
Abstract
Introduction
Workplace stress and burnout may influence nurses’ physical and emotional well-being, which can impact the quality of care patients receive and their overall satisfaction with their hospitalization.
Objectives
The objectives of the study were to evaluate whether there are significant statistical relationships between nurses’ perceived stress, frequency of stressors, mindfulness, emotional self-regulation, self-care habits, and patient satisfaction scores.
Methods
The study took place over the course of 4 weeks. In this study, 340 nurse participants were surveyed using cross-sectional voluntary sampling design. The survey included previously developed and validated instruments. SAS v. 9.4 was used for statistical analysis.
Results
Significant differences were noted in average patient satisfaction scores by perceived stress; major nursing units in the Death and Dying, Conflict with Physicians, Lack of Support, and Work Load subscales of the Nursing Stress Scale; and major nursing units and dispositional mindfulness.
Conclusions
Hospital administrators can use this information in their organizations and set priorities and tailor mindfulness-based stress-reduction interventions for nursing professionals.
Keywords
Introduction
Nurse stress and burnout have a direct impact on patient care and satisfaction. Stress impairs an individual’s ability to provide attuned communication and empathy and their ability to be in the present moment (mindfulness). Research has shown an inverse relationship between perceived stress and mindfulness (Atanes et al., 2015) and has also suggested that one’s ability to regulate emotions (emotional self-regulation) and practice healthy self-care habits is a factor that potentially may impact stress responses (Kozlowski, Hutchinson, Hurley, Rowley, & Sutherland, 2017; Salovey, Bedell, Detweiler, & Mayer, 1999; Sapolsky, 2007). This study aligns with the growing body of evidence in this field and adds additional insights into the experience of nursing professionals.
Review of Literature
The health of a hospital organization is directly proportional to the health of its doctors, nurses, and administrators. Stress, burnout, fatigue, and psychological distress impact the quality of health care an institution is able to provide. If the health-care organization does not attend to the health of those who provide care, then the provision of exceptional patient-centered, high-quality health care is sure to suffer (Salyers et al., 2017).
To understand the connection between burnout and patient care, a 2011 study by the University of Pennsylvania School of Nursing examined data from surveys of 95,499 nurses’ working conditions and data from both the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey and American Hospital Association Annual Survey of Hospitals. Their findings revealed that of the nurses who were satisfied with their salaries and benefits, those with better work environments had higher (in some cases twice as high) employee satisfaction scores than those in hospitals with poor work environments. Furthermore, this study revealed a statistically significant correlation among nurse burnout, job satisfaction, and patient satisfaction. It went on to report that “the percentage of patients who would definitely recommend the hospital to friends or family decreased by about two percent for every ten percent of nurses at the hospital reporting dissatisfaction with their job,” even after controlling for other variables (McHugh, Kutney-Lee, Cimiotti, Sloane, & Aiken, 2011, p. 5).
While health-care providers may be technically accurate in the care they provide, it is how the patient feels about the care received that leaves the lasting impression from which they fill out patient satisfaction surveys (Leiter, Harvie, & Frizzell, 1998). In fact, Vahey, Aiken, Sloane, Clarke, and Vargas (2004) stated that patients cared for on units that nurses characterized as having adequate staff, good administrative support for nursing care, and good relationships between doctors and nurses were more than twice as likely as other patients to report high satisfaction with their care, and their nurses reported significantly lower burnout. (p. 1)
Furthermore, employees’ mental well-being is costly to an organization, both in terms of dollars spent and employee productivity. The International Labor Organization estimates that 30% of all work-related ailments are due to stress (Mino, Babazono, Tsuda, & Yasuda, 2006). It is approximated that in the United States, stress-induced disorders amounted to a loss of $6.6 billion (Bertolini, 2015). In large-scale studies, employees with self-reported higher levels of stress were found to have significantly increased annualized medical expenditures (approximately 45%–46% higher) compared with those with lower stress levels (Goetzel et al., 1998).
Stress impairs an individual’s ability to provide attuned communication and empathy, which impacts relationships (Siegel, 2007), and results in diminished attention, increased distraction, increase in reaction time, and deficits in an individual’s working memory (Driskell & Salas, 1996). Stress also hinders an individual’s ability to be in the present moment (mindfulness). Mindfulness is a mechanism by which an individual becomes aware of his or her own internal responses to external stimuli. Research has shown an inverse relationship between perceived stress and mindfulness (Atanes et al., 2015) and has suggested that one’s ability to regulate emotions (emotional self-regulation) is a factor that may potentially impact stress responses (Kozlowski et al., 2017; Salovey et al., 1999; Sapolsky, 2007). Emotional self-regulation can be thought of in terms of cognitive reappraisal and emotional suppressive tendencies. Eftekhari, Zoellner, and Vigil (2009) defined cognitive reappraisal, simply put, as a form of cognitive change in which one thinks about the situation in a manner such that one does not respond emotionally. Emotional suppression, on the other hand, is defined as the conscious inhibition of emotional expressive behavior while emotionally aroused and is often associated with negative consequences (Eftekhari et al., 2009; Gross & Levenson, 1993).
