
Abstract
Introduction
Effective home care is critical to preventing complications and promoting recovery after Coronary Artery Bypass Grafting (CABG) surgery. In low- and middle-income countries like Pakistan, limited professional home care services place the responsibility for post-CABG care largely on family caregivers (FCGs), often without training or support. Understanding their challenges is essential for improving recovery outcomes.
Objective
This study aimed to explore the challenges faced by FCGs in providing post-CABG care at home after hospital discharge.
Methods
This qualitative exploratory descriptive study included 19 FCGs of Post-CABG patients, purposively recruited from cardiac outpatient department in a public hospital in Pakistan. Data were collected through face-to-face semi-structured interviews and analyzed using Creswell's content analysis.
Results
Six categories emerged: learning curve and adaptation, lack of information and guidance, physical and emotional strain, financial strain, hospital and healthcare challenges, and family support. FCGs felt unprepared for managing diet, wound care, and pain, while reporting fatigue, emotional distress, and high costs. Though family support offered some relief, gaps in medical support, communication barriers, and difficulties with follow-up intensified their burden.
Conclusion
FCGs of post-CABG patients in Pakistan face significant informational, emotional, physical and financial challenges worsened by healthcare system gaps. Nurses can play a central role by providing structured predischarge education, ongoing follow-up and culturally appropriate, family-centered support to strengthen FCGs capacity and improve patient recovery.
Keywords
Introduction
Cardiovascular diseases (CVDs) remain the leading cause of mortality worldwide, accounting for one in three global deaths, with 20.5 million fatalities in 2021 alone (World Heart Federation, 2023). The burden is significantly higher in low- and middle-income countries (LMICs), where 80% of CVD-related deaths occur (Roth et al., 2020). Pakistan, a LMIC with population exceeding 240 million, faces a critically high CVD mortality rate of 357.88 per 100,000, well above the global average of 239.85 per 100,000, where coronary artery disease (CAD) is predominant contributor (Samad & Hanif, 2023).
Coronary Artery Bypass Grafting (CABG) remains a cornerstone intervention for CAD, performed globally to restore myocardial blood flow and improve patient survival (Arsalan & Mack, 2016). Pakistan performed over 20,000 CABG surgeries in 2016, more than half of all 38,000 procedures conducted in South Asia, reflecting the increasing demand for surgical cardiac care in the country (Hosain et al., 2017). While CABG enhances patient outcomes, recovery requires careful postoperative management to prevent complications such as pain, edema, pleural effusion, limited mobility, and psychological distress (Ahmad et al., 2021).
With shorter hospital stays, post-CABG care has increasingly shifted from hospitals to home settings. In LMICs, where formal home care services are limited by financial and structural constraints, family caregivers (FCGs) often take on critical caregiving responsibilities such as wound care, symptoms monitoring, medication adherence, and emotional support (Bjornnes et al., 2019; McDonald et al., 2017). In Pakistan's sociocultural context, caregiving typically falls on spouses, children, or siblings and is influenced by strong familial and cultural norms.
Unlike Western healthcare models where professional home-care or transitional nursing support is available, Pakistani FCGs navigate complex tasks without formal training or systemic support. Observations by nurses in cardiac surgery units have revealed that FCGs often struggle to recognize early complications, manage wound care, and ensure medication adherence, leading to preventable readmissions (Javed et al., 2025).
Evidence from high income contexts demonstrate that nurse-led transitional care programs, including discharge education, home visits, telephonic follow-ups, and telehealth platforms enhance FCGs preparedness and patient outcomes following CABG (Berno et al., 2024; Gohari et al., 2022; Mares et al., 2018). Telehealth interventions, such as video consultations and remote symptom monitoring, have proven effective in extending post-CABG care in these contexts (Aydin & Celik, 2024; Ni et al., 2022). However, there is limited LMIC-specific evidence on the role of nurses and telehealth in supporting FCGs after CABG, particularly in Pakistan where formal home-care infrastructure is absent. Therefore, understanding the challenges of FCGs in Pakistan is critical for designing nurse-led, culturally sensitive interventions that bridge existing care gaps and improve post-CABG recovery outcomes.
Review of Literature
The literature shows that FCGs providing post-CABG care, encounter physical, psychosocial, financial, and informational issues. Studies report fatigue, sleep disturbances, and musculoskeletal pain, due to physical strain of assisting patients with mobility and daily activities (Bahrami et al., 2014; Halm, 2016). Continuous caregiving demands alongside household and work responsibilities exacerbate role conflict, creating stress, and emotional strain (Kim et al., 2020; Park et al., 2016). Managing patient behaviors, such as medication nonadherence or reluctance to adopt dietary changes or activity restrictions, further adds to their burden (Bangerter et al., 2018).
