wishing for an end to suffering and the inherent desire for one child’s survival underscores not only multidimensional nature of caregiver stress and guilt but also identity shift. I never wanted him not to be there anymore. But I think part of me sometimes gets thinking, “just do it, you’re going to do it” [to die], you know, and it doesn’t mean I wanted him to die. But in a way it must have been that, but I didn’t want that. To have had those thoughts about somebody, especially your own child, it’s an awful thing. (Emma) I feel that maybe a part of me changed a lot. And it’s been very hard to get close again to everybody else because it was just such a big thing. And I think because I didn’t know that – I mean the prognosis – in the first interview with the doctor, that neurologist, he started talking about, you know, death, epilepsy and sudden death and nobody had a clue with Tom … for a good period of time I had no idea if he would still be awake in the morning, you know and it was ... when you have to, when you have to live with that and get through it, it does change you and other things. I don’t know, I suppose I can’t let go in the same way you can’t relax, and you don’t want to fully enjoy it because you worry it might be taken away from you ... (Emma) It does affect you because you don't want to see ... well, it affects because you can’t do anything. [pause, crying] Sorry. […] And then you wonder how much longer you can carry on. (Josephine)
Post-Traumatic Self-Growth
As noted, caregiver’s well-being was challenged; however, for some, these challenges offered opportunity for reflection. Oftentimes, it was a healing process of the burdened or traumatised self that could be termed as a post-traumatic self-growth. Five of the eight caregivers revealed that the experienced trauma or burden enabled them to become stronger and to grow (Josephine, Florence, and Will’s accounts did not refer to self-growth). Caregivers reported they found a sense of strength (e.g., ability to cope with challenging situations) or developed a different outlook on life (e.g., they started valuing life more), and that this experience, which could be termed post-traumatic self-growth, happened subsequently to the traumatic change in self experienced (see the subtheme ‘Identity shift’ above).
Alice noted the inner strength she gained following her daughter’s stroke/brain injury. Yeah. I’m stronger than I thought I was. (Alice) Well, because we’ve moved so far down the road, I guess, anything I wanted to change has changed already. You know, I think, thankfully and luckily, we have got to that point. Yeah, the overriding thing is just wanting things to carry on getting better or at least just stay the same. And just that that little bit of me just to get better again really. (Emma) But it’s something that I learned from, you know, nearly 10 years of experience with her now, you know […] in helping her, I find that I’m helping myself. (Paul)
Discussion
This study explored the everyday lives of caregivers supporting someone who had an ABI. The findings are presented as three superordinate themes: making sense of brain injury; being consumed by caregiving; and changing self. Firstly, changes in the caregivers’ sense of self are notable in this study – providing care was seen as both a threat to self and an opportunity for self-growth, with the latter likely developing over time for some caregivers. Secondly, this study highlights the importance of illness perceptions to caregivers’ experience and well-being. Caregivers’ retrospective and reflective accounts point to change over time in how caregivers consider the illness impact and their care recipient’s needs. Thirdly, the study confirms previously described challenges and needs of ABI caregivers (e.g., Kokorelias et al., 2020), for example, for recognition and support from others including the lay public, for short breaks from a caring role.