Stress may also have a bidirectional impact on self-care habits. Self-care refers to taking care of oneself mentally, physically, emotionally, or spiritually, and self-care habits may be considered a form of stress prevention and stress management (Bauer, 2016). Chronic stress can be detrimental for individuals across all aspects of their lives, and for nurses, healthy self-care habits can help balance personal and professional demands and increase mental well-being.
Optimistically, a substantial amount of research has shown that mindfulness-based interventions can improve various outcomes (e.g., stress, mindfulness, anxiety, or resiliency) in clinical providers (Gauthier, Meyer, Grefe, & Gold, 2015; Kemper, 2017; Kemper & Khirallah, 2015; Ratanasiripong, Park, Ratanasiripong, & Kathalae, 2015; Sood, Prasad, Schroeder, & Varkey, 2011; Warnecke, Quinn, Ogden, Towle, & Nelson, 2011). These interventions focus on purposely paying attention, being in the present, and being nonjudgmental. The interventions can include activities, such as breathing exercise, guided imagery, relaxation methods, yoga, or desensitization-relaxation in person or through virtual modalities. (Gilmartin et al., 2017).
As levels of stress continue to rise in America (Bethune & Lewan, 2017), there is an increasing demand for hospitals to address factors contributing to stress of its employees, as well as provide effective solutions at an organizational level. To do that, a better understanding of the experiences and needs of registered nurses (RNs) is needed. We conducted a cross-sectional, correlational survey study to examine the frequency of stressors affecting nurses and the relationships among dispositional mindfulness, perceived stress, emotional self-regulation, self-care habits, and patient satisfaction scores.
The primary objectives of this study were to evaluate and quantify nurses’
sources and frequency of work-related stressors; correlations between the frequency of stressors, dispositional mindfulness, emotional self-regulation, and self-care habits; relationships between nurses’ perceived stress levels, age, years in nursing practice, dispositional mindfulness, emotional self-regulation, self-care, frequency of stressors, and HCAHPS scores; and relationships between major nursing units; and nurses’ age, years in nursing practice, dispositional mindfulness, emotional self-regulation, self-care, frequency of stressors, and HCAHPS scores.
Based on previous research, we hypothesized that there would be significant statistical relationships between nurses’ perceived stress, frequency of stressors, mindfulness, emotional self-regulation, self-care habits, and patient satisfaction scores. We also believed that there may be variations of these factors depending on the nurses’ medical unit and years of practice experience.
Methods
Study Design and Institutional Review Board
The study design used was a correlational, cross-sectional survey of RNs at a tertiary care medical center. The study protocol was reviewed and approved by the Aspire Institutional Review Board (Protocol 020.NUR.2017.D). The survey was disseminated over a 4-week period (July 19–August 16, 2017) via an e-mailed link from the study principal investigator. Qualtrics, a secure online survey platform, was used to collect survey responses anonymously. The link directed respondents to the survey with an informed consent front page. At the bottom of the informed consent page was a button to select indicating their willingness to participate, which once clicked, respondents were The informed consent page included an option for respondents to indicate their willingness to participate. Once they selected the option to participate, they were forwarded to the survey. The nurses’ survey instrument contained a variety of multiple choice, Likert-style, and free-text response option questions.
Sample and Inclusion/Exclusion Criteria
The survey was disseminated to 958 RNs in all Methodist Dallas Medical Center (MDMC) departments/units, including Medical-Surgical (Oncology/General Medicine, Neuro/Ortho, Telemetry, General Surgery/Telemetry, Nephrology, General Medicine/Surgery); Women’s and Children’s (Labor and Delivery, General Nursery/Postpartum Care, Neonatal Intensive Care Unit); Adult Critical Care (Intensive Care Unit, Neuro Critical Care Unit [NCCU]); Emergency Department (ED); Gastroenterology (GI) Lab; [Golden Cross] Academic Clinic; Interventional Radiology, Cardiology, Nursing Administration, Surgical Services (Operating Room [OR], Post Anesthesia Care Unit [PACU], Post Discharge Unit [PDU], Same Day Admit [SDA]); and other, not listed departments/units. RNs included direct-care nurses, nurse managers, nursing clinical coordinators, and directors/administrators. Study participants had to be (a) age 18 years or older, (b) be a current licensed RN practicing at MDMC during the survey period, (c) literate in English, and (d) able and willing to provide consent. A total of 340 RNs participated in the study.
