
Abstract
Aim
The study aimed to explore the perceptions of intensive care unit staff deployed to other clinical areas. It also aimed to identify challenges that the staff face during their redeployment.
Design
A mixed method study. Method: 40 participants (nurses and healthcare assistants) completed an anonymous online questionnaire, and five participants (nurses) participated in one-to-one semi-structured interviews. Participants were recruited through purposive sampling from the selected ICU/HDU.
Results
Content analysis of the data revealed three major themes: “Negative feelings of redeployment”, “Positive feelings of redeployment” and “Visible and Structured leadership interventions”. Results indicate that ICU nursing management needs to make some additional efforts and implement the study recommendations to improve the overall perception and experience of ICU/HDU staff redeployment. Public Contribution: This research will create insight into the redeployment of intensive care unit staff to other clinical areas. Furthermore, it will add value to patient safety and improve institutional healthcare policies.
Keywords
Introduction
Nurse redeployment is not a new practice in the Intensive Care Unit (ICU) and High Dependency Unit (HDU); it has become much more significant during the COVID-19 pandemic to address the staffing deficit in other clinical areas. Redeployment, often known as “being redeployed,” or “floating” has historically been utilized to alleviate staffing shortages in other units (O’Connor & Dugan, 2017). In most cases, redeployment helps in controlling varying patient acuity and census. In 2022, around 5537 nursing hours of redeployment occurred for registered nurses and healthcare assistants in the study ICU/HDU. This represents a total of more than two full-time equivalent staff being transferred to different areas of the hospital to aid with staffing needs and increased patient acuity. This capacity to assist other wards is partly due to the increased staffing numbers for the ICUs in New Zealand as a result of the COVID pandemic critical care capacity (Young et al., 2021). According to the available statistics from the study ICU, when there is extra staff in the unit often the duty manager or the charge nurses send that staff to another unit where there is a staff shortage. However, deployment from another unit to
Literature Review
Following best practice, an effort has been made to move nurses between similar units in the hospital, for example, a nurse from an intensive care unit moving to the emergency department to work in the resuscitation area. However, this is not always the case, some nurses are transferred to an unfamiliar unit or specialty, leading to a degree of discomfort. The position of the Joint Commission on Redeployment Operations (2004) supports that nurses moved to another unit must be assigned to a unit with similar patient populations and skill requirements. Additionally, the deployed nurses must have appropriate credentials to practice in another unit
The New Zealand Nurses Organization (NZNO) has implemented the Care Capacity Demand Management (CCDM) program in multiple district health boards (DHB's). The CCDM document clearly states that Staff redeployment is not the first line of action as a response to increasing acuity and utilizes metrics to guide actions such as moving patients from one area to the other rather than staff moving as it influences safety hence, reorientation to a new area is required if redeployment is to occur (McKelvie, 2018).
The American Nurses Association (ANA, 2009) argues that nurses have the right to refuse or reject a patient assignment that puts patients or their safety at risk. Before redeploying nurses from one unit to another, the manager must consider the nurse's level of experience, expertise, patient acuity, and care needs. If redeployment is required, the nurse should be redeployed in a similar clinical area (ANA, 2009).
The argument in this article is that nurses in the New Zealand have received comprehensive nursing training. However, they have all achieved clinical competence in the nursing area they practice. The assumption is that management does not take into account the expertise of ICU nurses when deploying them to other clinical areas. Rather there is a believe that a nurse is a nurse regardless of their clinical expertise and competence. The nurse is not consulted or discussed with regarding redeployment, only given instruction. Redeployment can be highly stressful event, depending on the area of allocation and tasks. Literature also suggests that nurse redeployment is associated with poor nurse and patient satisfaction, decreased productivity, and impaired nurse-patient relationships (O’Connor & Dugan, 2017). Additionally, there is a positive association between redeployed nurses and an increase in staff turnover. There are multiple pieces of research done about nurses’ redeployment during the COVID-19 pandemic, but there has been no study in New Zealand around ICU staff redeployment and there are few international papers on this topic. It is believe through this mixed-method research an insight into redeployment to other clinical areas will be achieved by understanding the views of ICU nurse regarding redeployment to other clinical areas.
