
Abstract
Introduction
Family violence (FV) is one of the most urgent health issues of our generation. While nurses play a vital role in identifying and supporting victim/survivors of violence, little is known about nursing readiness to respond across clinical areas.
Objective
This study aimed to compare and contrast the knowledge, confidence, clinical skills, and perceived barriers of nurses across three clinical areas of a tertiary trauma hospital in Melbourne, Australia, in responding to FV.
Method
A prospective, mixed methods design was used. The nursing staff at a large trauma hospital were approached to participate. Participants completed a brief online survey to quantify clinician-reported knowledge, clinical skills, and barriers to managing FV.
Results
Two hundred and forty-two nursing staff electronically completed a brief survey to capture self-reported confidence, knowledge, clinical skills, and barriers to working effectively in the area. The descriptive analysis reflected service-wide deficits in knowledge, confidence, and self-reported clinical skills, irrespective of the work area. Deficits were identified on a background of limited structured training for FV among this cohort. Significantly higher rates of FV confidence and knowledge were identified among emergency department nurses relative to acute and subacute clinical counterparts.
Conclusion
Nurse respondents overall reported low rates of confidence, knowledge, and clinical skills in responding to disclosures of FV. Findings reinforce the need for imbedded training programs to support frontline responses.
Keywords
Introduction
Family violence (FV) is one of the most urgent health issues of our generation and is at pandemic proportions. Worldwide, one in three women will experience violence at the hands of an intimate partner (World Health Organisation, 2018); with similar Australian estimates reported (Cox, 2016). FV refers to a range of violent and abusive behaviors including physical, emotional, psychological, and financial abuse. Underpinning this violence is a pattern of perpetrator behavior which seeks to control or dominate and cause fear in its recipient. While variable terminology is seen internationally, in the Australian state of Victoria, where this research is conducted, FV is the preferred term as it reflects the definition provided in the states Family Violence Protection Act (2008). Accordingly, FV has been defined as behavior directed toward a family member that is physically, sexually, emotionally, psychologically, or economically abusive or coercive and threatening in nature (Family Violence Protection Act, 2008). While FV transcends gender and sexual orientation, it is disproportionally perpetrated by men against women and children (Hamberger & Larsen, 2015). Exposure to FV conveys a high physical and psychological impact (Ayre et al., 2016) with significant public health implications.
Literature Review
In response to this overwhelming problem, frontline hospital clinicians have been identified as playing a vital role in identifying and appropriately responding to FV. In Australia, just under one-third of all assault presentations to the hospital were due to FV, with neck and head injuries commonly observed (AIHW, 2019). Ideally, hospitals should provide a safe environment for victim/survivors to confidentially disclose FV and receive a supportive response (García-Moreno et al., 2015). For many, contact with a hospital health professional may be the only opportunity they have to access supportive care. While many healthcare providers will encounter victim-survivors, a significant proportion of clients experiencing violence will go undetected due to failures in screening, and/or the existence of barriers to disclosure (Fisher et al., 2020; Reeves & Humphreys, 2018). Research shows that while more than half of all women who present to an emergency department have experienced FV at some point, only 5% are identified by healthcare workers (Ahmad et al., 2017; Hinsliff-Smith & McGarry, 2017). Moreover, health problems are commonly treated as a stand-alone issue, overlooking the interplay between chronic health presentations and FV (Ramsay et al., 2002). Despite the primary role hospitals have in responding to FV, there has been a slow evolution of health service system-wide transformational change in this area.
One of the most widely implemented interventions for FV in a healthcare setting over the last 15 years has been screening. While the efficacy of screening in isolation has not been reliably established (MacMillan et al., 2009; Ramsay et al., 2002), the importance of a hospital-wide response to facilitate the identification and management of violence has been highlighted (Hamberger et al., 2015; Royal Commission into Family Violence, 2016). Nurses are in a unique position to identify and support victim/survivors as they are often the first point of contact for a patient. They spend more time with patients than other consultant professional groups and play an important role in advocating for patient well-being and safety. Unsurprisingly, FV has increasingly become a clinical issue of high relevance to nurses (Bradbury-Jones, 2016). Despite this, recent data highlights the under-preparedness of nursing students (Beccaria et al., 2013) and practicing nurses (Sundborg et al., 2012) in responding to violence, with one-third of nurses shown to have no formal education in FV (Alshammari et al., 2018). A number of barriers have been identified by nurses in the screening and management of FV including language barriers, cultural differences, and low confidence in their clinical skills of enquiry (Alshammari et al., 2018).