Research Questions/Survey Tools
Demographic information was collected, including gender, age, educational level, and nursing unit. The survey included previously developed questions and validated, reliable instruments, which were all publicly available for use. Those included the following:
Perceived stress, also described as brain/emotional state (Mellin, 2011), was ascertained by asking respondents the single question “Which emotional/mental state do you most frequently find yourself in?” Options were 1 (feeling great!), 2 (feeling good), 3 (a little stressed), 4 (definitely stressed), and 5 (stressed out!). The Nursing Stress Scale (NSS) is a 34-item instrument that measures the frequency of situations that have been identified as causing stress for nurses on the job (Gray-Toft & Anderson, 1981). It is a validated and reliable tool that provides a total stress score as well as scores on seven subscales, which include the following: Death and Dying, Conflict with Physicians, Inadequate Preparation, Lack of Support, Conflict with Other Nurses, Work Load, and Uncertainty Concerning Treatment. Gray-Toft and Anderson (1981) used two estimates of the reliability: test–retest and internal consistency. The coefficient for test–retest for the total scale was 0.81. Four measures of internal consistency were obtained: a Spearman–Brown coefficient of .79, a Guttman split-half coefficient of .79, a coefficient of .89, and a standardized item α of .89. All four measures indicated a satisfactory level of consistency among items (Gray-Toft & Anderson, 1981). The NSS inquires how often respondents find the situations presented to be stressful. An example situation presented on the scale is “Not enough staff to adequately cover the unit.” Response categories were 0 (never), 1 (occasionally), 2 (frequently), and 3 (very frequently). The total NSS score was calculated by taking the average of all 34 items. Average subscale scores were also calculated. Mindfulness as it pertains to everyday experiences was analyzed using the Mindful Attention Awareness Scale (MAAS; Brown & Ryan, 2003). The MAAS is a validated and well-established scale that measures dispositional mindfulness. MacKillop and Anderson (2007) provided an analysis of the validity and internal reliability (Cronbach’s α indicated good internal reliability, α = .89) of the MAAS (MacKillop & Anderson, 2007). Fifteen statements about everyday experiences are presented and ranked by respondents based on how frequently or infrequently they have the experiences. An example statement is “I rush through activities without being really attentive to them.” Respondents ranked each statement on a 6-point Likert-type scale ranging from 1 (almost always) to 6 (almost never). To score the scale, the average of the 15 items was computed; therefore, the final scores could range from 1 to 6. Higher scores reflect higher levels of dispositional mindfulness. Emotional self-regulation was analyzed using the Emotion Regulation Questionnaire (ERQ) (Gross – John, 2003). The validity and internal reliability of the ERQ has been studied extensively, revealing several associations with constructs related to adaptive and nonadaptive functioning (Ioannidis & Siegling, 2015). The ERQ is a 10-item scale designed to measure respondents’ propensity to adjust their emotions in two facets: (a) cognitive reappraisal (ERQ_CR) and (b) expressive suppression (ERQ_ES). Respondents answered each item on the ERQ along a 7-point Likert-type scale ranging from 1 (strongly disagree) to 7 (strongly agree). Each facet’s scoring was kept separate. Higher scores on the cognitive reappraisal facet and lower scores on the emotional suppression facet may correlate to greater well-being (Eftekhari et al., 2009). An example statement on ERQ_CR facet is “When I want to feel more positive emotions (such as joy or amusement), I change what I’m thinking about.” An example from the ERQ_ES facet is “I control my emotions by not expressing them.” Self-care habits were measured using the Self-Care Quiz (SCQ). This quiz was developed by Oregon State University’s Academic Success Center (Oregon State University, 2017). The 18-item quiz is designed to measure how well respondents take care of themselves related to factors such as sleep, exercise, social support, time management, and well-being. Each item on the SCQ is answered along a 5-point Likert-type scale ranging from (5) more true to (1) less true. An example statement is “I exercise at least 5 days a week for 30 minutes.” Scoring was kept continuous and ranged from 18 to 90. Self-care habit scores were categorized as poor (18–35), fair (36–53), good (54–71), and excellent (72–90). HCAHPS overall satisfaction scores were abstracted from Press Ganey (2018) for the 6 months immediately preceding the survey period (January to June 2017). The scores were averaged per unit based on the percent of patients ranking the hospital between 9 and 10. This data was only available for Medical-Surgical, Adult Critical Care, Women’s and Children’s (General Nursery/Postpartum Care only), and ED units.
Statistical Analysis
Descriptive statistics are reported as absolute frequencies (n), mean ± standard deviation, and median (range) for continuous variables and as absolute (n) and relative frequencies (%) for categorical variables. Continuous variables included age, years in nursing practice, MAAS, ERQ_CR, ERQ_ES, SCQ, NSS, and HCAHPS, which were evaluated for normality. Categorical variables included sex, education level, nursing unit, and perceived stress. Relational concepts were evaluated by calculating Pearson’s correlation coefficients between MAAS, ERQ_CR, ERQ_ES, SCQ, NSS scales, and years on the job. Depending on whether the independent variables were normally distributed, parametric analysis of variance (ANOVA) or nonparametric Kruskal–Wallis tests were used to evaluate group differences between dependent variables (i.e., perceived stress, major nursing units). Significance was defined as p < .05. All analyses were conducted using SAS v. 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Descriptive and significant findings of the survey are presented later.
Sample Characteristics
Descriptive Statistics.