Methodology
Study Design
A single site, mixed method study was undertaken to explore the perception and challenges of the Intensive care staff during their redeployment to other clinical areas. A sequential explanatory mixed methods approach was utilised; initially, an anonymous online survey was conducted, the data from the survey were then analysed, and the findings were used to form the development of questions for semi-survey interviews (Creswell & Creswell, 2017). The qualitative element included face-to-face semi structured interviews focusing on perception and challenges ICU/HDU staff experience during redeployment to other clinical areas.
Setting and Sample
The study was conducted in a 14-bedded intensive care unit / high dependency unit in a single large 663-bedded hospital in Northern Auckland, New Zealand. The ICU/HDU serves a general mixed medical and surgical adult patient population. At the time of the study, 64 nurses and healthcare assistants were working in the ICU/HDU including the bedside nurses, coordinators, and associate clinical charge nurses (ACCN's). To be eligible for the study the participant has to be a registered nurse or healthcare assistant in the ICU/HDU, working for more than six months in the current ICU/HDU and redeployed to another unit in the last 6 months. For the quantitative survey, participants were recruited through purposive sampling via an email invitation to all eligible ICU/HDU nurses. Interested participants completed the online anonymous questionnaire. Subsequently, a further email was sent to all eligible ICU/HDU staff requesting volunteers to participate in a face to face interview, and to contact an external qualitative researcher if they wanted to take part. All interested participants were interviewed later.
Data Collection
Questionnaire
The online anonymous survey included twenty-seven open and close-ended questions. Quantitative data were analyzed using descriptive statistics and qualitative data were coded, categorized, and themes developed.
Interviews
The semi-structured interviews were conducted either face to face or via Zoom, by a qualitative researcher who was external to the ICU/HDU team so staff participation could be kept confidential from the ICU/HDU research and management teams. Even though the researcher was not the part of ICU/HDU team, she has previous critical care nursing experience which enabled a clear understanding of the study context
The face to face interviews offered the researcher an opportunity to read the participants’ body language and to understand the hidden meaning of non-verbal clues (Ryan et al., 2009). It also provided an opportunity for the participant to express their thoughts openly independent from the critical management structure. The interviews were conducted at a time and place convenient to the participants. Each interview lasts between 20 and 30 min in duration. The interviews were audio taped and transcribed verbatim.
Analysis
The quantitative questionnaire was analysed using descriptive statistics. The qualitative data were analysed using Graneheim and Lundman's (2004) guidelines which include data coding, categorization, and theme formation. An ICU research team helped to identify the themes and completed the analysis and coding. Members of the ICU research team includes doctors and nurses with rich experience in intensive and critical care and research. Nurses hold Masters in Nursing Degree and Doctors with bachelors in medicine and surgery and specialization in critical care. Our ICU is affiliated with the Australia and New Zealand Intensive Care Society Clinical Trials Group.
In the mixed analysis, results from the quantitative and qualitative analyses were presented together in a discussion where they are grouped side by side, following the method presented by Creswell and Creswell, 2017.
Ethical Consideration
The study received locality approval from the study hospital (Registration #: REDACTED). The interviews include a participation information sheet and informed consent form, participants were asked to read the participation information sheet and the consent before the initiation of the interviews. All participant data were de-identified before analysis.
Findings
Table 1 displays the demographic characteristics of the survey respondents. Out of 64 ICU/HDU nurses and healthcare assistants, 37 nurses and three Healthcare assistants completed the online questionnaire, a 63%response rate, and five registered nurses participated in a semi-structured interview.
Participants Demographic Data.

Initially, the findings of quantitative data were used to formulate the qualitative questionnaire, and later the findings of both quantitative and qualitative data were combined together and formulated the themes. The three themes that emerged from the findings were negative feelings of redeployment (Figure 1), positive feelings of redeployment (Figure 2), and visible and structured leadership interventions (Figure 3).

Negative feelings of redeployment.

Positive feelings of redeployment.

Visible and structured leadership interventions.