Impact on the Sense of Self: Post-Traumatic Growth and Resilience
Subjective experiential changes are increasingly recognised as important factors underpinning recovery and rehabilitation following ABI, and this may also include the changes in the caregiver’s sense of self (e.g., Abrahamson et al., 2017; Whiffin et al., 2019). Changes in the caregiver’s sense of self were evident in caregivers’ narratives (see the superordinate theme ‘Changing self’), a dynamic process recalled throughout the caregiving career. In a study conducted by Abrahamson et al. (2017), where 41 brain injury survivors and their caregivers were interviewed, the authors recognised a phenomenon of the ‘self-identity disintegration’, characterised by an awareness of the profoundly different life in the post-injury existence for both ABI survivors and caregivers. For example, our findings show how caregivers’ struggles with navigating the line between prolonging care recipients’ life and alleviating their suffering (Holloway et al., 2019) underlie self-identity disintegration. Although there are several studies exploring the sense of self or identity in ABI survivors (see, for example, a qualitative meta-synthesis of 23 studies by Levack et al., 2010), only a small number of studies have considered the changes to the caregiver’s sense of self (Abrahamson et al., 2017; Couchman et al., 2014; Whiffin et al., 2019). What was clearly evidenced in our data is that caregiving following the care recipient’s brain injury can be an opportunity for caregivers’ self-growth, that is, changing sense of self. The superordinate theme ‘Changing self’ presents the positive aspects of the caring role, uncovering factors that may promote well-being for ABI caregivers. Consistent with scarce previous research, mainly outside the brain injury caregiving context (e.g., Hallam & Morris, 2014; Thornton & Perez, 2006) but with some studies in the context of brain injury (e.g., Powell et al., 2012; Simpson & Jones, 2013), caregivers manage to find positive meaning and enrichment in distressing circumstances. As evidenced in findings, the difficult experiences of caregivers can, for some, result in post-traumatic growth and increased resilience. In the meta-synthesis of 30 qualitative studies focused on caregivers providing care to someone with a traumatic brain injury (Whiffin et al., 2021), “the incredible positive potential” exemplified by some caregivers was highlighted (p. 17). In the context of the current study findings, we highlight that ‘the incredible positive potential’ may be underpinned by caregiver resilience and post-traumatic growth. In the United Kingdom, despite the general inadequacy of long-term services for caregivers and ABI survivors (Norman et al., 2023), certain interventions have demonstrated effectiveness in enhancing positive outcomes for caregivers/care recipients. For example, interventions such as the Brain Injury Family Intervention have improved family resilience and well-being (Bushnik et al., 2015). The resilience of those supporting relatives with TBI or spinal cord injury has been also shown to be crucial in coping with caregiving challenges (Simpson & Jones, 2013). Additionally, social communication partner training has been effective for adults with severe chronic TBI and their caregivers, enhancing communication skills, which are a component of caregiver support and resilience (Togher et al., 2016). These findings indicate that targeted interventions can significantly aid caregiver resilience and post-traumatic growth in the ABI caregivers. It is also important to distinguish between caregiver resilience and post-traumatic growth. Resilience is understood as the ability to adapt or to improve one’s own conditions following experiences of adversity (Limardi et al., 2016). Post-traumatic growth is the experience of positive change resulting from very hard personal crises (Tedeschi & Calhoun, 2004). We propose that resilience may be seen as a resource factor that caregivers may develop during the course of caregiving, whereas post-traumatic growth unfolds later in the course of caregiving and is subsequent to the traumatic change in self experienced (see the subtheme ‘Changing self’ above), the reflection on how caregivers coped with challenges and on their attempts to incorporate the trauma/challenge into their life (Jones et al., 2020).
Illness Perceptions
As noted at the outset of this paper, there is a gap in research on caregiver illness perceptions with respect to ABI caregiving. Our study findings reveal that illness perceptions have an important impact on caregivers’ well-being and on their relationships with other family members (see the superordinate theme ‘Making sense of brain injury’). It is clear that the occurrence of an acute-onset health problem with chronic consequences, like ABI, affects not only patients but also caregivers, whose perceptions and responses may in turn enhance or impede a patient’s own coping responses and consequent adjustment to illness (Karademas et al., 2010; Weinman et al., 2012). Caregivers’ different ways of ‘making sense’ of the brain injury were a source of dilemma/uncertainty regarding the care recipient’s behaviour: is their behaviour a product of their personality or intentional (where they assume the ‘sick role’; Parsons, 1975) or an unintentional consequence of brain injury? Inevitably, caregivers’ responses to the care recipient, both behavioural and emotional, are dependent on their illness perceptions and beliefs. Caregivers reported inadequate support in their roles in relation to learning about ABI and its impact (Holloway & Tasker, 2019). This in turn may impact caregivers’ ability to effectively manage the care and rehabilitation of an ABI patient. There is need for information provision as well as educational training that could address caregivers’ illness perceptions.
Caregivers in this study reported differences in the interpretation of their care recipient’s behaviour and in recovery expectations amongst family members, which could lead to tensions. ABI caregivers have to deal with cognitive and emotional impairments that are often invisible to others in addition to any physical impairments (Jourdan et al., 2016; Merriman et al., 2019). As seen in the data, a caregiver’s illness perceptions may have a negative impact on the relationship between the caregiver and care recipient (e.g., if the caregiver thinks that the ABI survivor is being lazy instead of being fatigued) and the relationship between the caregiver and other family members.