A recurring issue is inadequate information and preparedness. Many feel unprepared for home care, experiencing distress due to insufficient knowledge about wound care, medications schedules, and complications recognition (Bangerter et al., 2018; Blair et al., 2014; Solórzano et al., 2021). Inadequate education on symptom monitoring and emergency preparedness leaves them uncertain, increasing risk of ineffective care (Bahrami et al., 2014).
Another challenge is lack of assistance and support. FCGs frequently feel isolated due to increasing demands on their time, and diminishing social interactions (Chi et al., 2018). Studies report that FCGs showed concerns about inadequate support from family, making them feel frustrated (Bangerter et al., 2018; McIlfatrick et al., 2018). Financial strain due to reduced work hours, medical expenses, and lack of financial support further worsens their situation (Chi et al., 2018).
Despite sufficient international literature on challenges faced by FCGs of CABG patients, a critical gap exists in the Pakistani context, where caregiving is profoundly shaped by religious beliefs, sociocultural values, and familial expectations. In a setting marked by traditional caregiving roles, financial constraints, and limited institutional support, FCGs likely face unique challenges and intensified caregiving burdens that remain unexplored. To address the gap, this study explored the challenges faced by FCGs in providing post-CABG care at home after discharge from hospital, aiming to inform targeted nursing interventions to better support FCGs and enhance patient recovery outcomes.
Methods
Study Design
This study employed an exploratory descriptive qualitative design. This approach is well-suited for gaining an in-depth understanding of complex phenomena, particularly when existing knowledge in the context is limited (Grove et al., 2017; Polit & Beck, 2017). By adopting this design, the study aimed to explore and comprehensively describe the caregiving challenges encountered by FCGs while providing post-CABG care at home.
Study Duration and Setting
The study spanned over 6 months, from March to August 2024. The study was conducted in the cardiac out-patient department (OPD) of a public tertiary care hospital in Islamabad, the capital city of Pakistan. As the only public sector hospital in the capital, serving patients from across the country including Punjab, Khyber-Pakhtunkhwa, Gilgit-Baltistan, and Azad Kashmir, this setting was chosen to ensure geographical representation of participants.
Study Population
The study population comprised FCGs of CABG patients, including spouses, children, and siblings, whose experiences on caregiving challenges were considered essential to the research. The study included FCGs who met the following criteria: (1) aged 18 years or older, (2) spouse, sibling, or child of patient who underwent CABG surgery within the past 3 months, and (3) ability to understand Urdu (national language). FCGs were excluded who had active psychiatric illness requiring medication.
Sampling and Sample Size
A Purposive sampling technique was used to recruit study participants. In qualitative studies purposive sampling is preferred to select participants with necessary experience and to ensure maximum diversity (Creswell & Creswell, 2018, p. 423; Sandelowski, 2010). The sample size was guided by the principle of data saturation, defined as the point at which no new themes or subcategories emerge and additional interviews provide redundant insights (Hennink & Kaiser, 2022). Data collection continued until saturation was reached, resulting in a total of 19 face-to-face interviews and ensuring a comprehensive understanding of participants’ experiences.
Recruitment and Data Collection
The unit in-charge and head of department were approached to request permission and facilitation in data collection at the study hospital. A flyer was also posted in the cardiac OPD to disseminate information about the study and to invite potential participants. Eligible participants were identified and invited during follow-up visits of CABG patients in the OPD, in collaboration with the consultant. Those who agreed to participate were directed to a separate room, where they were briefed about the study, provided written informed consent and scheduled their interview at a date, time and location of their choice, either at home or hospital.
Face-to face, semi-structured interviews were conducted in Urdu, lasting 30–45 min, with audio recording after obtaining permission from the participants. Interviews were conducted using an interview guide with open-ended questions (Supplementary File 2). Prior to data collection, two mock interviews were conducted, with audio recordings and transcripts reviewed by the supervisors. Based on their feedback, refinements were made to improve question clarity and to enhance probing techniques. Field notes were also taken to record participants’ emotions and nonverbal responses during the interview.
Data Analysis
Data analysis aimed to organize, structure, and produce the actual meaning from the raw data (Polit & Beck, 2017). The manual content analysis method was employed following the steps described by Creswell and Creswell (2018) outlined in Table 1.
Steps of Data Analysis (Adapted from Creswell & Creswell, 2018).
