
Abstract
We conducted a systematic review of literature from the years 2000 through 2017 on the prevalence and burden of lower urinary tract symptoms (LUTS) in men aged 50 and older, and medical treatments of and alternative nonmedical approaches to LUTS. EBSCOhost (Medline with Full Text) was searched for observational, experimental, and review studies in peer-reviewed journals in the English language. Our review found that LUTS were highly prevalent in the world and estimated to affect 2.3 billion people in 2018, with 44.7% being men. Men with LUTS suffer from not only burdensome symptoms such as nocturia and urgency but also adverse psychological consequences (e.g., anxiety and depression) and financial burden. Current medical treatments are clinically effective, but their efficacy is compromised by side effects and low compliance rates. Alternative nonmedical treatments for LUTS were also sought worldwide. There is evidence that lifestyle modifications such as pelvic muscle exercises and bladder training, physical activity, dietary modification, and nutritional supplements can alleviate LUTS and improve patient quality of life; however, evidence based on rigorous methodology remains minimal and cannot be generalized across populations. Evidence of effectiveness of weight loss programs to reduce LUTS is inconclusive. We conclude that although behavioral treatment is a promising approach to alleviating LUTS, especially when combined with medical treatments, well-designed randomized controlled and longitudinal clinical trials on behavioral treatments of LUTS are still needed. Minimally invasive procedures and neuromodulation therapy also show positive results of alleviating LUTS but require further research as well.
Introduction
Lower urinary tract symptoms (LUTS) are estimated to affect 2.3 billion individuals, or 45.8% of the world population in 2018, an increase of 18.4% since 2008 (Irwin, Kopp, Agatep, Milsom, & Abrams, 2011). According to the International Continence Society (2015), LUTS are defined as symptoms that result from conditions and diseases affecting the bladder and the urethra, including urinary incontinence (e.g., stress, urge, and mixed urinary incontinence); storage/overactive bladder symptoms (e.g., urgency, frequency, and nocturia, with or without incontinence); voiding (e.g., urinary retention, hesitancy, straining to void, slow or interrupted stream); and postmicturition (e.g., postmicturition dribble). LUTS have multifactorial causes that present a challenge to the management of this chronic problem. Despite various options of medical treatments, LUTS remain a significant public health problem and economic burden on society.
LUTS prevail among men aged 50 and older and become increasingly common in American men as the population ages. During the past decade, best practice guidelines for LUTS treatments were published in the United States and Europe (see American Urological Association, 2010; Oelke et al., 2013 for LUTS due to benign prostatic hyperplasia [BPH]), and the guidelines recommended behavioral management in which health professionals play a significant role. Evidence of LUTS prevalence, treatments, and behavioral therapies has emerged. There is a review of evidence published before 2000 (Bruskewitz, 1999). Since then, there have been systematic review studies that focused on medical treatments or herbal treatments of LUTS across countries, but there is a lack of systematic reviews of the prevalence of LUTS or other alternative treatments (e.g., lifestyle, weight loss, dietary nutrition, and acupuncture) that have emerged worldwide over the past decades. Hence, we conducted a systematic review of literature since 2000 to present the prevalence of LUTS from a global perspective and a comprehensive review of LUTS treatments. This review fills in a gap in the literature by presenting the estimated global prevalence and impact of LUTS on quality of life (QOL) over past 18 years and examining newly emerged alternative treatments for LUTS. Our objective is to provide health-care providers, especially nurses, with evidence-based information on LUTS, its treatment, and management for improving clinical treatment strategies and reducing the impact of this significant problem.
Methods
Extant research on LUTS prevalence, current medical treatments, and alternative treatments from January 2000 through 2017 were reviewed using database Medline with Full Text (EBSCOhost) that provides a reputable source of selective, qualifying biomedical and life science journal articles (National Institutes of Health, 2018). The systematic search generated 1,549 publications on LUTS. Using keywords of lower urinary tract symptoms (LUTS) AND prevalence, 442 references were found. Studies that were not available in English, did not use a population-based large database, or discussed the prevalence of LUTS in subpopulations with specific diseases (e.g., diabetes, Parkinson's disease, and cardiovascular disease) were excluded. Twenty-eight articles discussing the prevalence of LUTS in men in the general population were selected for review.