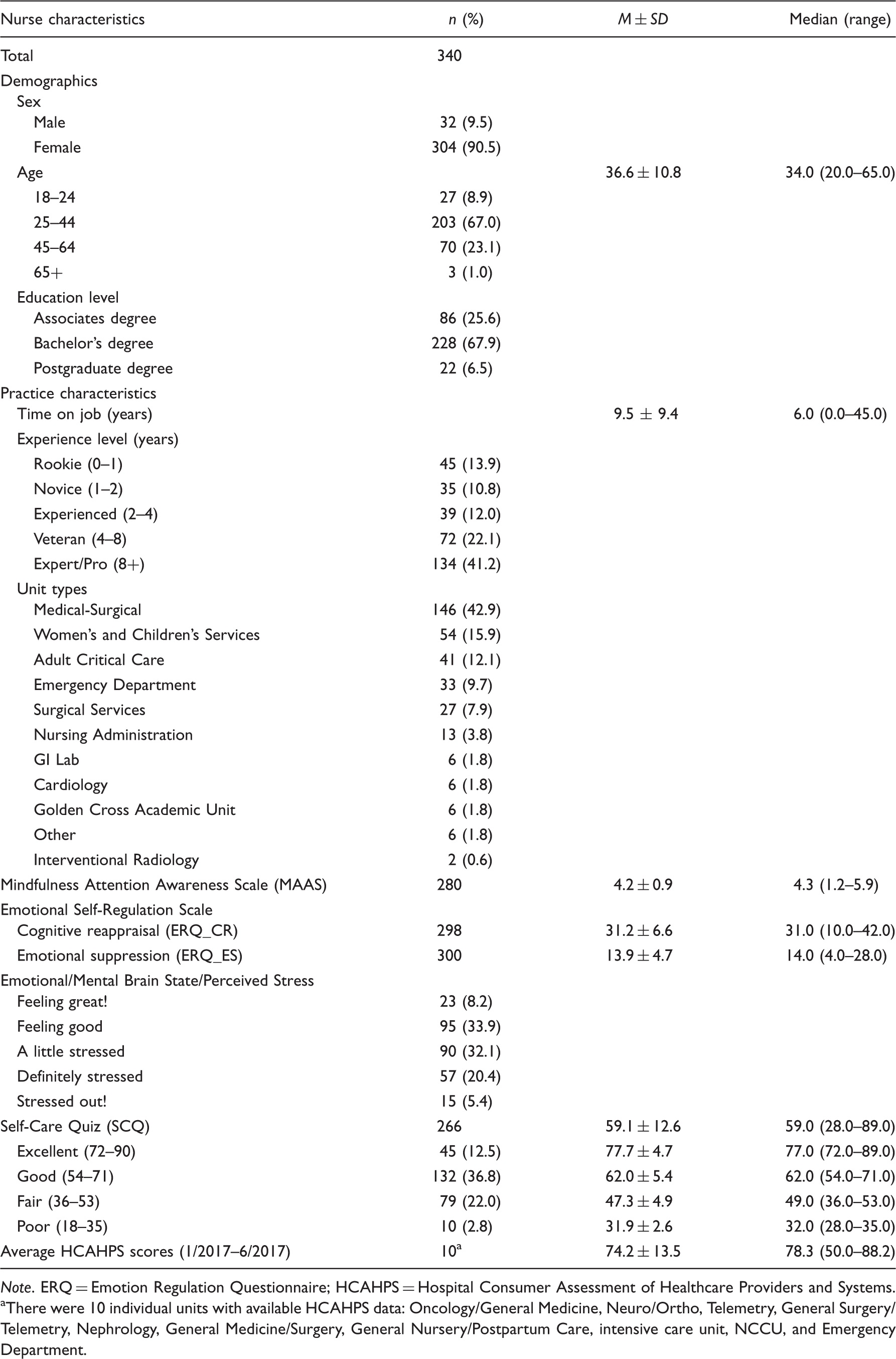
Note. ERQ = Emotion Regulation Questionnaire; HCAHPS = Hospital Consumer Assessment of Healthcare Providers and Systems.
aThere were 10 individual units with available HCAHPS data: Oncology/General Medicine, Neuro/Ortho, Telemetry, General Surgery/Telemetry, Nephrology, General Medicine/Surgery, General Nursery/Postpartum Care, intensive care unit, NCCU, and Emergency Department.
Nurse Characteristics by Hospital Unit.

Note. Statistically significant differences (i.e. p <.05) are bolded. ANOVA = analysis of variance; ED = Emergency Department; MAAS = Mindful Attention Awareness Scale; ERQ = Emotion Regulation Questionnaire; CR = cognitive reappraisal; ES = expressive suppression; SCQ = Self-Care Quiz; NSS = Nursing Stress Scale; HCAHPS = Hospital Consumer Assessment of Healthcare Providers and Systems.
aData only available for the following units: Medical-Surgical (Oncology/General Medicine, Neuro/Ortho, Telemetry, General Surgery/Telemetry, Nephrology, General Medicine/Surgery); Adult Critical Care (intensive care unit, NCCU); Women’s and Children’s (General Nursery/Postpartum Care); and the Emergency Department.
Research Question Results
Perceived Stress (Emotional/Brain State)
Nurse Characteristics by Perceived Stress Level.