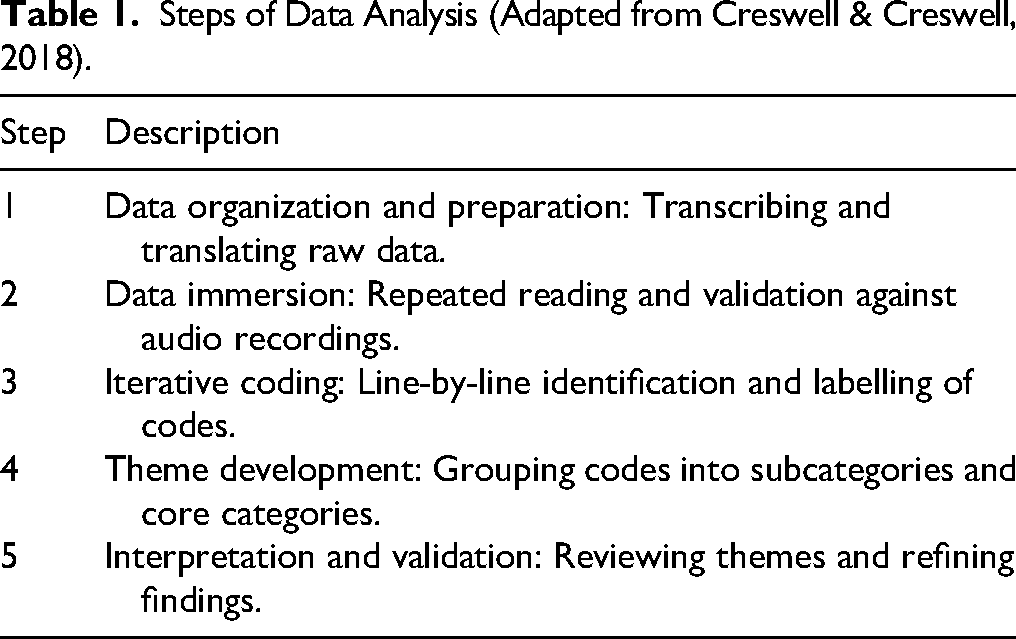
First, the data were organized and prepared for analysis by transcribing audio recordings in Urdu and translating them into English using a one-way translation approach, validated by the supervisors. Second, the transcripts were read and re-read, validating them against audio recordings with the supervisors to ensure accuracy and completeness. Third, meaningful units were identified and labeled with codes through a detailed line-by-line reading of the transcripts. Fourth, similar codes were merged, and opposing ones reconciled to form new subcategories, which were then grouped into distinct categories. Finally, the analysis was thoroughly reviewed and the findings were interpreted to derive meaningful insights and gain a deeper understanding, answering the research question.
Study Rigor
Lincoln and Guba (1986) five criteria for trustworthiness, including credibility, confirmability, dependability, transferability, and authenticity, were applied to ensure rigor of the study. Credibility was ensured through prolonged engagement with the study participants, enabling thorough exploration of participants’ experiences. Reflexivity was applied by acknowledging that the researcher's prior clinical and academic experience in cardiac care could influence data collection and interpretation. Measures such as adherence to the interview guide, neutral probing, and careful documentation were employed to minimize bias and enhance credibility. Reflexivity was maintained throughout the research process, as the primary researcher continuously reflected on how her prior clinical and academic experience in cardiac care could influence data collection, interpretation, and analysis. Confirmability was established through an audit-trail documenting all methodological decisions, coding processes, and data interpretations, ensuring transparency. Dependability was ensured by cross-checking transcripts with audio recordings to eliminate errors and maintain accuracy. All interviews were conducted in Urdu and subsequently translated into English for analysis. To ensure linguistic accuracy and conceptual equivalence, translations were verified by bilingual experts and cross-checked against the original transcripts. These steps enhanced dependability and confirmability of the data. Consistency in data analysis was further maintained by using code-recode strategy, where transcripts were coded several times to ensure reliability. To address transferability, purposive sampling was employed to select participants with diverse perspectives, ensuring a rich, detailed data collection to allow findings to be applicable to other contexts. Thick descriptions of the study context and participants’ sociodemographic characteristics further enhanced transferability. Authenticity was maintained by fostering a respectful and inclusive environment, ensuring clear communication, valuing participants’ perspectives. Furthermore, discussions with the supervisors and peer debriefing helped refine interpretations and uphold authenticity.