Examining the impact of LUTS, we used the keywords of lower urinary tract symptoms (LUTS) AND quality of life AND male. A total of 561 results were generated. After excluding articles of drug efficacy, assessment and management of LUTS, physician perceptions of LUTS patients, and QOL in specific disease context (e.g., poststroke, muscular dystrophies, and diabetes), 18 articles regarding QOL in men with LUTS were selected for review.
For medical treatment of LUTS, using keywords of lower urinary tract symptoms (LUTS) AND current treatment OR intervention OR therapy, 180 references were found. After excluding studies that treated LUTS in patients with a specific disease (e.g., diabetes, heart diseases) or primarily focused on QOL as treatment outcomes, 18 studies that examined the effectiveness of current medical or surgical treatments of LUTS, medication adherence, and side effects, through systematic reviews or using a large database, were identified.
Finally, research on alternative nonmedical treatments of LUTS was reviewed extensively on both EBSCOhost and Medline (PubMed), because many studies in this area are newer or exploratory, and PubMed allows us to access them in open access journal articles and in process or ahead-of-print articles (National Institutes of Health, 2018). Using the keywords of lower urinary tract symptoms (LUTS), treatment, alternative, behavior, lifestyle, pelvic floor, pelvic floor exercises, bladder training, muscle strength, intervention, self-care, nonpharmacological interventions, exercise or physical activity, and diet, we identified 366 articles. Excluding articles on metabolic syndrome, preventive care, and prostate cancer, 29 articles were identified for the review, including 8 articles related to lifestyle modification, 4 articles focusing on physical activities and weight loss, 14 articles on nutrition and supplements, and 3 articles on acupuncture. Of these selected 93 articles, 8 articles were identified for review in two separate areas. Thus, the total number of publications selected for this review is 85. The following flowchart outlines this selection process (Figure 1).
Flowchart of the search process.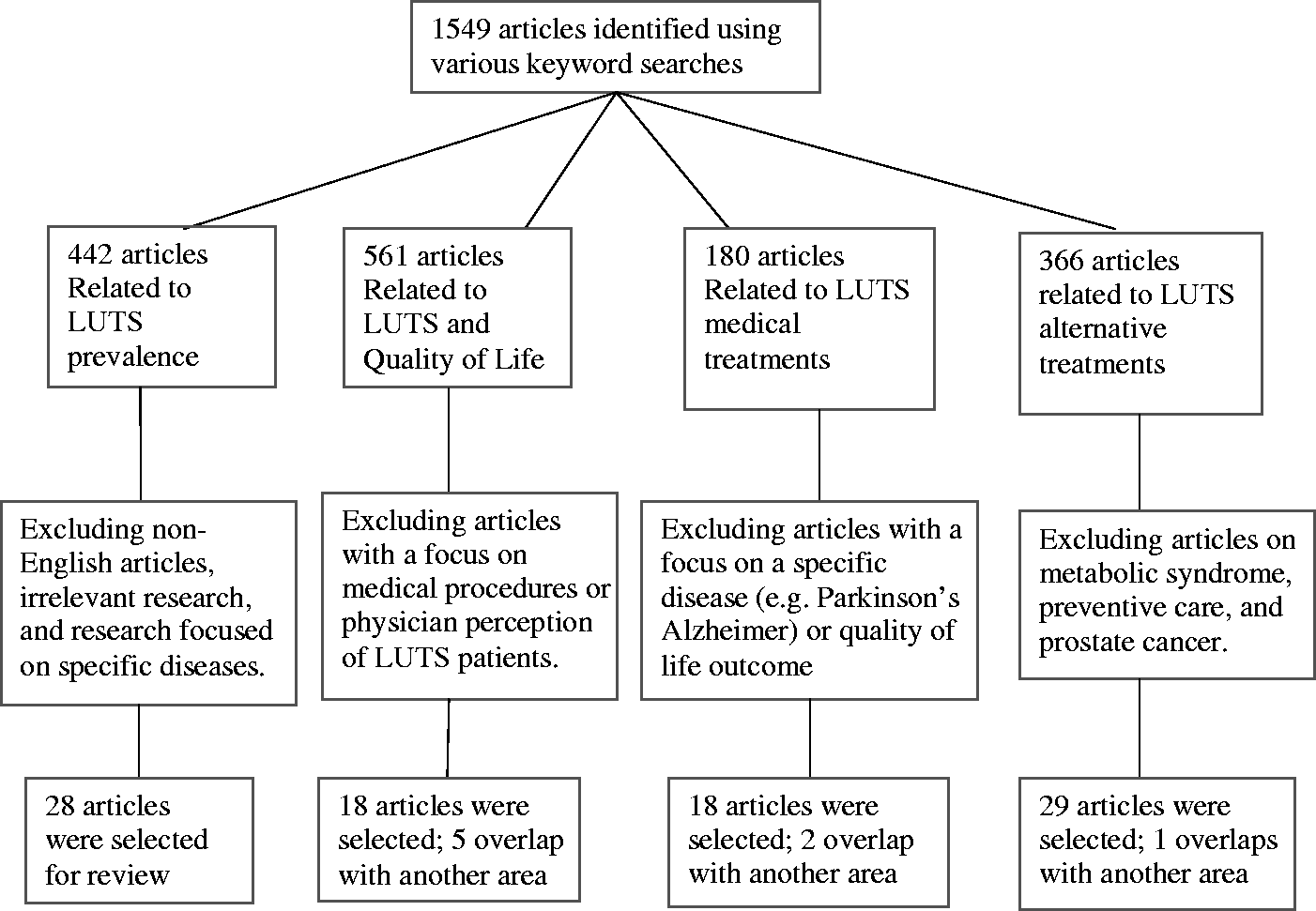
Results
A Summary of Reviewed Studies.