With increasing recognition of the role of healthcare providers in responding to FV, several research studies have evaluated the effectiveness of educational interventions in improving readiness to respond. Alhalal (2020) reported improved knowledge and attitudes among a mixed sample of doctors and nurses following a one-off three-hour training program that focused on assessment and identification of violence, responding to disclosures and personal attitudes and beliefs. Importantly, however, the intervention did not significantly impact self-reported clinical practices. Brief training has also been reported to increase nurses’ knowledge and preparedness to undertake screening of violence (Baird et al., 2018) and reduce perceived barriers associated with screening (Arrab & Ibrahim, 2018). Collectively, while promising outcomes have been reported to support the effectiveness of training, overall, this body of literature is limited by heterogeneity in intervention content and failures to rigorously evaluate outcomes (Crombie et al., 2017). It is also important to note, that screening is just one component of a recommended best-practice health service response to the FV experiences of patients (World Health Organisation, 2013).
Despite the evolving evidence base about nursing preparedness as a whole, little is known about readiness to respond across distinct clinical areas. With the diversity of roles within nursing, there is a need to understand the relative knowledge, confidence, and skills in responding to FV in each clinical area. Doing so represents an essential first step in identifying relative areas of clinical weakness and adapting training to match the baseline skill sets of nurses across clinical areas.
The data reported in this study are part of a larger data set, with some results from this data set already published (Fisher et al., 2020; Rudd et al., 2021; Withiel et al., 2021). The overall study involved a whole-hospital staff survey of FV knowledge, confidence, and clinical skills, in a large metropolitan trauma hospital in Australia. The current paper presents the results from the sizeable nursing cohort from this data set, in detail. This study aimed to compare and contrast the knowledge, confidence, clinical skills, and perceived barriers in responding to FV among nurses across three clinical areas of the hospital: emergency department, acute inpatient units, and subacute wards.
Methods
Design, Materials and Setting
This cross-sectional study prospectively quantified clinician-reported knowledge, clinical skills, and barriers to managing FV in a large tertiary hospital in Australia. The Royal Melbourne Hospital is a metropolitan Level 1 adult trauma hospital with multiple divisions including emergency medicine, trauma, and rehabilitation. The local environment at the time of survey completion was characterized by an absence of FV policies or procedures to guide staff responses. There was also no FV training program available for clinicians, within the hospital.
As noted, overall results from this data set have been published elsewhere, together with accompanying details on the outcome measurement tool Fisher et al., 2020. Briefly, this questionnaire was designed to collect data on self-reported FV training, knowledge, and confidence together with estimated rates of screening and perceived barriers to safe FV practice. The survey contained a combination of Likert, categorical, and dichotomized items together with free-text response sections (see Supplementary File 1). Due to the mixed nature of items, a total score from this measure could not be calculated with group comparisons instead facilitated at an item level. Satisfactory internal consistency has been demonstrated for the current data set (Cronbach’s alpha = 0.83). STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) guidelines for observational research were adhered to in the reporting of this study (Supplementary File 2).
Participant Recruitment
All available work email addresses of nursing staff (N = 1,541) at [hospital name] were sent an email with study information and a link to participate in the online survey. The distribution list for nursing staff was developed by collating the organization email addresses of all staff in the email directory with a role description that aligned to nursing (e.g., Nurse, Nurse Unit Manager, Assistant Nurse Unit Manager, Nurse Educator, Registered Nurse, and Enrolled Nurse).