Ethical Considerations
Approval for this study was obtained from the institutional review board and ethics committee of the university (IRB 157-24) and the ethics review board of the study hospital (ERB 1279/2024). Written informed consent was secured from all participants after they received briefing on the study including its purpose, data collection, and voluntary participation. The participant's personal information was kept private, with only research team having the access to all participant data. Anonymity was maintained by assigning an ID to each participant, hiding their names. The collected data were stored securely in a safe, private, and lockable cabinet in hard copies while digital data were safeguarded in password protected computer files.
Results
A total of 19 FCGs participated in this study, representing diverse familial roles, including sons (n = 8), wives (n = 4), daughters (n = 4), brothers (n = 2), and a nephew (n = 1). Both genders were included, comprising 12 (63%) men and 7 (37%) women. FCGs’ ages ranged from 20 to 55 years, with an average age of 45 years. Most were married (74%) and had varying educational backgrounds, from no formal schooling to postgraduate degrees. Monthly household income ranged between PKR 10,000 and PKR 125,000, with the majority belonging to a low socioeconomic background. Ethnic diversity was reflected, with 12 (63%) identifying as Punjabi, 6 (32%) as Pathan, and one (5%) as Kashmiri. Majority (58%) resided in a joint family system. A detailed breakdown of FCGs’ sociodemographic characteristics is provided in Table 2.
Sociodemographic Information of Participant FCGs (n = 19).

The analysis of interviews data identified six main categories and 20 subcategories, as outlined in Table 3. The interviews were translated into English therefore grammatical corrections were made where needed to enhance the readability and clarity of participants’ quotes without altering their meaning.
Analysis of Interviews Data.

Learning Curve and Adaptation
This category captures FCGs’ journey of adapting to their new caregiving role, from initial challenges to developing confidence and skills. It consists of three subcategories: initial learning and training, gained experience over time, and significant recovery.
Initial Learning and Training
In the early post-CABG period, FCGs faced a steep learning curve, feeling the need for learning information related to patient's condition, use of medications, and care procedures. One FCG stated, “Giving him [the patient] medicine was the bigger problem after surgery. We felt the need for information from the hospital on how to give proper medicine and perform care” [FCG 15].
FCGs gained confidence by acquiring knowledge and skills related to patient care tasks as one FCG expressed: “I learned a lot; tasks like cleaning the wound, giving medication and mobilization were new to us” [FCG 12/1].
Gained Experience Overtime
FCGs’ gained experience over time and refined their methods of care. As one of the FCGs stated: “The experience was tough but gradually, I learned everything, like giving medicine, bathing, and cleaning the wound. Now it is easier” [FCG 14]. Another participant shared: “from day one, I have been taking care of him [the patient] and I believe, I have learned so much and refined my methods of care” [ FCG 5].
Significant Recovery
Despite early challenges, FCGs noted a significant improvement in patient recovery. One FCG shared, “when we went home, there were initial difficulties with care, but later the experience improved, his [the patient] health improved and improved mobilization” [FCG 3]. Similarly, another FCG expressed: “Alhamdulillah, with time and experience, my father is now better like his diet and sleep is improved” [FCG 12/1].
Lack of Information and Guidance
This category of “lack of information and guidance” is divided into three subcategories: dietary challenges, medication and wound care management, and blood pressure and sugar management.
Dietary Challenges
FCGs frequently highlighted the challenge of insufficient instructions about dietary intake and nonprovision of diet plan upon patient's discharge from the hospital. One FCG asserted: “We were not given any instructions on what should be added to the diet or what to avoid. There were no specific instructions given to us about what kind of food we should be aware of” [FCG 8/1].
Another FCG expressed unavailability of a diet plan for post-CABG patient who was also diabetic. He illustrated: We could not give him [the patient] anything sweet or food that would raise sugar levels because if the sugar goes high, his wounds would not heal properly, which was also a challenge for us. The hospital staff should have provided us with a proper diet plan, highlighting this food to give and that to avoid [FCG 8/1].
Medication and Wound Care Management
FCGs faced challenges with medication and wound care management, expressing lack of information about administering medicine, and guidance on wound care. One FCG highlighted: “There were difficulties with administering medication. The medical store staff provided us with the necessary information, telling us how to give and when to give it. The hospital staff did not provide any information on this” [FCG 3].
FCGs were disturbed by inadequate discharge instructions about wound care at home. One FCG narrated: “Since it was a major surgery, we needed expert guidance on wound dressing, and it was essential to follow the precise instructions. If we had received detailed instructions, we might have managed the wound care better” [FCG 6].
Blood Pressure and Sugar Management
FCGs reported difficulties in monitoring and managing blood pressure and sugar levels of post-CABG patient. One FCG, who was patient’ son stated, “Initially, we didn’t receive specific information from the hospital on how to check blood pressure and sugar, but later we got information from outside on how to use the machines” [FCG 7].