Note. LUTS = lower urinary tract symptoms; EPIC = European Prospective Investigation into Cancer and Nutrition; IPSS = international prostate symptom score; EpiLUTS = Epidemiology of LUTS; MrOS = Osteoporotic Fractures in Men Study; ED = erectile dysfunction; PCP = primary care providers; PSA = prostate-specific antigen; BPH = benign prostatic hyperplasia; RCT = randomized controlled trial; PCPT = Prostate Cancer Prevention Trial; QOL = quality of life; HRQoL = health-related quality of life; EjD = ejaculatory dysfunction; PDE5-Is = phosphodiesterase type 5 inhibitors; IIEF = International Index of Erectile Function; AUR = acute urinary retention; ABs = alpha blocker; 5-ARI = 5-alpha reductase inhibitor; PVR = postvoid residual urine; SMP = self-management program; POR = prevalence odds ratio; BMI = body mass index.
Bold fonts indicate the article that was included in another area for review.
The Prevalence of LUTS
International studies provide a worldwide perspective of the prevalence of LUTS. In the European Prospective Investigation into Cancer and Nutrition (EPIC) study, a multinational population-based survey conducted in Canada, Germany, Italy, Sweden, and the United Kingdom in 2005, 62.5% of men reported at least one LUTS, and more than 6% of men reported having moderate-to-severe LUTS (Irwin et al., 2009). In a population-representative Epidemiology of LUTS (EpiLUTS) study that surveyed 14,139 men from the United States, United Kingdom, and Sweden via the Internet, 72.3% reported at least one LUTS (Coyne et al., 2009b). A cross-sectional, population-representative, Internet-based study conducted in mainland China, Taiwan, and South Korea in 2015 reported that LUTS prevalence was 62.8% in men older than 40 years of age (Chapple et al., 2017). In Brazil's first nationwide epidemiological study of LUTS, the prevalence of LUTS in men was reported to be 69%, with 21% of them reporting moderate-to-severe symptoms that warranted treatment consideration (Soler, Gomes, Averbeck, & Koyama, 2017). Similarly, 19.2% to 25.1% reported moderate-to-severe LUTS in a population-based survey of 4,979 men living in four urban areas from Netherlands, France, United Kingdom, and South Korea (Boyle et al., 2003). In another population-based survey of 8,700 men in Denmark, the prevalence of moderate-to-severe LUTS was 28% (Nørby, Nordling, & Mortensen, 2005). Based on the EPIC study and the U.S. Census Bureau International Data Base, it was estimated that 1.9 billion individuals of the worldwide population (45.2%) were affected by LUTS in 2008, and 2.3 billion in 2018 (44.7% of men). The increasing cases of LUTS were mostly seen in developing regions in African, South America, and Asia (Irwin et al., 2011).