In a broader societal context, caregivers referred also to the responses of other people towards the brain injury survivor and caregivers themselves, that likely arise from their lack of awareness and understanding of the health condition, its consequences, and the associated need for caregiving. In some cases, where the functional changes associated with brain injury are largely invisible (see the subtheme ‘Living with an invisible condition’), individuals living with a brain injury may not be routinely identifiable. Previous studies have attempted to explain the public’s misconceptions about brain injury as experienced by professionals and families of people with brain injury (e.g., McClure, 2011). For example, misconceptions can occur because people misattribute the actions of brain injury survivors (e.g., to rudeness and drunkenness) due to the absence of visible markers of the injury (‘invisible condition’). This misattribution can lead to stigma: a failure amongst members of the public to recognise that care recipients’ challenging/problematic behaviours may result from brain injury (McClure, 2011). However, these study findings show that the stigma was also felt by the caregivers: with the members of the public failing to recognise that caregiving is needed.
Previous research shows that some people living with a disability such as brain injury experience significant and damaging prejudice (Gwyn, 2003; Riley & Hagger, 2015): an issue mentioned by two caregivers in this study in relation to the people they supported. This is particularly the case when brain injury survivors decide not to disclose their injury to others and carry disability under the mask of normality (Lupton & Seymour, 2003). This fear of stigma or prejudice can lead people living with brain injury to self-exclude (as seen in case of Josephine’s care recipient), fulfilling to a certain degree the social outcome they anticipated (Reidpath et al., 2005). Decreasing social circles, loss of key relationships, and a sense of loneliness are documented phenomenon for people living with brain injury (Claude Blais & Boisvert, 2005; Salas et al., 2018). The importance of addressing brain injury survivors’ stigmatisation and discrimination should be stressed for both brain injury survivors and their informal caregivers as such factors are crucial in terms of caregivers and care recipients’ well-being, and the caring relationship.
Caregiving Challenges
As our data have shown, the physical, cognitive, behavioural, and emotional changes that occur with a brain injury can all place significant demands on the caregiver (see the superordinate theme ‘Consumed by caregiving’). Numerous issues, including anxiety, depression, emotional distress, family strain, adjustment problems, and the ABI survivor’s loss of insight (related to caregiver burden), have been documented in studies of caregivers of people with brain injury – pointing to the critical issue of identifying and addressing caregiver support needs (e.g., Holloway et al., 2019; Jourdan et al., 2016; Kreutzer et al., 2016; Norman et al., 2023). The current findings also highlight some generic needs, similar to those found amongst caregivers caring for people with different health conditions (e.g., Amer Nordin et al., 2019).
Support needs of those providing care to brain injury patients have previously been shown to include emotional and financial support, counselling and education, respite care/short breaks, peer support, equipment access, and assistance with in-home care assistance (Bellon et al., 2015; Kitter & Sharman, 2015). The current qualitative findings, obtained in the British context, support these findings. Specifically, caregivers in this study highlighted the need for breaks from caregiving taken apart from their care recipient. This is perhaps not surprising given the frequent challenging behaviours displayed by brain injury survivors (but not limited to this subpopulation) which include impulsiveness, mood changes, irritability, memory problems, fatigue, temper outbursts, and anxiety, all of which having a potential to contribute significantly to caregivers’ burden (Kitter & Sharman, 2015). Being able to access regular breaks from caregiving is vital for informal caregivers, helping them to relieve their stress, look after their own health, enhance their well-being, and enjoy a life alongside caregiving. Breaks can help sustain the caring relationship and avoid the need for crisis support (Carers UK, 2021; Seddon et al., 2021). Secondly, our findings highlight the need for information provision, due to the problems with understanding the changes involved with brain injuries and seeking information as to how to cope with the psychological and physical effects of the brain injury. Similar findings have been noted in an earlier qualitative study (Townshend & Norman, 2018). Thirdly, counselling and emotional support is important given the mental health challenges expressed by caregivers in this study (e.g., depression, anxiety, and psychological trauma). Services providing breaks, counselling, information provision, and educational training should be available to caregivers (Bellon et al., 2015; Chan et al., 2009; Norman et al., 2023) and responsive to caregivers’ individual circumstances and the challenges they face, and delivered flexibly, given the ongoing grief and ambiguous loss often experienced by ABI caregivers (Holloway et al., 2019; Lond & Williamson, 2022). Caregiver support should be delivered flexibly to accommodate the complex emotional landscape caregivers navigate, marked by the enduring presence of loss. This qualitative study also suggests that it is crucial that services are available to caregivers along the spectrum of recovery (at the time of the incidence, during the discharge from in-patient care, and during outpatient care); each ‘caregiving journey’ is unique, and different recovery trajectories are evidenced (decline, improvement, or stabilisation).