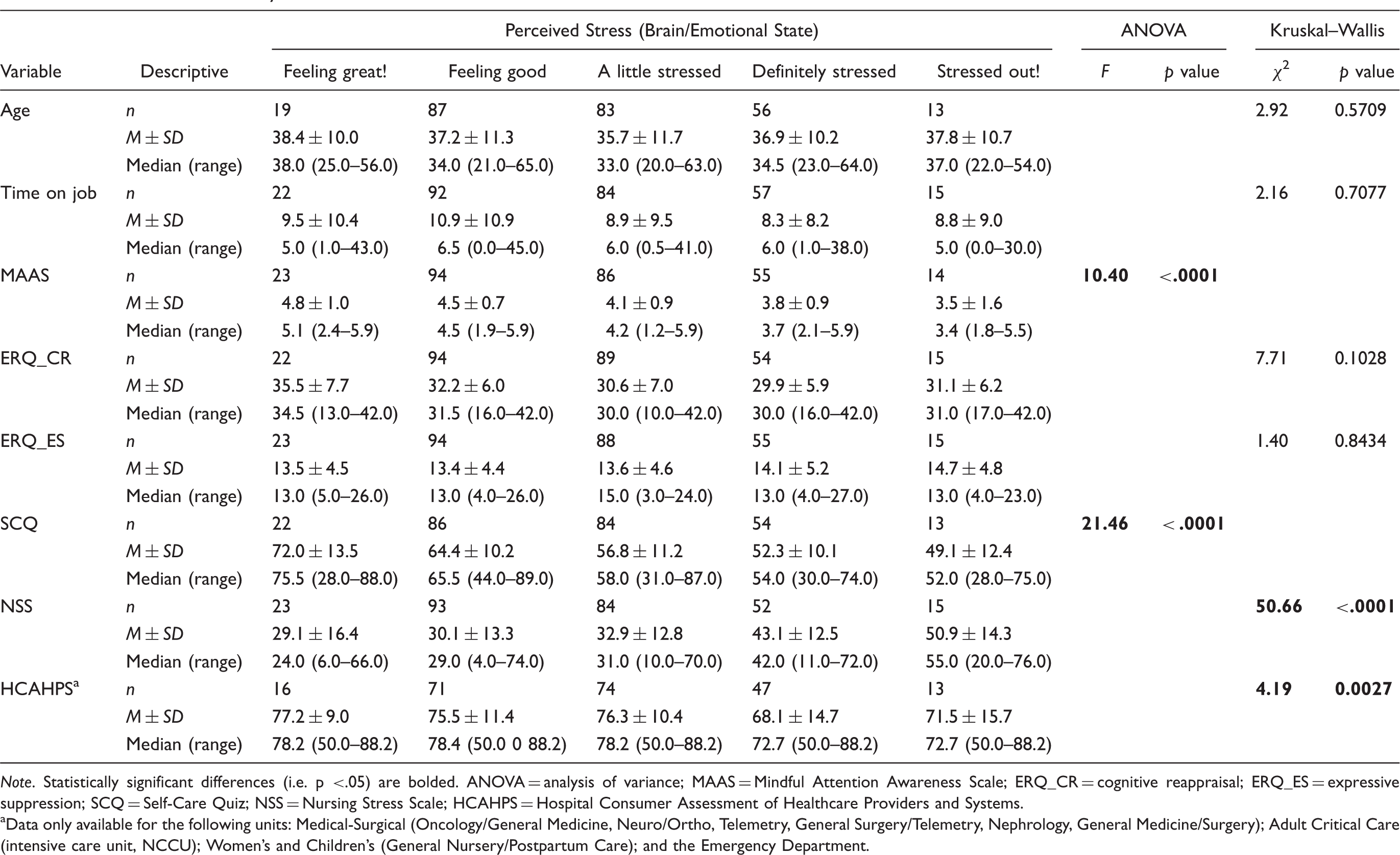
Note. Statistically significant differences (i.e. p <.05) are bolded. ANOVA = analysis of variance; MAAS = Mindful Attention Awareness Scale; ERQ_CR = cognitive reappraisal; ERQ_ES = expressive suppression; SCQ = Self-Care Quiz; NSS = Nursing Stress Scale; HCAHPS = Hospital Consumer Assessment of Healthcare Providers and Systems.
aData only available for the following units: Medical-Surgical (Oncology/General Medicine, Neuro/Ortho, Telemetry, General Surgery/Telemetry, Nephrology, General Medicine/Surgery); Adult Critical Care (intensive care unit, NCCU); Women’s and Children’s (General Nursery/Postpartum Care); and the Emergency Department.
NSS
Nursing Stress Scale (NSS) and Subscale Results.

Note. Respondents were asked how often they found the situations presented in the NSS to be stressful. Respondents answered each question on 4-point Likert scale where 0 = never, 1 = occasionally, 2 = frequently, and 3 = very frequently.
NSS Subscales by Major Nursing Units.