Several studies of the prevalence of LUTS were carried out in the United States and reported that the prevalence was 18.7% to 98% in American men, depending on age and the level of severity (Litman et al., 2007; Taylor et al., 2006). The prevalence of LUTS increases by age. In the 2002–2005 Boston Area Community Health (BACH) Survey, 2,301 American men aged 30 to 79 years were surveyed, and 18.7% reported experiencing LUTS (Litman et al., 2007). Glasser, Carson, Kang, and Laumann (2007) studied 901 men aged 40 years and older and reported a 28% overall prevalence of LUTS. In a study of 448 men aged 51 and older, 42% of the men reported moderate-to-severe LUTS (international prostate symptom score [IPSS] > 7; Naslund et al., 2007). In the Third National Health and Nutrition Examination Survey (1988–1994), 59.9% of men aged 60 to 69 years and 75.1% men aged 70 and older reported having LUTS (Platz, Smit, Curhan, Nyberg, & Giovannucci, 2002). In the 2002 Osteoporotic Fractures in Men Study of 5,284 men aged 65 years and older without a cancer history, 98% of the men reported LUTS, with 39.6% moderate and 6.6% severe LUTS (Taylor et al., 2006).
The increase of LUTS prevalence by age has also been reported worldwide (Coyne et al., 2009a; Speakman, Kirby, Doyle, & Ioannou, 2015), and this is associated with enlarged prostate gland—BPH. More than 50% of men aged of 51 to 60 years and 70% or more of the men older than 60 years have BPH (Berry, Coffey, Walsh, & Ewing, 1984; Wei, Calhoun, & Jacobsen, 2005). Of men older than the age of 60 years experiencing LUTS, 30% were due to BPH (Liatsikos, Kyriazis, Kallidonis, & Stolzenburg, 2011; McNicholas & Kirby, 2011). There are a few other sociodemographic risk factors, but many disease associations identified for LUTS. Several large survey studies in the United States did not detect racial difference in the prevalence of LUTS (Fowke et al., 2011; Litman et al., 2007; Markland, Thompson, Ankerst, Higgings, & Kraus, 2007; Platz et al., 2002). However, in the 2002–2005 BACH Survey, the 5-year incidence of moderate-to-severe LUTS (IPSS > 7) in 1,610 men was significantly lower in Whites (7%) than other racial groups (13%; Maserejian et al., 2013a), mirroring the Prostate Cancer Prevention Trial report that African American and Hispanic men had a significantly higher rate of BPH than White men (Kristal et al., 2007). Fowke et al.'s (2011) study showed that low income was significantly associated with the prevalence of LUTS, but having private insurance was associated with a lower risk of LUTS. Other risk factors for LUTS/BPH have also been identified, including genetics, childhood nocturnal enuresis, sex steroid hormones, modifiable lifestyle factors, and inflammation (Coyne et al., 2009a; Parsons, 2010). This suggests a broader genetic-environment interaction related to LUTS and other diseases. International studies have shown that LUTS are associated with a wide range of comorbid conditions, including arthritis, asthma, chronic anxiety, depression, diabetes, heart disease, irritable bowel syndrome, neurological conditions, recurrent urinary tract infection, sleep disorders, and vitamin D deficiency (Coyne et al., 2009a; Litman et al., 2007; Vaughan et al., 2011).
Symptom clusters of LUTS were reported in a few studies. In the EpiLUTS study, 47% of men had LUTS from more than one symptom category, with voiding + storage + postmicturition symptoms as the largest subgroup (24.3%) and storage + postmicturition symptoms as the smallest subgroup (2%; Coyne et al., 2009c). In a U.S. population-based study, “Male Attitudes Regarding Sexual Health,” 2,173 American men reported the prevalence of storage (13%) and mixed (9%) symptoms higher than that of voiding symptoms (6%; Glasser et al., 2007). Nocturia has been reported as the most common symptom in several studies worldwide (Coyne et al., 2008; Irwin et al., 2009; Platz et al., 2002; Rohrmann, Katzke, & Kaaks, 2016).