(Table 2 displays participants’ wording & Figure 4 displays generated themes).
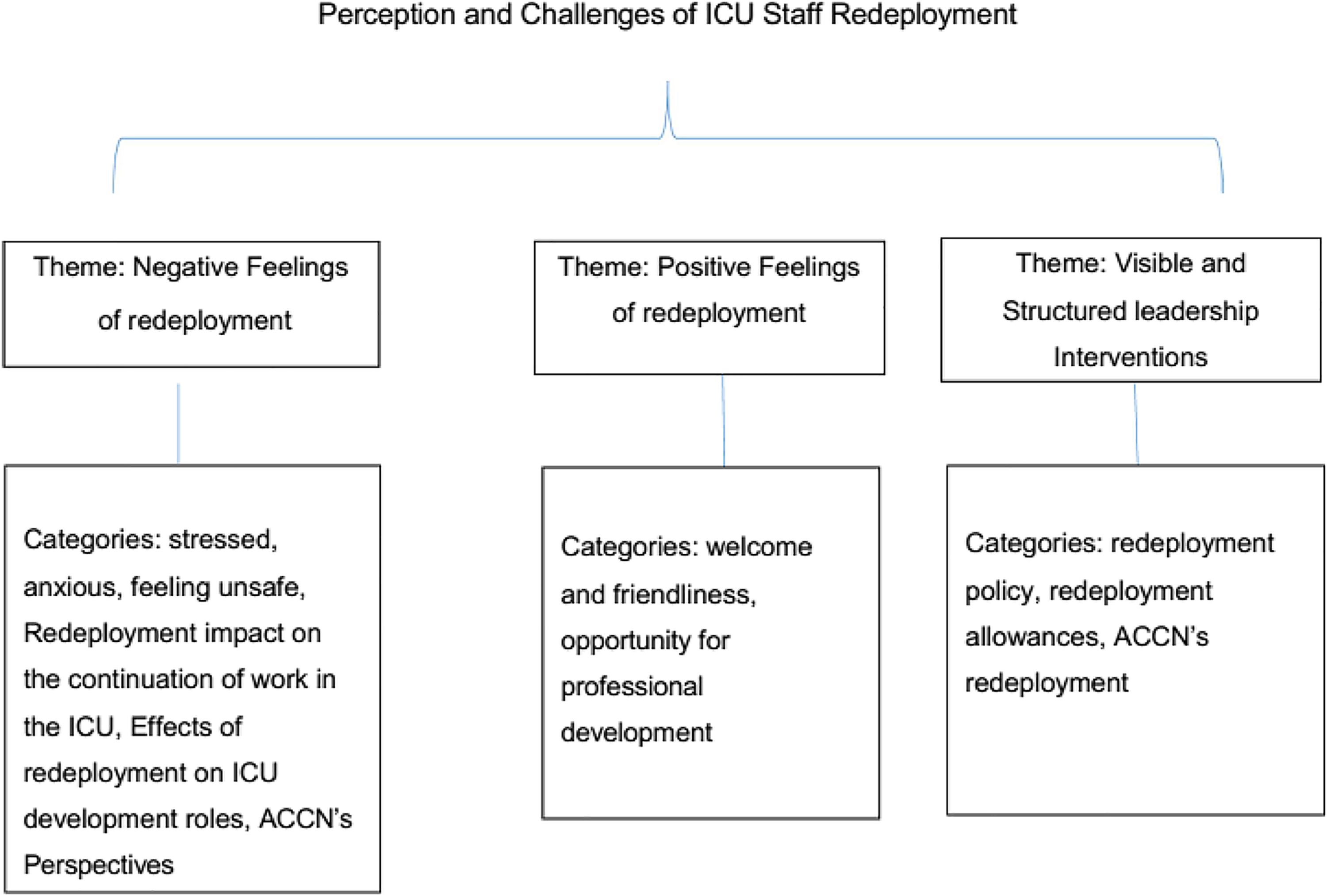
Themes and categories emerging from survey questionnaire and semi-structured interviews.
Phrases and Wording Associated with Themes.