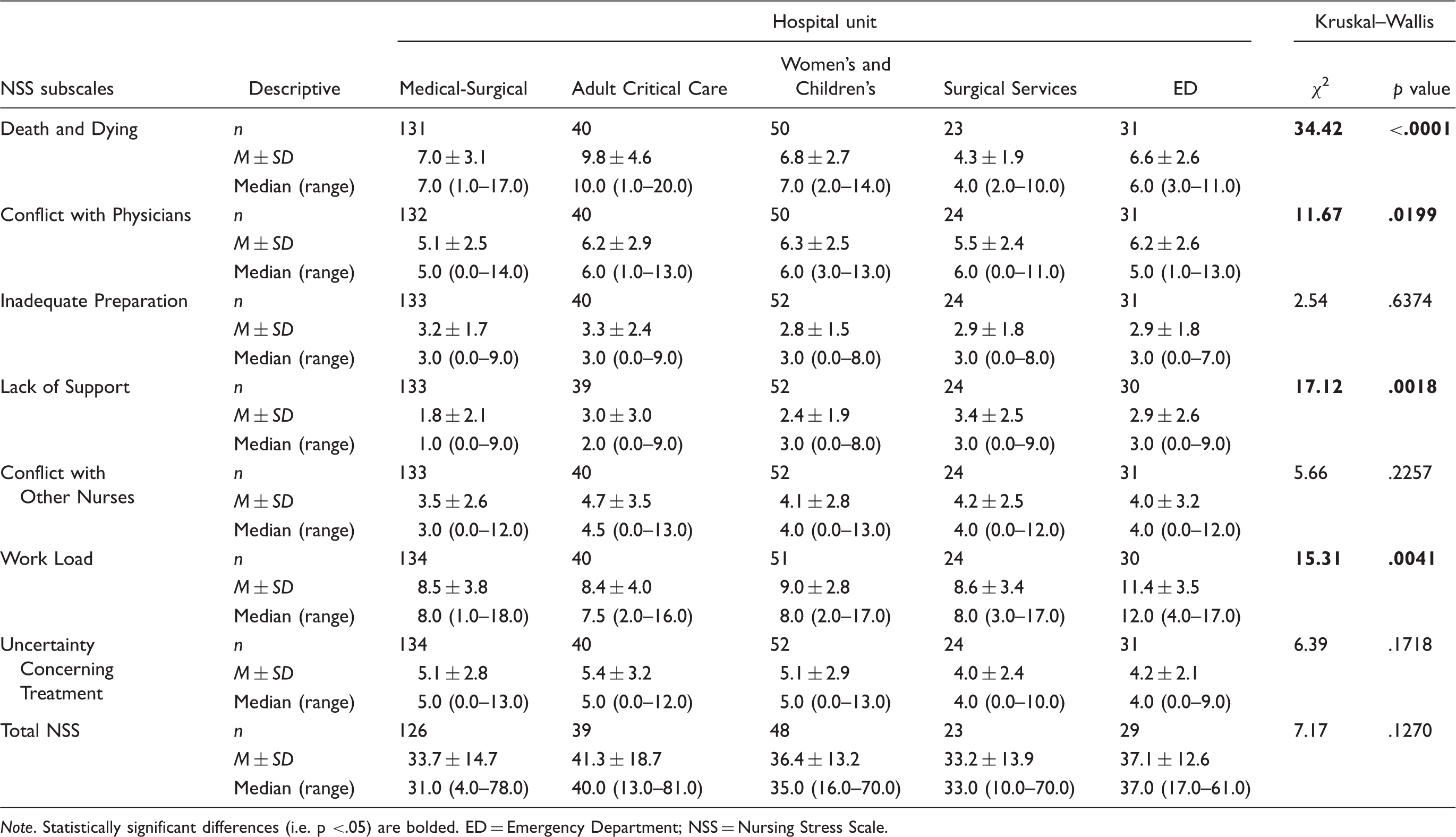
Note. Statistically significant differences (i.e. p <.05) are bolded. ED = Emergency Department; NSS = Nursing Stress Scale.
Pearson’s Correlations of Dispositional Mindfulness (MAAS), Cognitive Reappraisal (ERQ_CR), Emotional Suppression (ERQ_ES), Self-Care (SCQ), Nursing Stress Survey (NSS) Scales, and Years on Job.

Note. Statistically significant differences (i.e. p <.05) are bolded.
Although there was not a significant correlation between years in practice and NSS scores, we investigated if there was a relationship between expertise levels and NSS using a nonparametric one-way of ANOVA test (not shown). Here, we found that nurses at the novice expertise level (1–2 years’ experience) had higher NSS stress scores as compared with those in the experienced group (2–4 years), χ2(4, 262) = 9.51, p = .0496.
Mindfulness Attention Awareness Scale (MAAS)
Higher scores on the MAAS indicate greater dispositional mindfulness. The mean mindfulness score was 4.2 ± 0.9. The instrument has a potential range between 1 and 6. Mindfulness scores exhibited a very weak, negative correlation with the ERQ_ES (r = −.13423, p = .0258); a weak, negative correlation with total NSS scores (r = −.30985, p < .0001); and a moderate, positive correlation with SCQ (r = .45313, p < .0001; Table 6). There were differences between major nursing units and dispositional mindfulness: Medical-Surgical units had the highest mean scores (4.5 ± 0.9), and Adult Critical Care units had the lowest (3.8 ± 0.9), F(4,242) = 3.58, p = .0074 (Table 2).