LUTS progressively worsens over time. In the BACH Survey of men aged 30 to 79 years, 1 in 10 men in this age range newly developed LUTS over 5 years, with an 8.5% increase in men from no-to-mild LUTS at baseline, to moderate-to-severe LUTS in 5 years (Maserejian et al., 2013a). In the 2002–2007 California Men's Health Study of 9,640 men aged 45 to 69 years, 3,993 men (41%) had changed from no-to-mild LUTS to moderate-to-severe LUTS at a 4-year follow-up, and only 9% of them received a medical treatment for LUTS (Wallner et al., 2015). This is the same trend observed in a large cohort of European men (N = 8,627) of 48 to 79 years of age, of whom 24.7% had moderate-to-severe LUTS at baseline, but 54.8% reported worsening LUTS over a 3-year period (Rohrmann et al., 2016).
Burden of LUTS
Data from the 2005 EPIC study surveying 19,165 adults in 5 countries showed that symptom bother significantly increased by the number of LUTS experienced (Irwin et al., 2009). Urgency and urge incontinence were commonly reported to be bothersome; nocturia also topped the list (Agarwal et al., 2014; Coyne et al., 2009b; Fujimura et al., 2011).
Symptom burden of LUTS is widespread and significant. Coyne et al. (2009c) surveyed 14,139 men in the United States, United Kingdom, and Sweden (the EpiLUTS study) and reported that 35.9% of men with LUTS have clinically diagnosable anxiety, and 29.8% have clinically diagnosable depression. Rom, Schatzl, Swietek, Rücklinger, and Kratzik (2012) detected a significant association between LUTS and various levels of depression in a sample of 673 healthy Austrian men. Other studies from France (Fourcade et al., 2012), Norway (Haltbakk, Hanestad, & Hunskaar, 2005), and Brazil (Perchon, Pintarelli, Bezerra, Thiel, & Dambros, 2011) reported a significantly diminished QOL in men with LUTS. The quality of sexual life significantly worsened. The EpiLUTS study data showed that leaking urine during sexual activities was the most frequently reported bothering symptom by 82% of participants (Coyne et al., 2009b) and that men with multiple LUTS had more severe erectile dysfunction and more frequent ejaculatory dysfunction and premature ejaculation (Wein et al., 2009). Other international and multinational survey studies confirmed associations between LUTS and poor quality of sexual life (Chitale, Collins, Hull, Smith, & Irving, 2007; Rosen et al., 2003).
LUTS places a tremendous economic burden on society (Speakman et al., 2015). The 2006 U.S. National Health and Wellness Survey data showed that LUTS is significantly associated with increasing emergency room visits, doctor visits, and hospitalizations (odds ratios: 1.57, 1.52, and 1.56, respectively), as well as greater loss of work productivity (8.03%) than normal controls (Kannan, Radican, Turpin, & Bolge, 2009). Evidence has shown that QOL in the caregivers and partners of men with LUTS was impaired (Gotoh et al., 2009; Marklund, Spångberg, & Edéll-Gustafsson, 2014). It was estimated that BPH alone cost $1.1 billion annually in 2000 in the United States (Wei et al., 2005). The cost can be much higher today, especially when all causes of LUTS are considered (Physicians Practice, 2008). Clearly, LUTS have become a public health concern and require effective management.
Standard Medical Treatments and Effectiveness
LUTS have multiple pathological causes involving abnormal function in prostate, bladder, and urethra; neurological diseases; inflammation; and metabolic syndrome (Soler et al., 2013). Accordingly, a variety of medical treatments, including medication, surgery, minimally invasive procedures, and neuromodulation therapy are used to treat LUTS.
The combination therapy of alpha blockers (ABs) and 5-alpha reductase inhibitors (5-ARIs) is the first-line treatment of LUTS due to BPH. McNicholas and Kirby (2011) systematically reviewed 63 published studies and reported that ABs improved peak urinary flow significantly and 5-ARI relieved LUTS. The use of phosphodiesterase type 5 inhibitors alone or with ABs was shown to be safe and more effective than placebo in treating LUTS due to BPH (Gacci et al., 2016; MacDonald et al., 2018; Silva, Silva, & Cruz, 2014). Dahm et al. (2017) reviewed 43 clinical trials of newer drugs, including phosphodiesterase type 5 inhibitors, and concluded that traditional ABs treatment produces superior outcomes to the newer drug or drug combination because of a similar effectiveness but fewer side effects. Mirabegron is a new drug that treats urinary storage symptoms. A recent systematic review and meta-analysis evaluated eight clinical trials that compared mirabegron with placebo or tolterodine. Mirabegron was found to be an effective treatment for overactive bladder, with a slightly (nonsignificant) increased risk of side effects (Sebastianelli et al., 2017).