Most participants (N = 26, 65%) felt anxious, stressed, and frustrated during their redeployment. This was represented in the associated qualitative commentary: “I'm feeling frustrated and anxious” another participant stated, “feeling responsible in a place that isn't my place of work, stressed, worried”.
Several participants (N = 19, 47%) verbalized that they feel unsatisfied when redeployed to another unit, which also affects their productivity “I feel extremely unsatisfied by the attitude of senior nursing management outside ICU towards redeployment of ICU staff, and treating them as bureau staff, it affects my morale”.
Several participants (N = 24, 60%) shared concerns about feeling unsafe when redeployed due to unfamiliarity with using an electronic medication management system, patient acuity, and unfamiliar working environment. A participant stated “I feel unsafe not knowing the processes, unfamiliar to place, procedures, and protocols” another stated,” I do feel that there is more risk of making a mistake because you are in an unfamiliar environment and you are given tasks to do for patients for whom you have very little information about”.
A large proportion of participants (N = 23, 57%) verbalized that they feel that their nursing registration is at risk and this makes them more scared and worried when they are redeployed, “In the past during deployments to the ward, the ward has been significantly short staff. There have not been enough people around to ask questions, confer about complex patients, etc. This can lead to some challenging situations and patient care interactions” another said “So many times I have given a patient medication by just trusting what their nurse has asked me to give them. There is not enough time or knowledge on my part to do anything different. This feels risky as we don't really know what we are doing, we are just taking orders. We don't write notes in the patient's notes, we don't have any way of recording except word of mouth”.
In addition, not only the ICU nurses but unit coordinators and ACCN's also felt uneasy when they have to redeploy their ICU/HDU staff to another unit and are concerned for their learning and development within the ICU. One participant stated, “They were employed for ICU and need to improve their skills and knowledge but lose opportunities to improve it”. However, it is always not easy for the coordinators to send the staff to the ward for help, they also struggle and face lots of challenges. One coordinator stated, “As a coordinator - I hate it [redeploying someone]; one staff member complained then said they felt sick and went home; another just said no and walked off the unit”. Coordinators also face less autonomy and are more dependent on the duty managers to manage the staffing in their unit. One coordinator verbalized, “The duty managers take in the number of patients but not the acuity; they don't know how many people it takes to roll a patient with shift break relief; they don't even come near the unit; I've had threats of escalation and comments that I'm not in charge but I say that I am responsible for the safety of the unit and escalated to the ICU/HDU unit manager”.
Some of the participants indicated that redeployment has a major impact on their will to continue working in the ICU. One participant stated, “If it's quite frequent. I should have applied for a bureau nurse or agency nurse”, another stated “But here they make us feel like they can just take us/use us whenever suits, and it's not always appreciated. Would be nice for the “everyone matters” value to be applied here”. Most of the nurses working in the ICU really enjoy their roles and responsibilities however they get literally upset and worried if they are unable to do what they like or want. One participant shared, “it felt like I am of no use in the ICU/HDU, I don't know if I want to continue in this ICU.”
Many of the participants shared that redeployment hinders their new learning in the ICU and slows down their ICU development. One participant stated, “I do three shifts a week, and one or two of those I could be redeployed” another mentioned, “even if not much going on [in ICU], just being in the environment you get to pick up/soak up things”. Nurses feel that to be a good critical care nurse, one needs to spend some quality time in the unit, it allows them to observe and learn new things from the surroundings. One participant responded, “I don't feel I've had the chance to be a critical care nurse for a decent chunk of time - I can be quite frustrated about it”. The redeployment of ICU nurses is not only restricted to senior nurses, even the new graduate nurses are also redeployed when the need arises. One new graduate nurse stated, “Redeployed about 9 or 10 months [new grad] because there was no one else who could go due to skill mix”.