Ethical Considerations
This study was approved by Melbourne Health Research Ethics Committee with approval number HREC/17/MH/283. Survey completion was voluntary, and participants were able to withdraw prior to the submission of responses, due to the anonymous nature of data collection. Participants were fully informed about the research goals, with informed consent assumed upon survey submission.
Statistical Analysis
All data was analyzed using SPSS (version 27). A two-sided alpha value of less than 0.05 was considered statistically significant for all analyses. Owing to the ordinal nature of data, a series of Kruskal–Wallis tests, with Bonferroni corrected pairwise comparisons, were used to explore differences in self-reported rates of knowledge, confidence, screening, and frequency of working with clients who disclose between professional areas. Effect sizes were calculated using Cohen’s f coefficients, with magnitude interpreted according to Cohen (1988) (0.1 = small, 0.3 = medium, and 0.5 = large). Nominal data relating to demographics, understanding of indicators, knowledge of how to manage disclosures, and ability to inquire about violence were compared using Chi-Squared Analyses with post hoc analysis using Bonferroni correction (Beasley & Schumacker, 1995).
In order to understand the manifest level of nursing experiences, free text responses were analyzed using qualitative description with overtones of content analysis (Graneheim & Lundman, 2004). The qualitative description was chosen as it provides a comprehensive summary of nurse perceptions in the accessible and translatable language (Sandelowski, 2000). In this regard, text responses were read for familiarity, with content and meaning units (words/phrases) identified and condensed. Codes were assigned to structure meaning units and the codes were discussed and agreed upon by two independent researchers (TW and NR).
Results
Sample Characteristics
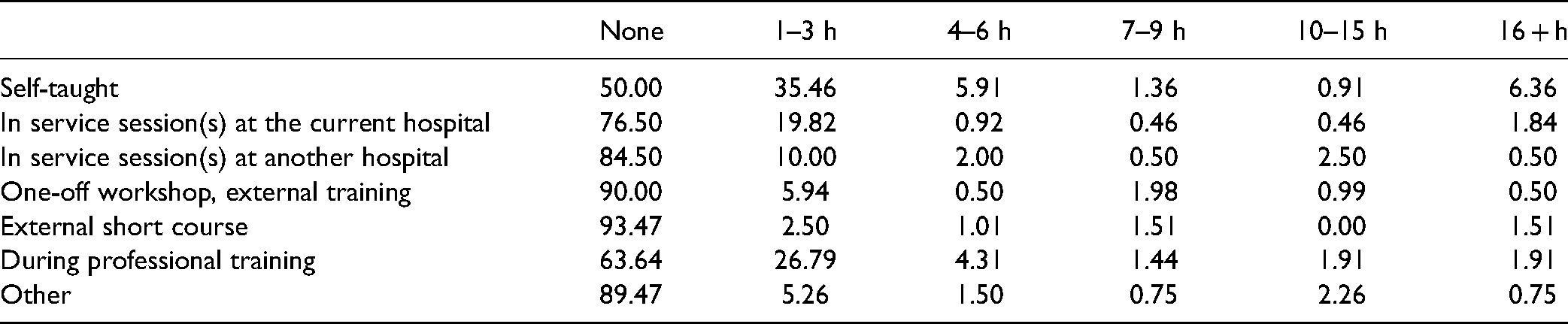
Two hundred and forty-two nursing staff participated, representing a total response rate of 15.7%. The majority of respondents reported working in the acute inpatient units (n = 141; 58.3%). Of the remaining nurses, just over one quarter worked in the emergency department (n = 64; 26.4%) and 15.3% worked in subacute areas (n = 37). The majority of the sample were experienced nurses, with 53.3% (n = 129) having 10 years + of clinical experience, 21.9% (n = 53) with six to 10 years, 23.1% (n = 56) with one and five years, and only four nurses (1.7%) less than one year of clinical work experience. When applying post-hoc correction, there was no significant difference in years of experience between clinical work areas. The majority of nursing respondents reported receiving some form of FV training at any time in the past (n = 163; 67.4%); although most of this was through self-taught means (for further characterization, see Table 1). There was no significant difference between the clinical work area and previous FV training exposure, χ2 = 4.63, p = 1.00, two-tailed.