Despite their effectiveness, medications of LUTS were frequently reported for their side effects on cardiovascular events, higher Gleason score grade, depression, and particularly, erectile dysfunction (Gacci et al., 2014; Traish, Mulgaonkar, & Giordano, 2014). Based on two large clinical trials, the Prostate Cancer Prevention Trial and the Reduction by Dutasteride of Prostate Cancer Event, the U.S. Food and Drug Administration warned consumers in 2011 that 5-ARIs might increase the risk of high-grade prostate cancer, despite that they reduced the risk of low-grade (Gleason score ≤ 6) prostate cancer (Food and Drug Administration, 2011). Further, a 2003 survey of 1,275 U.S. physicians indicated that patients with BPH underreported treatment drug side effects, with 19% reporting to urologists and 24% to primary care providers (Seftel, Rosen, & Kuritzky, 2007). Moreover, patient compliance with medication treatment is poor. A study of 1.5 million American men with BPH reported the 1-year adherence rate at 29% (Cindolo et al., 2015). Evidence from international communities also suggests that two thirds of newly diagnosed BPH patients with LUTS discontinue medication within 12 months (Koh, Cho, Kim, & Kim, 2014) and a 4-year adherence rate at 19% (Masumori, Hashimoto, Itoh, Tsukamoto, & The Sapporo Medical University Naftopidil Study Group, 2007).
When medication treatment fails, surgical procedures are considered. Transurethral resection of the prostate remains the gold standard approach for BPH, but various minimally invasive treatments have been used to treat LUTS, including transurethral and transrectal alternative and laser-based treatments. Based on a systematic review of the literature, Liatsikos et al. (2011) concluded that such minimally invasive treatments had comparable efficacy and minimal side effects and thus increasing popularity among patients. Further, Yamanishi, Kaga, Fuse, Shibata, and Uchiyama (2015) reviewed evidence of neuromodulation therapy of LUTS, including pelvic floor electrical stimulation, interferential therapy, magnetic stimulation, and percutaneous tibial nerve stimulation and sacral nerve stimulation across gender. They acknowledged an initial evidence for the superiority of these treatments over placebo and also urged further research of their effectiveness relative to other conservative treatments. Biester et al. (2012) reviewed 43 mainly low-quality clinical trials that compared standard surgery (e.g., transurethral resection of the prostate) with nonstandard treatments (e.g., laser ablation, interstitial laser coagulation, transurethral microwave therapy, and transurethral needle ablation). They concluded that these nonstandard treatments were not superior for symptom reduction, but holmium and thulium laser resections of the prostate might have an additional benefit to patients. Tennvall, Hjelmgren, and Malmberg (2006) reported that microwave thermotherapy (ProstaLund Feedback Treatment) was cost-effective after 5 years of the treatment in comparison with alpha-blockade drug therapy. In view of a moderate utility of minimally invasive treatments and low compliance for medication treatment, it would be prudent to consider alternative treatments of LUTS.
Alternative Treatments of LUTS Worldwide
Lifestyle
One of the main alternative approaches to treating LUTS is to enhance patient self-management of LUTS through lifestyle modification. Two well-designed clinical trials were carried out. In the United States, Burgio et al. (2011) randomized 143 men who continued to have overactive bladder symptoms after a 4-week AB run-in to a behavioral treatment (pelvic floor muscle exercise [PFME], urge suppression, and delayed voiding; n = 73) or drug therapy (n = 70) over 8 weeks. Both groups continued AB therapy throughout the trial and showed a significant reduction of voiding episodes without detectable difference, while the behavioral treatment group showed more reduction in nocturia, and the drug therapy group showed more reduction in urgency. In the United Kingdom, a clinical trial was carried out to assess a behavioral intervention to lifestyle factors (e.g., fluid intake) and behavioral techniques (e.g., bladder training) among 140 men with LUTS. It was reported that the behavioral intervention plus standard care group (n = 73) had significantly higher voided volume by 57 ml, lower frequency of daily voids (by 2.6) and nocturnal episodes (by 0.7), less severe urinary symptoms, and better QOL than a standard care group (n = 67) over 12 months (p < .01 for all; Brown & Emberton, 2009; Yap, Brown, Cromwell, Van Der Meulen, & Emberton, 2009).