FCGs expressed their dependence on external sources due to the lack of training on how to check blood pressure or sugar levels. One FCG stated, “For blood pressure and sugar, we relied on the local dispenser who came daily for wound dressing. I didn't know how to check blood pressure or sugar, we were dependent on him for checking and managing it” [FCG 6].
Physical and Emotional Strain
This category covers the physical and emotional challenges faced by FCGs, reflecting their physical hard ships and inadequate emotional support. The category is divided into five subcategories: mobilization and physical assistance, disruption of sleep, emotional and psychological distress, household management and routine disruption, and balancing job and caregiving responsibilities.
Mobilization and Physical Assistance
This subcategory highlighted FCGs’ difficulties in lifting and moving the patient. One FCG, who was a wife and elderly lady, expressed difficulties in moving and lifting the patient, stating: “Taking care of him [the patient] is challenging because my age has also advanced, making it hard to lift, seat, move, and take him to the washroom [FCG 1].
FCGs expressed that moving patient to the bathroom was the biggest problem and it required special attention and care. One FCG affirmed, “The biggest problem we faced at home was when we had to take him to the washroom. We needed special care to help him sit down and get up” [FCG 3]. Similarly, another FCG shared, “I used to call my son or daughter-in-law for help while seating and bathing him. I needed a helper” [FCG 1].
Disruption of Sleep
FCGs reported that patients struggle to sleep during the first week after surgery due to recovery related problems such as wound pain, coughing, and breathing difficulties keeping them awake around the clock to provide care and comfort to their loved ones. One FCG affirmed, “when my father couldn't sleep through the night, my mother had to stay up all night as well. We also stayed up with him to ensure nothing happened to him” [FCG 7]. Similarly, another FCG stated, “Initially, sleep was disturbed because he [the patient] woke up every one to two hours, and we all had to stay awake, myself and my children, taking turns to care for him” [FCG 14].
Emotional and Psychological Distress
Anxiety, fear of complications, and witnessing the patient's suffering caused mental strain for FCGs and the entire family. One FCG narrated: Almost everyone in the family was worried about taking care of my father and being attentive to him. My mother worked very hard, she stayed up late caring for my father. She was mentally distressed, thinking about my father all night and cry, fearing that he might not be okay after such a major operation [FCG 7].
The FCGs expressed fear and concern about potential complications following surgery. One FCG affirmed, “Initially, he had severe pain and coughing, and we were worried that his wound stitches might open. We also felt fear, wondering what might happen next or if any issues would arise” [FCG 13/1].
Household Management and Routine Disruption
This subcategory reflects the difficulties of balancing home responsibilities with caregiving and managing children’ routine. One of the FCGs said: “it was difficult for my mother to manage household chores, took care of my father, and attending the guests” [FCG 7]. Similarly, another FCG mentioned, “We ladies face many difficulties as we have to do household chores while also addressing the needs of the patient” [FCG 8/1].
FCGs highlighted that providing continuous care substantially disturbed their routine. One FCG affirmed “During the initial ten days, we set aside our routine responsibilities and stayed awake continuously to care for the patient” [FCG 4/1]. FCGs expressed that their children's routines were also affected such as sleep, study, and play time. One FCG shared that she could not give proper time to children and due to this they became upset and mentally disturbed. My children became very upset, almost as if they had lost their mother. I felt very upset because I couldn’t give them any time. During my hospital stay, they missed me a lot and suffered significantly. For two months, I couldn’t give them proper time. Both of my children were mentally disturbed, and sometimes my daughter would sit alone and talk to herself [FCG 10].
Balancing Job and Caregiving Responsibilities
This subcategory derived from the difficulties balancing work and caregiving responsibilities. An FCG who was the patient's son, elucidated, “I prioritized my father's care over work. On the day of operation, I had a duty but requested rescheduling to be with my father till he was in the hospital. I returned to work after my father's discharge” [FCG 10]. FCGs handled multiple tasks at once, including their jobs, housework, and providing care. One FCGs narrated: I mostly took leave from work to help but it was not enough. Sometimes, I had to spend time at work and at home both. For instance, sometimes when I was at office and she [the patient] needed something, I had to rush back to fulfill her needs, or if a guest arrived, I had to take care of their needs too [FCG 8/1].
Financial Strain
Financial strain emerged from transportation cost, medical expenses, and the impact on employment when providing care to their loved ones.