Respondent Ratings by Percentage of Sample for Type and Hours of Historic Family Violence Training.
Knowledge, Confidence, and Screening
As seen in Table 2, FV knowledge and confidence rates were generally low for the nursing groups as a whole. Self-reported FV screening rates and perceived frequency of working with patients with FV experiences were also low. Baseline levels of FV knowledge, confidence, and clinical skills were compared using a series of Kruskal Wallis non-parametric analyses (see Table 3 for associated mean ranks).
Nurses’ Self-Ratings of Skills and Experience in the Area of Family Violence by Survey Question.

Note. FV = family violence.
Mean Rank for Nurses Knowledge Confidence and Screening Practices by Clinical Area.
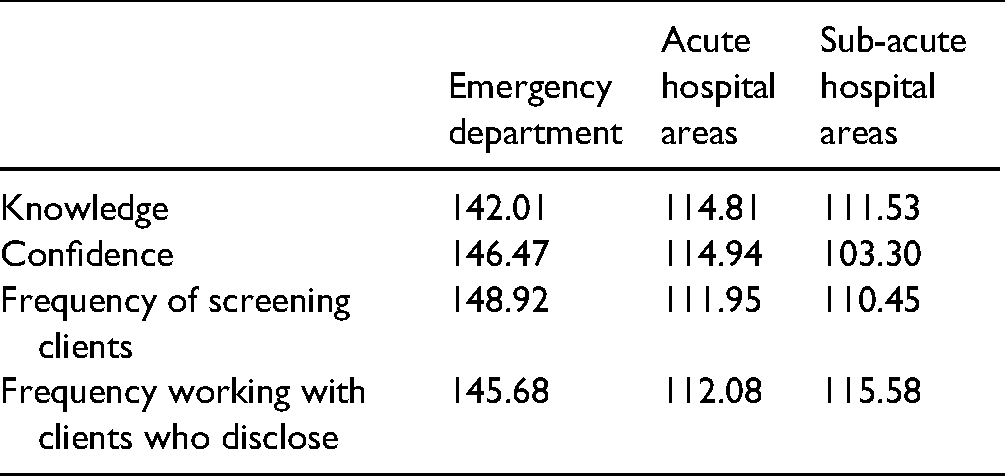
There was a small statistically significant difference between self-reported FV knowledge among clinical work areas, H = 10.42, df = 2, p = .005, Cohen’s f = 0.21. Post-hoc analysis using pairwise comparisons indicated that emergency department nurses reported significantly higher levels of knowledge than their acute (p = .002) and subacute (p = .013) colleagues. No significant difference in knowledge ratings were seen between acute and subacute nurses (p = .77).
For FV clinical confidence, there was a small, statistically significant difference between self-reported confidence among clinical areas, H = 13.41, df = 2, p = .001, Cohen’s f = 0.24. Pairwise comparison with Bonferroni correction again revealed significantly greater confidence ratings among emergency department nurses relative to colleagues in acute (p = .007) and subacute (p = .039) work areas, with no differences between acute and subacute nurses (p = 1.00).
A small, statistically significant difference was seen between professional groups on self-reported frequency of screening clients for FV, H = 14.90, df = 2, p = .001, Cohen’s f = 0.26. Emergency department nurses reported a significantly greater frequency of screening clients than acute (p = .001) and subacute (p = .015) colleagues. No significant difference in ratings of screening was seen between acute and subacute nurses (p = 1.00).
Finally, on ratings of the frequency of working with clients who have disclosed FV, Kruskal–Wallis analysis indicated a significant difference between clinical work areas, H = 11.79, df = 2, p = .003, Cohen’s f = 0.22 of a small magnitude. Emergency department nursing respondents again reported significantly greater frequency of working with clients who had disclosed, relative to colleagues in acute areas (p = .002). No difference was seen between the emergency department and subacute nurses (p = .081), nor between acute and subacute respondents (p = 1.00).