Emotional Self-Regulation Questionnaire (ERQ)
Higher scores on the cognitive reappraisal facet and lower scores on the emotional suppression facet could indicate greater mental well-being (Eftekhari et al., 2009). The mean score on the cognitive reappraisal facet of the ERQ was 31.2 ± 6.6 (this instrument facet has a potential range between 6 and 42), and the emotional suppression facet was 13.9 ± 4.7 (this instrument facet a potential range between 4 and 24; Table 1). ERQ_CR was weakly and positively associated with self-care habits (r = .20172, p = .0010; Table 3). ERQ_CR and ERQ_ES were not associated with perceived stress (Table 6).
SCQ
The majority of nurses ranked in the good (scores 54–71) and fair (36–53) categories for self-care habits (36.8% and 22.0%, respectively; Table 1). Significant correlations with other continuous scales and relationships with perceived stress are discussed earlier.
Discussion
This study contributes to the body of evidence that examines the relationships between perceived stress, mindfulness, emotional self-regulation, and self-care habits, in a population of RNs at a tertiary care medical center.
Mindfulness is defined as “… paying attention in a particular way: on purpose, in the present moment, and nonjudgmentally” (Kabat-Zinn, 1994, p. 4). The results of this study are in agreement with the substantial amount of research indicating converse relationships between perceived stress and mindfulness (Atanes et al., 2015; Black, Sussman, Johnson, & Milam, 2012; Branstrom, Duncan, & Moskowitz, 2011; Gard et al., 2012; Weinstein, Brown, & Ryan, 2009), the NSS and mindfulness (Gauthier et al., 2015), and perceived stress and self-care habits (McKinzie, Altamura, Burgoon, & Bishop, 2006).
Compared with other research studies using the NSS, the RNs in this study had a smaller degree of stress based on the total NSS stress scores (Gray-Toft & Anderson, 1981; Rolf, 1999). However, our results are reinforced by the fact that only 25.8% of nurses perceived themselves as being definitely stressed or stressed out. This reporting of lower levels of stress overall may be due to the inclusion of nondirect patient care nurses (i.e., directors/administrators, nursing clinical coordinators, and nurse managers) who do not encounter the situations presented in the NSS or do not find these situations to be stressful, or both. To protect anonymity in the survey, we did not ask nurses to identify their job title because we asked them to identify their unit. In addition, Chang et al. (2006) demonstrated that mental health scores were higher for nurses working more years in the unit. Nurses in our sample mostly fell into the experienced, veteran, and expert/pro levels (75.3%); therefore, one might conclude nurses reported less perceived stress and frequency of stressors because they were largely more experienced and acclimated to handling the demands of nursing.
Results of the NSS identified stressors that occurred most frequently for nurses. The highest stress situations were in the Work Load subscale, with factors that included breakdown of a computer, unpredictable staffing and scheduling, too many nonnursing tasks required, not enough time to provide emotional support to a patient, not enough time to complete all nursing tasks, and not enough staff to adequately cover the unit. Additional high-frequency stressors were in the Death and Dying subscale and included performing procedures that patients experience as painful and feeling helpless in the case of a patient who fails to improve. National and international studies using the NSS affirm these as common high-stress situations for nurses in a variety of settings (Cai, Li, & Zhang, 2008; Chang et al., 2006; Fathi, Nasae, & Thiangchanya, 2012; Gholamzadeh, Sharif, & Rad, 2011; A. Lambert & Lambert, 2008; V. Lambert, Lambert, & Ito, 2004).
We also discovered differences in the NSS subscales between units. Understandably, Adult Critical Care units reported the highest levels of stress related to Death and Dying considering these nurses are taking care of critically ill and often end-of-life patients. Nurses in the ED reported the highest stressors related to Work Load. It is important to note that in the months preceding the survey administration, the MDMC ED experienced high turnover among nursing staff which may have resulted in increased pressure and responsibilities for remaining staff and their subsequent feelings of higher stress.
Consider also that stressors related to Work Load and Death and Dying reflect factors often outside of nurses’ individual control. Individuals are only able to control their view of and responses to these stressors. Healthy practices of cognitive reappraisal and mindfulness techniques (such as mindfulness-based stress-reduction interventions) have been shown to benefit individuals and enable them to better respond to these stressors (Gilmartin et al., 2017; Irving, Dobkin, & Park, 2009). For example, mindfulness-based interventions have demonstrated that they have the ability to increase the clarity of values and ability to withstand exposure, to one’s capacity to sustain openness to unpleasant/pleasant dynamics, without becoming cut off from awareness of the present moment. This, in theory, leads to a more real and healthier experience, based on acceptance of reality rather than its suppression. (Atanes et al., 2015, p. 6)
Self-care habits are defined as “engagement in behaviors that maintain and promote physical and emotional well-being and may include factors such as sleep, exercise, use of social support, emotion regulation strategies, and mindfulness practice” (Myers et al., 2012, p. 56). Existing research has demonstrated a significant relationship between these self-care factors and stress (Brown & Ryan, 2003; Frank, Tong, Lobelo, Carrera, & Duperly, 2008; McKinzie et al., 2006; Moore, Zoellner, & Mollenholt, 2008; Munir & Jackson, 1997; Wright, Valdimarsdottir, Erblich, & Bovbjerg, 2007). We administered the SCQ to tease out self-care habits and found that perceived stress was significantly related to self-care habits, cognitive reappraisal tendencies, and mindfulness.