Transportation Cost
FCGs faced financial difficulties during the caregiving period as they had to bear substantial expenses for transportation and follow-up visits to the hospital, reflected in one of the FCGs narration: Today we came, and the fare from Khushab [city of residence] to Islamabad is approximately Rs. 20,000, and on the day of discharge, it also costed us Rs. 20,000 and we must have to come back again after a month. The journey is quite long, and the OPD time is 8 o'clock, so we must leave home at 2 o'clock mid-night by car, the fare alone is unbearable rest other medicinal expenses [FCG 4/1].
Similarly, another FCG asserted: “We had to bear substantial expenses for transportation and related costs. Each visit for follow-up check-ups costs around Rs. 12,000 to 13,000, which included Rs. 10,000 for transport” [FCG 6].
Medical Expenses
This subcategory reflects the financial burden stemming from purchasing medication, and supplies like glucometer, nebulizer, or a bathroom commode chair for post-CABG care at home. One FCG illustrated: We had to buy a plastic chair for the bathroom, which was a struggle due to financial constraints. We also bought a blood pressure machine and a sugar testing machine ourselves. We incurred these expenses ourselves, and the cost of medicine added to it as well. We called the village doctor to check his blood pressure and sugar, and we had to pay him money for this. We could not arrange money to buy a machine for breathing support [Nebulizer], which costs around Rs. 6000 [FCG 4/1].
Impact on Employment
FCGs shared experiences of financial instability caused by caregiving responsibilities, which forced them to temporarily leave work or, in some cases, leave their jobs altogether. One FCG stated: “I am a laborer myself, and the patient's son is also a laborer, so we had to leave our jobs to come and help” [FCG 5]. Another FCG asserted, “My husband left his daily labor work and remained busy with caregiving and household management” [FCG 14].
Hospital and Healthcare Management Challenges
This category highlights the challenges FCGs face due to hospital and health care management issues.
Lack of Immediate Medical Support and Communication
FCGs expressed their difficulty in accessing specialized medical services due to nonavailability of cardiac hospital in vicinity. One FCG stated, “The main difficulty was that there is no cardiac hospital. If it were a 10-minute, 15-minute, or half-hour drive from home, it wouldn’t be as noticeable” [FCG 2]. Additionally, another FCG highlighted the importance of timely access for medical services. “We needed timely medical access and contact with doctors to avoid complications. The family felt the absence of immediate medical support and had to rely on hospital visits for every concern.”
Most FCGs highlighted that communication breakdown with the hospital made it difficult for families to comprehend the correct protocols for care at home, causing uncertainty and anxiety resulting in reliance on external sources. One FCG stated, “The hospital staff neither provided much information nor any source to contact them when needed at home. We had to ask people outside and consult medical persons we knew” [FCG 7].
Postoperative Follow-Up Visits
This subcategory emerged from difficulties faced by FCGs during follow up visits and their expressed need for technology-driven solutions. One FCG illustrated: The hospital has only one day nominated for post-operative follow-up visits. There should be a 24-h post-op follow-up visit schedule. Look, we have a nominated surgeon, and his follow-up visit day is only one day. If the patient visits on a different day, they are told it's not their follow-up day, and they should go back [FCG 15].
FCGs highlighted the importance of utilizing technology to reduce follow-up costs. One FCG illustrated: I believe that for those who reside in remote areas and cannot visit hospital for follow-ups, technology should be utilized. Many people like us travel long distances to visit the hospital, and you know it's an era of inflation, and things are very expensive. It becomes difficult to come to the hospital for minor issues. The doctor just needs to send a voice message, it doesn't cost much. [FCG 15].
Family Support
This category emphasized the critical role that families play in providing direct physical care, emotional support, and help with household management and finances.
Direct Caregiving and Emotional Support
FCGs stated that providing patients with emotional and physical support was made possible by their family working together. One FCG shared: “At my home, there are two brothers, our mother, my wife, and my sister-in-law. Everyone worked together to take care of him” [FCG2]. Another FCG affirmed: “My mother and my wife helped me in lifting and seating him [the patient]. My mother prepared food and stayed awake with me. Besides that, she helped in taking him to the washroom and bathing” [FCG4/1].
FCGs emphasized that despite their limited financial means, family's emotional support was crucial in giving them stability and fortitude to get through the difficult circumstances. One FCG stated, “My nephews and other relatives came and provided emotional support, especially in the challenging scenario of scarce resources” [FCG2]. Similarly, another FCG asserted, “My family provided emotional support, but they themselves were not able to offer financial help” [FCG3].