Clinical Skills
A series of chi-squared analyses were used to examine differences in knowledge of FV indicators, FV enquiry skills, and capacity to respond to disclosures (see Table 4). As noted in Table 4, no significant differences in these clinical skills in these areas were identified across nursing groups.
Frequency of Family Violence Skill Endorsement by Clinical Area.

Barriers
In addition to descriptive analysis, a series of chi-squared analyses were used to examine differences in barriers nominated by nurses across the clinical area (see Table 5). While a number of significant differences were seen in barrier endorsement across clinical groups, none remained significant when Bonferroni correction was applied in post hoc analysis. Regardless, from a whole sample perspective, the presence of a suspected perpetrator was nominated as the most common barrier by participants (n = 142; 58.68%), followed closely by concern at impacting rapport with a patient (n = 139; 57.44%). Lack of clinical supervision in the area was the least endorsed barrier by respondents (n = 72; 29.75%).
Frequency (n) of Barrier Endorsement by Clinical Area.

Note: ED = emergency department.
Qualitative Responses
Identifying indicators of violence
Fifty-four respondents who reported that they “knew” or “somewhat knew” about indicators of violence provided free text responses. The pattern of responses was similar across clinical areas with repeat, unexplained hospital admissions and suspicious injuries most cited as indicators of violence, together with overt physical and emotional indicators of abuse (see Table 6).
Qualitative Responses for Identification of Indicators of Violence.

Asking about violence
Respondents who indicated that they knew, or somewhat knew, how to appropriately ask about FV, were requested to describe how they would do this. A total of 52 respondents provided free-text responses. Respondents commented on the importance of the environment and being aware of potential safety risks when asking about violence. Several nursing respondents also spoke about the need to ask whether a patient felt safe to return home with a variety of questioning styles adopted (see Table 7). Emergency department nurses more commonly identified the importance of asking about safety relative to other clinical areas, with greater emphasis on environmental and safety considerations. By comparison, acute inpatient nursing staff more frequently cited rapport considerations in asking about violence with a variety of open and more directive approaches to inquiry.
Qualitative Responses for Asking About Violence.

Responding to disclosures of violence
Descriptive analysis was undertaken on 98 free-text responses provided about the clinician’s response to victim-survivor disclosures of violence. The majority of respondents indicated that they would escalate the situation to a senior nurse or doctor and/or make a referral to social work (see Table 8). However, vagueness and uncertainty about managing disclosures of violence were clear from a number of respondents. Emergency department nursing more frequently commented on the importance of patient safety relative to other clinical areas. No further notable differences were observed.
Qualitative Responses for How to Respond to Disclosures of Violence.

Barriers to working effectively
Descriptive analysis was undertaken on 31 respondents. The pattern of qualitative responding was the same across clinical areas with a lack of formal training and time constraints most commonly described as barriers to respondents (see Table 9).
Qualitative Responses for Barriers to Working Clinically in Family Violence.

Discussion
This study aimed to characterize and contrast the knowledge, confidence, clinical skills, and perceived barriers in responding to FV among nurses across three primary clinical work areas. Notably, results revealed service-wide deficits in knowledge, confidence, and self-reported clinical skills irrespective of the clinical work area. The majority of nurse respondents reported limited knowledge and confidence in working clinically in the area; a finding consistent with existing literature (Alshammari et al., 2018; Sundborg et al., 2012). Qualitative data further reflected deficits in responding to FV, including a poor understanding of pathways to support victim-survivors following disclosures. Taken together, these findings reinforce the under-preparedness of nurses to respond clinically to FV.
Despite overall low levels of knowledge and confidence across the sample, when qualitative free-text data was provided for nurses who self-reported “knowing” or “somewhat knowing,” it reflected a reasonable understanding of indicators of violence; a pattern seen consistently across clinical areas. Nominated indicators ranged from overt physical manifestation (e.g., bruising and unexplained injuries) to covert social indicators and behavior (e.g., interaction with a partner). Yet even with the capacity for identification, the mixed methods data reflects a degree of uncertainty in nurses regarding how to respond to FV disclosures, with most assuming a passive role in clinical management. Taken together, the data suggests nurses often have the skills to identify violence indicators but require further education and training to improve the response to disclosures. Hence, while nurses in this sample had some awareness about when FV is occurring in their patients, they lack the skill set, knowledge, and confidence to effectively respond, to assist patients with their situation.