Limitations and Strengths
The timeframe between brain injury onset and the interviews for some participants could bring their memory recall into question. Given that previous research and our current findings show that caregiver burden and illness perceptions change over time, future (IPA and other) studies should adopt a longitudinal approach exploring the emergence of experiences and perceptions over time, in contrast to the retrospective and cross-sectional accounts presented here. A 22-year age range and a difference in time spent caregiving (stretching from 1 to 13 years) were present within the sample, indicating some heterogeneity. The inclusion of the potentially divergent needs and experiences of those in later life and middle-aged, at different points of their caregiving career, and varying relationship types to the care recipient (e.g., parental and spousal), may introduce further potentially problematic heterogeneity into the analysis and impact the findings presented. It also needs to be acknowledged that the experience of recovery for different caregivers may differ, for example, when no recovery is achieved, and allied to this the support needs may be different. Moreover, due to ethical reasons, the data on the nature of the care recipient’s ABI (e.g., stroke and TBI) has not been collected from caregivers.
This paper presents findings related only to caregivers’ perspective and does not explore the relational experiences, as enacted by both the caregiver and the person with ABI. This may of course present some challenges where the person with ABI has moderate–severe cognitive impairment. Future efforts to enhance our understanding of dyadic experiences would likely benefit emerging dyadic approaches for supporting a caring dyad (Lond & Williamson, 2022). Similarly, triadic experiences that include the caregiver, the person with support needs, and the professionals involved in helping should be included. Exploration of caregiver challenges across the entire family/friend networks may give greater insight into caregivers’ needs and how to further improve well-being of all involved. The Most Significant Change (MSC), a dialogical, story-based, and participatory qualitative technique, may be a potentially suitable method to capture and assess qualitative accounts and changes in dyadic/triadic qualitative research (Dart & Davies, 2003). Moreover, the current body of empirical literature necessitated the inclusion of references to strokes and other types of ABI in both the Introduction and Discussion sections. It needs to be highlighted, however, that whilst stroke and other forms of ABI are frequently discussed together, the distinctions in their pathophysiology, demographic profiles, and clinical manifestations caution against treating them as fully comparable.
The study employed an interpretative phenomenological approach, enabling caregivers to identify and reflect upon the aspects of experience they considered most significant when providing care to an ABI survivor and how this caregiving experience has affected their everyday lives. Despite the abovementioned limitations, the research findings contribute to understanding the impact of ABI caregiving and caregivers’ perceptions on a person’s sense of self and potential for a post-traumatic growth and confirm the variety of challenges faced in the caregiver role.
Conclusion
Firstly, caregiving can represent both a threat to self and an opportunity for self-growth. We suggest that resilience emerges over the course of caregiving whilst post-traumatic growth manifests later in the course of caregiving, following the traumatic change in self experienced. Secondly, the study emphasises the important role of illness perceptions in shaping caregivers’ well-being and family relationships. In line with the past research, addressing stigmatisation and discrimination experienced by brain injury survivors and caregivers is an important aspect for the overall well-being of the caring dyad. Thirdly, this study confirms the variety of challenges faced by ABI caregivers and highlights their need for recognition, support, and respite/short breaks. Especially, the significance of short breaks from caregiving (separately from the care recipient), information provision, educational training, and emotional support are highlighted.
Supplemental Material
Supplemental Material - Supporting Individuals With an Acquired Brain Injury: An Interpretative Phenomenological Study Exploring the Everyday Lives of Caregivers
Supplemental Material for Supporting Individuals With an Acquired Brain Injury: An Interpretative Phenomenological Study Exploring the Everyday Lives of Caregivers by Mikołaj Zarzycki, Diane Seddon, Milica Petrovic, and Val Morrison in Qualitative Health Research
Footnotes
Acknowledgments
Thanks to Prof Andrea Gaggioli (Università Cattolica del Sacro Cuore) for his helpful comments on an earlier draft.
Author Contributions
Conceptualisation: MZ and VM; data curation: MZ; methodology: MZ and VM; investigation (interviews): MZ; formal analysis: MZ and MP; writing (original draft): MZ; writing (review and editing): MZ, MP, VM, and DS; and supervision: VM and DS.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. All authors listed have made a substantial, direct, and intellectual contribution to the work, and approved it for publication.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This qualitative study was funded by the EC-funded Marie Skłodowska-Curie Innovative Training Network (H2020-MSCA-ITN-2018), grant agreement no. 814072. The funder has not had any role in the preparation of the manuscript.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.