More supporting evidence emerged from international studies that had relatively less methodological rigor. Reports from two studies (one was randomized and another was case-controlled) of 222 and 406 Chinese LUTS patients, respectively, showed evidence that a brief behavioral intervention consisting of PFMEs, fluid intake, and bladder training techniques resulted in a significant reduction of self-reported LUTS over a period of 3 to 12 months when compared with standard care (Chen et al., 2012; Choi et al., 2015). In a single-group study of 56 Japanese subjects (including 47 men and 9 women), a lifestyle modification requiring restricted fluid intake, moderate exercise, keeping warm in bed, and restrictive bed hours led to a significant reduction of nocturnal urine volume, from 923 to 768 ml, with an average reduction of one nocturia episode per night (Soda et al., 2010). Shafik and Shafik (2003) found a significant association between PFMEs and declined detrusor pressure in a small sample of 28 Egyptian men and women, lending support for the PFME effect on overactive bladder. Further, de Jong, Pinckaers, ten Brinck, à Nijeholt, and Dekkers (2014) conducted a systematic review of 11 published studies and reported that a sitting position is better than standing position in improving urodynamic parameters such as low postvoid residual volume in men with LUTS, although it made no difference in healthy men.
Physical activity and weight loss
Studies highlighted physical activity as an important lifestyle factor. Fowke et al. (2013) reported a significant association between physical activity and lower LUTS severity, with a strong association among the obese in a cross-sectional analysis of 405 cancer-free American men with LUTS. Wolin et al. (2015) used National Cancer Institute-sponsored Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial data to examine associations between levels of physical activity and self-reported LUTS. They found that men who were physically active 1 hour or more weekly were 13% less likely to report nocturia—a significant bothersome symptom—and 34% less likely to report severe nocturia, when compared with men who were physically inactive.
Evidence on a weight loss intervention, however, was inconclusive. Khoo et al. (2014) tested an intervention of a 12-week reduced fat diet among 45 Singapore men and reported that a 10% weight loss was significantly associated with less self-reported LUTS. Yee et al. (2015) tested a weight loss program focusing on weight reduction and medical nutrition among 130 men in Hong Kong. They found no significant difference in weight difference or self-reported LUTS between the intervention and control groups over 48 weeks.
Dietary nutrition
Much research attention has been given to supplements and nutrition. In a randomized controlled trial that tested daily use of 1,500 mg of dried, powdered cranberries over 6 months in 42 Czech Republic men, investigators found that the intervention group (n = 21) reported significantly less LUTS and better QOL than the control group (n = 21), with 70% of the intervention participants showing a significant improvement in urinary flow rate, bladder voiding, and postvoid residual volumes based on uroflowmetry measurements (Vidlar et al., 2010). In a nonrandomized study of Italian men using 120 mg of a standardized cranberry extract (Anthocran) daily for 60 days, it was found that the intervention group (n = 23) significantly reduced the number of urinary tract infection episodes (from 3.2 to 0.8; p < .05) during the intervention compared with the control group (n = 21; from 3.1 to 2.1; Ledda et al., 2016). In a randomized double-blind trial of 96 American men with LUTS, men taking 240 ml of 100% grape juice daily for 3 months (n = 47) showed no significant difference in LUTS compared with men in the control group (n = 49; Spettel et al., 2013). However, in the BACH study, citrus juice intake was found to be significantly associated with a 50% lower chance of LUTS progression in men, while greater coffee or baseline total caffeine intake significantly increased the chance of LUTS progression (Maserejian et al., 2013b).