Paralleling clinical skills deficits was a lack of structured training among this cohort, with the majority of respondents reporting engagement limited to unstructured, self-taught means of training. The lack of available training programs to support clinical responding to FV has been previously highlighted (Alshammari et al., 2018; Beccaria et al., 2013; Wathen et al., 2009) and may underpin the lack of confidence, knowledge, and clinical skills. These findings have concerning clinical implications, particularly given the unique and privileged role nurses play in the hospital setting. Relative to other disciplines, nurses spend a significant amount of time with patients across repeated points of contact in the hospital. Hence, nurses are well positioned by virtue of their clinical responsibilities to play an active role in supporting victim-survivors. A lack of clinical capabilities may also explain, at least in part, nurses’ perceptions that they do not often work with patients with FV experiences. The majority of participants reported that they “never” or “very rarely” had exposure to patients who had disclosed FV experiences. This contrasts with known high rates of FV in the Australian community (AIHW, 2019), high rates of hospital usage among victim-survivors (Campbell, 2002), and high rates of patient-reported FV disclosures to clinician staff at the same hospital (Fisher et al., 2020). Thus, nurses may not be aware patients are experiencing FV, because they are not screening regularly, leading to potential missed opportunities to provide support and assistance. Collectively, the findings highlight the urgent need for formalized FV training to be implemented systematically within training programs and hospital services. To sustainably support training implementation, the landscape in which these programs sit needs to recognize the health implications of FV and make a concerted effort to emphasize the role of all clinical staff in responding to FV.
Comparisons of clinical preparedness across professional areas yielded several interesting findings. The results indicated significantly higher rates of FV confidence and knowledge among emergency department nurses relative to acute and subacute clinical counterparts; a finding not previously demonstrated in the literature. Moreover, qualitative outcomes highlighted a greater focus on safety considerations when asking about and responding to violence among emergency department nurses. The directionality of these differences is not unexpected and makes intuitive sense given the local environment of the emergency department. With consideration to pathways of care, the emergency department typically represents the first point of contact an individual will have with the hospital system and hence the first possible opportunity for identification and/or disclosure of FV. The high flow of visitors and staff through this area, together with pragmatic space considerations may also account for the relative focus on safety among emergency department nurses. A study within the same hospital surveyed patients from a broad range of clinical streams for their FV screening experiences and revealed that 80% had utilized the emergency department at some point in time (Fisher et al., 2020). Moreover, existing literature has found disproportionally high rates of emergency department usage among victim-survivors of FV (Kothari et al., 2015). Thus, nurses working in the emergency department may have greater exposure to patients with a history or current experiences of FV and consequently may have a greater opportunity to refine and develop FV clinical skills. In support of this hypothesis, emergency department nurses in this sample reported a significantly higher frequency of working with patients who have FV experiences and greater clinical capabilities in responding to disclosures of violence. Importantly, however, although higher rates were seen in this clinical area, overall rates of knowledge, confidence, and clinical proficiencies remained low. Thus, while relative areas of clinical strength may be indicated in emergency department settings due to the nature of contact with patients, there is room for further skills improvement, even in these areas.