In examining how nurses’ stress relates to outcomes like patient satisfaction, we found that nurses who reported higher perceived stress belonged to units that, on average, had lower HCAHPS scores. This aligns with studies by McHugh et al. (2011) and Vahey et al. (2004) that illustrated relationships between patient satisfaction and nurse stress/burnout and job satisfaction. This underscores the importance of placing nurses’ emotional well-being high on a list of priorities for health-care organizations. Patient satisfaction data collected through HCAHPS are intended to “allow objective comparisons between hospitals, create incentives to improve care, and enhance accountability and increase transparency in the quality of health care provided with public money” (Geiger, 2012, p. 11). Centers for Medicare & Medicaid Services began tying Medicare reimbursements to HCAHPS scores in 2012, and by 2017, health-care organizations could gain or risk up to 2% of reimbursement dollars (Letourneau, 2016). Better performance on HCAHPS protects health-care organizations’ revenue.
Finally, we found differences between nursing units, age of nurses and years of experience, dispositional mindfulness, and HCAHPS scores. Scanning their nurse populations and implementing interventions with identified differences in mind will enable health-care organizations to rollout tailored stress-reduction interventions focused on the needs of nurses and their medical units. This approach increases any intervention’s chance of being effective.
Limitations
This study employed a cross-sectional, correlational design, which cannot imply causation between variables, and alternative interpretations of the data presented are plausible. Well-designed randomized control trials are needed to establish a causal link between nurses’ stress, mindfulness, and self-regulation levels and outcomes like patient satisfaction. In addition, the self-report nature of the study presents the potential for response bias in which participants may not answer questions truthfully. However, the survey was administered in an anonymous fashion to reduce potential response bias. Further, the fact this survey used a convenience sample and was administered to nurses at one facility introduces the potential for participation bias, in which respondents disproportionately possess certain traits that can affect the interpretation of results and impedes generalizability. Regardless, our data agree fundamentally with extensive existing research into the interplay of perceived stress, mindfulness, self-regulation, self-care habits, and patient satisfaction.
This analysis did not include a deep dive into individual unit-level differences. For the purpose of analysis, individual units were combined by type (e.g., Medical-Surgical, Women’s and Children’s, etc.). It is important to keep in mind that although similarities exist in the groupings of units, there may be inherent differences in the cultures of the individual units that make up these groups, which may increase or decrease perceived stress levels; the effects of which could disappear when those units are combined. In addition, nurses working on Medical-Surgical units were the largest group of respondents (42.9%). This could potentially skew our results and interpretations of unit type differences. Furthermore, HCAHPS surveys are not collected from every patient. This presents a potential bias in the interpretation of the interpretation of analyses involving unit-level HCHAPS scores.
Even though survey participants were assured of anonymity and no personally identified information was collected, self-report surveys typically carry the potential of social desirability bias. This is a type of response bias that drives respondents to answer questions in a way that makes them appear more favorable to the experimenter. The magnitude of stress reported on the NSS was of a lesser degree than other research studies using the NSS. However, the findings of the NSS measure were significantly consistent with nurses’ reported perceived stress and were related to years of nursing experience; therefore we are confident that the stress levels reported by our nursing population are an accurate representation of the true state of nurses at MDMC.
Implications for Practice
The interplay between stress, mindfulness, emotional self-regulation, and self-care habits, and outcomes like patient satisfaction, is presented herein and aligns with a substantial body of research available, with additional insights into nursing professionals and differences between types of nursing units. Hospital administrators can use this information or replicate the methods in their own organizations and set priorities and tailor mindfulness-based stress-reduction interventions for their own nursing professionals.
For example, nurses on units who report high-stress-related work load may feel overwhelmed by additional activities unrelated to their immediate job duties, even activities aimed at improving well-being and decreasing stress. Time commitment has been shown to be a common barrier for practice of mindfulness-interventions in health-care professions, so evidence-based interventions that are brief and easy to access would be best used in such environments to support uptake and effectiveness (Gilmartin et al., 2017). Nurses that report greater stressors related to death and dying may need stress-reduction interventions focused on coping mechanisms and emotional self-regulation, while nurses on units reporting interpersonal conflict or perceived lack of support may need interventions tailored to mindful-communication, empathy, and teamwork. Understanding the factors that drive why we do what we do, personally and professionally, supports the conception of root-cause solutions.
Conclusions
The health of a hospital organization is directly proportional to the health of its doctors, nurses, and administrators. Organizations that attend to the emotional well-being of their providers also enable the delivery of exceptional patient-centered, high-quality health care.
Footnotes
Acknowledgment
We thank Andrea Lee, BSN, RN for her role in helping to develop and dissiminate the survey to nurses at MDMC.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.