Most respondents 67% (N = 27) described that the friendliness of the staff and the feeling of being welcomed into the team created a positive redeployment experience. One respondent indicated that she was very anxious initially, but with the support of the ward staff, she felt her redeployment experience was positive. Simple steps such as a quick orientation to the ward, introduction to ward staff working in the unit, and orientation to the toilets and staff room created a friendly and welcoming environment. The following quotes are examples of these elements. “Most staff are very welcoming and friendly. Re-deployment can be a good learning experience to see new presentations, Ward staff grateful for the help”, “Some areas are great to work in and staff is lovely, supportive and appreciative which always makes me feel great because we are here to help and take the stress off them. Also, nice to see other areas of the hospital and practice skills that we don't do often in ICU”
An aspect of this theme is the emotional impact on the respondents when they perceived themselves as unwelcomed, some described that they felt isolated or like a burden, while others reported that these negative experiences affected their motivation to come to work. It is not unreasonable to assume that these negative emotions impact on quality of care provided, an issue also raised by respondents: “Feeling uncomfortable and unwelcome by ward staff (sometimes, definitely not the majority of experiences). I have only been orientated to toilets/resus equipment etc once when working on a ward and that was because it was my first time being redeployed and specifically asked for a tour. I never really feel quite confident in the tasks I am doing as I am functioning on limited info about the patient, ward policies, etc. Some nurses on the ward also will delegate inappropriate tasks as they know we are from ICU, and they assume better knowledge, I feel this is sometimes unsafe for patient and nurse as we are working with limited knowledge of the patient and we are not the appropriate person to escalate to (they need to escalate to CCOT or ICU registrars)”
Overall, approximately 82% (N = 33) of participants viewed their redeployment experience as a positive one, 7.5% (N = 3) viewed it as negative and the remainder (10%, N = 4) skipped. Those who have positive views stated that “ I get to practice competencies more often required on the wards such as stoma care and IV cannulation, using some of my skills that I haven't been using recently”. Among them, most of the staff relate redeployment to learning new skills and practicing different nursing skills outside ICU “Learning new things unique in the ward” and Practicing ward skills that haven't always been practiced in ICU”.
Those who view redeployment as a negative factor for growth and development stated that “We apply to ICU to work in ICU so it is a bit disheartening to be in the ward for 1/3 of our shifts and it feels like I am losing my ICU skills”. Another participant added “Although I've had positive experiences and some staff on the wards have been lovely, they aren't where I want to work. I love being in ICU and am happiest when I have ICU shifts. I don't feel I learn much on the wards, and have sometimes experienced staff giving me plenty of tasks when they sit and talk amongst themselves”.
More than half of the participants stated that redeployment was not discussed with them in their interviews and they don't have any information about that (N = 21, 52%). “I am not aware of the redeployment policy”, one participant stated, and another said, “Redeployment was not discussed in my interview”.
Throughout this study, most of the participants shared that management should provide some allowances to the redeployed nurses as it will boost their energy mentally, will help them financially, and will be a fair distribution of money. “An allowance for being on-call for the wards would be appropriate and may result in less resistance to deployment”, another participant stated, “It would make the challenge more bearable”.
Overall, approximately (N = 22, 55%) participants shared that along with nurses the ICU ACCN or coordinator should also redeploy to ensure fairness in the practice of redeployment. One participant stated, “If it is supposedly about filling gaps in the hospital despite what needs to be done by us in ICU then sure why not?” another participant shared, “ I think they need to experience what it is like for us so they may be more sympathetic with our situation”.
Discussion
This mixed-method study explored ICU/HDU staff's experience of redeployment and the challenges faced by them. Key themes emerging from qualitative findings showed that “negative feelings of redeployment” was some challenges faced by ICU nurses during their redeployment, however, “welcome and friendliness” and “opportunity for positive development” were important elements to create a positive experience. The study also suggested “visible and structured leadership interventions” as a key theme in suggesting new strategies to overcome the redeployment burden on nurses.