Household Management Support
FCGs emphasized the value of a joint family system, appreciating the shared support in managing household tasks. One of the FCGs reflected: “our combined family system played a significant role like nephews, cousins, and female relatives supported the housewives in household management tasks, such as cooking or looking after children” [FCG8/1]. Another FCG asserted, “All family members including my sister, my brother-in-law, and my brother managed household matters and ensured everything was handled properly in my absence” [FCG 5].
Financial Support
Financial support from family members was significantly vital for managing medical expenses, particularly when resources were insufficient. One FCG stated, “My brother is concerned and sends money for expenses but can't come himself due to his job” [FCG 4/1]. Moreover, one FCG who was the wife of the patient asserted, “My brother-in-law has been particularly helpful, continuing to provide financial assistance. My father gave me Rs. 10,000, and my brother also provided money” [FCG 11].
Discussion
This study explored the challenges faced by FCGs in providing post-CABG care at home after discharge from a public hospital in Pakistan. The findings reflect caregiving patterns characteristic of South Asian societies, where caregiving is culturally embedded within familial obligations (Pharr et al., 2014). Consistent with studies from India and Bangladesh, caregiving roles were distributed among spouses, children, and extended family members, reinforcing the collectivist model of care (Victor et al., 2018). Variation in educational backgrounds influenced FCGs’ health literacy and caregiving capacity, echoing patterns reported in other LMICs (Yuen et al., 2018). Despite socioeconomic hardship, the prevalence of joint family systems offered shared caregiving responsibilities, highlighting the importance of engaging families in discharge planning and follow-up care to optimize recovery after CABG (Yeung et al., 2018).
Several challenges identified including inadequate preparation for caregiving, physical and emotional strain, financial hardship, and systemic healthcare limitations. The lack of adequate preparation was the most prominent concern, leaving caregivers uncertain about managing postoperative tasks at home. Similar findings across LMICs reveal that nonprofessional caregivers often experience anxiety and distress due to insufficient knowledge and support (Halm, 2016; Knoll & Johnson, 2000). Evidence from Bangladesh, India, and Iran emphasizes the value of structured, nurse-led predischarge education in improving caregiver confidence and competence (Bjornnes et al., 2019; Chudgar et al., 2022; Depari et al., 2024). When FCGs receive structured training, they demonstrate improved caregiving capacity, fewer complications, and reduced readmissions (Ahlawat et al., 2025; Akbari & Celik, 2015; Kaur et al., 2022; Liu et al., 2019). These insights emphasize the need to integrate systematic caregiver education into discharge planning within resource-limited healthcare systems such as Pakistan's.
Physical and emotional exhaustion was another significant challenge. Many FCGs reported sleep deprivation and psychological distress resulting from continuous caregiving combined with domestic responsibilities. Similar reports from LMICs reveal that role overload and emotional strain often lead to caregiver burnout and diminished well-being (Halm, 2016; Hussain et al., 2018). Interventions that include psychosocial and emotional support have been shown to strengthen caregivers’ resilience and sustain caregiving performance (Lenz & Perkins, 2000; Solorzano et al., 2021). Strengthening psychosocial support for caregivers, either through counseling or peer-support programs, could therefore be a vital component of postdischarge care.
Financial strain was particularly evident among low-income and rural families, where out-of-pocket expenses for medications, wound care supplies, and travel for follow-up visits exacerbated the caregiving burden. Similar barriers have been documented in India and Bangladesh, where uncovered medical costs and travel expenses impede continuity of care (Bahrami et al., 2014; Blair et al., 2014; Kim et al., 2020). In this context, telehealth and community outreach interventions offer cost-effective alternatives to improve follow-up care and minimize financial strain (Kvedar et al., 2014; Malik et al., 2024; Noor Hanita et al., 2022; Vaid et al., 2023). Expanding such digital health initiatives in Pakistan could enhance continuity of care and reduce the inequities faced by rural caregivers.
System-level limitations, including poor communication, workforce shortages, and overburdened nursing staff, further exacerbated FCGs’ challenges. These issues mirror the realities of many LMICs, where limited transitional care frameworks strain both families and healthcare systems (Muhammad et al., 2023). Training and involving FCGs as active partners in postdischarge care may help mitigate these systemic gaps. Evidence from similar contexts indicates that caregiver engagement improves continuity of care and reduces readmission rates (Nigolian & Miller, 2011). Thus, empowering caregivers can be a cost-effective strategy to strengthen family-centered care and alleviate system pressures in resource-limited settings.