In consideration of barriers to responding to FV, several key issues were identified by nurses. The presence of a suspected perpetrator was nominated as the most common barrier by participants. The high number of nurses endorsing this barrier (59%) may reflect the likelihood of suspected perpetrators attending appointments and admissions with a victim-survivor and highlights the pragmatic limitations of enquiring about and responding to violence in a health service. The next most commonly endorsed barrier by nurses was concern about affecting rapport with a patient. Existing literature highlights the openness and willingness of patients to disclose violence when asked confidently and directly (Bacchus et al., 2002, 2003) and re-enforces the need for education to support nurses in sensitively inquiring about violence. Interestingly, despite the lack of formal training in the area and suboptimal clinical readiness, the availability of clinical supervision was the least common barrier identified. The immediate reason underpinning this discrepancy is not immediately clear but may relate to different perceptions of supervision among nurses. External to nursing, supervision is used as a tool for ongoing professional development and support. However, within nursing, supervision may be perceived as “observational” and direct guidance on a procedure or clinical issue; a disparity in implementation which may explain the findings. Interestingly, from a comparative level, no significant differences were identified between clinical areas in terms of perceived barriers. Thus, limitations to effectively managing FV in a hospital setting appear to be consistent across clinical areas.
Strengths and Limitations
While this study provides a helpful snapshot of nurses’ readiness to respond to FV in a tertiary hospital, it is not without limitations. Notably, this cross-sectional study surveyed a percentage of staff from a single healthcare service. Response rates as a percentage of the total nursing staff were low. In addition, given the self-selecting nature of participation, it is possible that nurses who did participate had prior interests or perceptions about FV. Collectively, these limitations may impact the representatives of the study sample and limit generalisability. However, it is important to note that the response rate in the current survey, at close to 15.7%, for nursing staff, is considerably stronger than that obtained in healthcare workers in the same region in two recent studies (i.e., Soh et al. 2021 at 6.8% and Forsdike, et al., 2019 at 4.8%). It is also in keeping with other healthcare worker studies with survey pools of >1500 where surveys are distributed via online only administration and email invitation for participation (e.g., Hassenbusch and Portenoy, 2000 at 18.70%; Hollowell et al., 2000 at 13.96%). Although our findings are consistent with existing literature, further exploration in a more representative sample is recommended. Similarly, the self-reported nature of this tool is also a limitation, as responses may not fully reflect what occurs in actual clinical practice. Future research should seek to replicate this study across settings and investigate objective measures of actual responses and services provision for patients experiencing FV.
Conclusions
Nurse respondents overall reported low rates of confidence, knowledge, and clinical skills in responding to disclosures of FV on a background of limited training exposure and opportunities. While many nurses were able to effectively identify indicators of FV, collectively they generally lacked the clinical skill set needed to manage and respond to these indicators effectively. Isolated areas of relative strength were evident among nurses working in the emergency department which may relate to the higher level of exposure to patients experiencing FV in this care setting. This research provides a useful snapshot of nurses’ perceptions of their FV skill levels in an Australian tertiary trauma hospital.
Implications for Practice
Findings reinforce the relative under-preparedness of nurses to respond to FV and the corresponding need for imbedded training programs to support knowledge and confidence in managing disclosures of FV. Notably, this study team in conjunction with governmental support has implemented structured FV training in the local hospital environment. Systematic evaluation of this initiative is currently underway and will be published elsewhere.
Supplemental Material
sj-docx-1-son-10.1177_23779608221126355 - Supplemental material for Preparedness to Respond to Family Violence: A Cross-Sectional Study Across Clinical Areas
Supplemental material, sj-docx-1-son-10.1177_23779608221126355 for Preparedness to Respond to Family Violence: A Cross-Sectional Study Across Clinical Areas by T. D. Withiel, BSc, S. Sheridan, BSc, N. Rudd, BA and C. A. Fisher, BA in SAGE Open Nursing
Supplemental Material
sj-doc-2-son-10.1177_23779608221126355 - Supplemental material for Preparedness to Respond to Family Violence: A Cross-Sectional Study Across Clinical Areas
Supplemental material, sj-doc-2-son-10.1177_23779608221126355 for Preparedness to Respond to Family Violence: A Cross-Sectional Study Across Clinical Areas by T. D. Withiel, BSc, S. Sheridan, BSc, N. Rudd, BA and C. A. Fisher, BA in SAGE Open Nursing
Footnotes
Acknowledgments
We thank all of the clinicians that supported the conduct of this study and invested their time and effort into making it possible.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. This work was supported by the Victorian Government (grant number Strengthening Hospital Responses to Family Violence).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.