Our results regarding nurses’ perceptions of redeployment showed that ICU nurses reported an increased level of stress and anxiety. Also, Ballantyne and Achour, (2022) and Crowe et al. (2021), found that the redeployment of nurses to other clinical areas has resulted in increased stress and anxiety among them. The feeling of unsafe, low morale, and unsatisfied was also common in our study participants as they always wonder if they are at high risk of making errors because of unfamiliarity with another ward routine and especially using the electronic applications to administer medications to the patients. The redeployment has also created a sense of fear among ICU nurses for their growth and development as critical care nurses. According to Matlakala, (2015) and Rattray et al. (2021), the consequence of taking a nurse out of their unit and placed in a different unit can lead to poor growth and functioning of the deployed nurse. The feeling of being less autonomous and more dependent on the duty nurse manager was also highlighted as the unit coordinators or the charge nurses’ decision was mostly overruled by the duty nurse manager's decisions to deploy ICU staff.
The study highlighted several positive features of redeployment to individual nurses and the organization as a whole. The positive features of redeployment include an opportunity for learning new skills and professional development especially when nurses are redeployed to an area that requires specialized nursing skills. However, depending on the duration and area of redeployment, there were some concerns about losing the opportunity to learn new skills in the ICU. Consistently, Kennedy et al. (2022) found that redeployed nurses should practice in the specialty areas to provide safe care and integrate specialized skills into patient care rather than providing hygiene care to the patients. Redeployment was also perceived as positive because of the friendliness and warm welcome by the ward nurses toward ICU nurses.
The study participants made some suggestions to improve the redeployment process which would make it less stressful for them; sharing of redeployment policy, introducing redeployment allowances, and redeployment of unit coordinators and charge nurses. Some study participants shared variation in redeployment duration i.e., some nurses are redeployed for a whole 12 h shift while others are only for 2 or 4 h. This variation in hours may affect nurses negatively. Furthermore, the findings suggested a structured orientation for the redeployed nurses in the ward, especially the usage of electronic applications for medication administration was a common concern among ICU nurses. Panda et al. (2021) showed that training and deployment of ICU nurses to other clinical areas was feasible. They demonstrated that if the ICU nurses are reoriented about the electronic notes entry and electronic medication administration through structured orientation will result in both safe patient care and staff well being.
Finally, the findings suggest that nurses should be redeployed based on their previous ward experiences or from one critical care area to another critical care. Familiarity with similar units and skills improves nurses’ confidence to care for patients and improves their redeployment experiences (“Joint Commission on Accreditation of Healthcare Organizations (JCAHO),” 2004).
Implications for Practice
This article presents to the reader the perceptions and challenges of redeployment among ICU staff. The study findings suggest that sharing of redeployment policy and adhering to the policy standards is important. The current ICU redeployment policy emphasizes sending the ICU nurses to the emergency department (ED), patient at risk (PAR), coronary care unit (CCU), and surgical unit. However, ICU nurses are being redeployed to hospital wide, which creates a sense of stress and uneasiness for them. Creating a peer support group in the unit and providing consultation and emotional support to the staff prior to redeployment by the charge nurses, providing deployment allowances, and practicing e MAR in the unit would be beneficial to improve ICU staff redeployment to other areas.
Conclusion
To conclude, this study aimed to explore the perceptions of intensive care unit staff redeployed to other clinical areas. The findings revealed that ICU nurses experience multiple challenges due to the frequent deployment in other units. There was a large proportion of staff who expressed negative feelings toward deployment. Factors like frequent deployment, lack of expertise in the particular clinical area, working with unknown staff, and sometimes 12 h away from their unit increase the magnitude of anxiety and stress among the ICU nurses. However, the findings also revealed that some study participants associate positive experiences with their redeployment because of the positive and welcoming attitude of the ward nurses, and their ability to practice and showcase their ICU skills in the ward.
This study suggests that nursing leadership and management have to make some additional efforts based on the study survey and recommendations to improve the overall perception and experience of ICU/HDU staff redeployment.
Footnotes
Acknowledgement
Researchers appreciate Ms Kathryn Tennant, an external qualitative researcher for conducting the face to face interviews. We also would like to thank all the study participants.
Author Contribution
Hina Karim She is the main author, she contributed to topic selection, getting approval, collecting the data, preparing the manuscript, and approaching the journal for publication.
Peter Groom He contributed to providing expert opinions in recommendations and suggestions.
Melvin Tiu He contributed to a literature review, wrote the manuscript, and provided recommendations.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.