In an analysis of 1,388 male participants of the 2005–2006 National Health and Nutrition Examination Survey, vitamin D deficiency was associated significantly with the presence of moderate-to-severe urinary incontinence and a symptom of LUTS (Vaughan et al., 2011). Espinosa and coworkers (Espinosa, 2013; Espinosa, Esposito, Kazzazi, & Djavan, 2013) concluded that a heathy level of vitamin D was associated with a decrease of prostate volume and a lower risk of BPH, based on a literature review. Moreover, in the BACH Survey, dietary intakes of carotenoids and vitamin C (not supplements) were associated with a significantly lower chance of LUTS in men (Maserejian, Giovannucci, McVary, & McKinlay, 2011).
There was a debate over the effectiveness of saw palmetto (Serenoa repens) in the past decade. Following initial evidence of Cochrane meta-analysis in favor of saw palmetto on treating LUTS, especially nocturia (Tacklind, MacDonald, Rutks, & Wilt, 2009; Wilt, Ishani, & MacDonald, 2002), two randomized controlled clinical trials were published in the New England Journal of Medicine (Bent et al., 2006) and JAMA (Barry et al., 2011), followed by an updated Cochrane meta-analysis (Tacklind, MacDonald, Rutks, Stanke, & Wilt, 2012), all of which reported that saw palmetto was not superior to placebo in treating LUTS, including nocturia. In addition, the use of pumpkin seed (Cucurbita pepo) has been studied for treating LUTS. A systematic review evaluated 16 studies of pumpkin seed and reported an improvement of LUTS in all studies, and QOL in four studies (Damiano et al., 2016). The results are promising, but further clinical trials are recommended for confirming these findings.
Acupuncture
Evidence supports the use of acupuncture. Zhang, Ma, Bauer, Liu, and Lu (2017) reviewed eight randomized clinical trials that compared acupuncture with controls, placebo/sham acupuncture, or other treatments over 4 to 6 weeks. Acupuncture significantly reduced the severity of LUTS in the short term, but its clinical significance and long-term effect required further research (Zhang et al., 2017). Other studies reported that reflexology significantly reduced nocturnal frequency and micturition, with a 4-point deduction on IPSS in the treatment group when compared with the control group (Ricci, Minardi, Romoli, Galosi, & Muzzonigro, 2004; Wang et al., 2013).
Conclusions and Suggestions for Future Direction
A decade of accumulated evidence has shown that LUTS is prevalent worldwide and affects men's QOL significantly. Medication treatment is effective but often compromised by poor compliance due to undesired side effects. Minimally invasive procedures and neuromodulation therapy have emerged but are not without side effects and have yet to be accepted widely.
Behavioral treatment is a promising approach to LUTS, especially when combined with medical treatments. Some clinical trials have shown the effectiveness of behavioral interventions to boost physical activity, as well as dietary nutrition such as vitamins C and D and certain fruit juices, resulting in a reduction of LUTS. Other studies have found some efficacy in nurse-led lifestyle modifications (e.g., adherence to medication, PFME, fluid restriction, and bladder training) for LUTS reduction. Two well-designed clinical trials involving lifestyle modifications provided opposing results: One from the United States showed little evidence of the effectiveness of lifestyle modification relative to medication, but another trial from the United Kingdom showed a significant improvement in urinary measures in comparison with standard care. However, the majority of published studies involving lifestyle modification in the treatment of LUTS had methodological deficiencies, such as a small sample size, not randomized or controlled with a comparison group, or the intervention procedure was not reported as manualized or closely monitored. Many studies were conducted in different parts of the world, making it difficult to compare or interpret their results. Therefore, while some evidence of behavioral interventions is promising, the evidence of interventions to all-around lifestyle modification is at present slight and cannot be generalized across populations, times, and regions. Furthermore, specific mechanisms of such behavioral interventions to LUTS have not been studied.
The current state-of-the-art science of behavioral treatments for LUTS suggests that well-designed, randomized, and controlled longitudinal clinical trials with a large sample size are needed to systematically examine the effect and mechanisms of behavioral interventions to lifestyle factors in comparison with standard care. Such clinical trials need to carefully evaluate the added benefits of behavioral management and the magnitude of the effect, be rigorous in the behavioral intervention programs that incorporate evidence-based therapeutic components, be mindful of implementability of the behavioral intervention programs to be generalizable across clinical or community settings, and consider using technology to reach out to a diverse population of men with LUTS and empower them for better urinary health. With this effort, it is hopeful that we will identify an effective solution to the management of LUTS to improve men's QOL and reduce its societal burden in the United States and the world.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.