Despite these challenges, the findings also revealed a notable strength: the collective nature of caregiving in Pakistani families. Unlike reports from Western and some Asian contexts, where caregivers often experience isolation (Bangerter et al., 2018; Chi et al., 2018; McIlfatrick et al., 2018), Pakistani FCGs benefited from shared emotional and logistical support within the family unit (Moazam, 2000). However, in the absence of structured caregiver training, even strong familial support may not prevent preventable complications. Therefore, culturally appropriate, nurse-led, family-centered interventions are essential to enhance caregiver competence and sustain optimal post-CABG outcomes.
Strengths and Limitations
The qualitative design provided in-depth insights into the challenges faced by FCGs of post-CABG patients in home care settings, capturing rich, context-specific narratives often absent in quantitative studies. Another key strength is the inclusion of a socioeconomically and ethnically diverse participant group reflecting Pakistan's caregiving dynamics. Additionally, its focus on cultural influences provided novel insights into caregiving in LMICs.
Limitations include single-site recruitment from a public hospital, which may not fully represent the experiences of FCGs from private hospitals, and the cultural specificity of caregiving practices in Pakistan, which may limit generalizability to other settings. Lack of longitudinal data also restricts understanding of how challenges evolve beyond the 3-month postoperative period. As this was an exploratory descriptive study, we included patients with various comorbidities (e.g., diabetes), which may have influenced the nature and extent of caregiver burden. Future research should include FCGs from private hospitals and diverse cultural contexts to enhance transferability and examine how specific comorbid conditions shape caregiving experiences.
Implications for Practice
The findings highlight an urgent need for nurse-led, multi-level interventions to enhance support for FCGs of post-CABG patients. This includes conducting culturally adapted, hands-on predischarge workshops in Urdu on wound care, medication management, and mobilization techniques. Nurses can also integrate FCGs into care planning during hospitalization to clarify expectations and build their confidence. Postdischarge, nurses can moderate hospital-run WhatsApp groups to offer real-time guidance on diet, symptom monitoring, and emergency response. Nurses can further facilitate peer support networks by connecting FCGs with trained caregiving volunteers. At a broader level, nursing advocacy is essential for policies that subsidize transportation and medication costs, and expand telehealth access to ease follow-up burdens, particularly for rural families.
Conclusion
The FCGs of post-CABG patients in Pakistan face significant informational, emotional, physical, and financial challenges worsened by gaps in the healthcare system. Nurses play an important role in addressing these challenges through structured predischarge education, ongoing postdischarge support including digital follow-ups, and culturally appropriate, family-centered interventions. Nurse leaders and policymakers should prioritize the development and implementation of Nurse-led initiatives to empower FCGs, enhance patient recovery, and strengthen cardiac rehabilitation programs nationwide.
Supplemental Material
sj-docx-1-son-10.1177_23779608251408908 - Supplemental material for Post-CABG Care at Home: A Qualitative Study of Family Caregiver Challenges in a Resource Limited Context
Supplemental material, sj-docx-1-son-10.1177_23779608251408908 for Post-CABG Care at Home: A Qualitative Study of Family Caregiver Challenges in a Resource Limited Context by Farhana Parveen, Kainat Asmat, Khalil Ahmed Jatt and Asghar Khan in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608251408908 - Supplemental material for Post-CABG Care at Home: A Qualitative Study of Family Caregiver Challenges in a Resource Limited Context
Supplemental material, sj-docx-2-son-10.1177_23779608251408908 for Post-CABG Care at Home: A Qualitative Study of Family Caregiver Challenges in a Resource Limited Context by Farhana Parveen, Kainat Asmat, Khalil Ahmed Jatt and Asghar Khan in SAGE Open Nursing
Footnotes
Acknowledgments
The authors sincerely acknowledge the hospital administration for their support in facilitating study activities within the hospital. A heartfelt appreciation is also extended to all the participants who generously shared their time and experiences, making this study possible.
Ethical Approval and Informed Consent Statements
Ethical approval was obtained from the Institutional Review Board and Ethics Committee of Shifa Tameer e Millat University (IRB 157-24) and the Ethics Review Board of the study hospital (ERB 1279/2024). Written informed consent was obtained from all the participants prior to their enrollment in this study.
Authors contributions
Farhana Parveen: conceptualization, design, data collection, analysis, drafting, and editing of the manuscript. Kainat Asmat: supervision in design, methods and processes of the study, and critical review and final approval of manuscript. Khalil Ahmed Jatt: supervision in design, methods and processes of the study, and critical review and final approval of manuscript. Asghar Khan: supervision in design, methods, and processes of the study and critical review and final approval of manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data gathered and analyzed during this study will be available from the corresponding author upon reasonable request, ensuring compliance with the ethical guidelines and confidentiality requirements.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.