
Abstract
Objective:
Most multiple sclerosis patients have urological complications such as lower urinary tract symptoms. This study was conducted to evaluate the prevalence of these symptoms and whether they result in a urological evaluation.
Methods:
A cross-sectional study of 517 multiple sclerosis patients at Tehran’s referral multiple sclerosis center and neurology clinics between 2018 and 2022 was performed. Data were collected through interviews after patients completed informed consent forms. Urological examinations, including urine analysis and ultrasonography, were evaluated as final assessments. The data were analyzed using descriptive and inferential statistical tests in Statistical Package for Social Science.
Results:
Among all participants, the prevalence of lower urinary tract symptoms was 73% (n = 384), with urgency (44.8% n = 232) being the most common symptom. The prevalence of intermittency was significantly higher among women (p = 0.004). There was no gender-significant difference in terms of the prevalence of other symptoms (p > 0.050). Lower urinary tract symptoms were significantly correlated with age, clinical course, disease duration, and disability (p < 0.001). Additionally, 37.3% and 18.7% of patients with lower urinary tract symptoms, as well as 17.9% and 37.5% of patients with multiple sclerosis attacks, respectively, had undergone urine analysis and ultrasonography.
Conclusion:
Multiple sclerosis patients rarely undergo urological evaluations during the course of their disease. Proper assessment is essential as these symptoms are among the most detrimental manifestations of this disease.
Introduction
Multiple sclerosis (MS) is an autoimmune, progressive disease caused by demyelination and axonal degeneration of the central nervous system (CNS). 1 Global prevalence of MS has increased from 29.26 in 2013 to 43.95 in 2020 per 100,000, according to a worldwide study. 2 The pooled incidence rate in 75 countries is 2.1 cases per 100,000, with a mean age of 32 years at diagnosis. 2 According to the results of a recent study, the prevalence of MS in Iran has been estimated to be 100 per 100,000. 3
Typical plaque formation in the pathogenesis of MS results in neurogenic lower urinary tract dysfunction (NLUTD). 4
Between 48% and 92% of patients with MS experience lower urinary tract disorders (LUTDs). 5
These symptoms are generally manifested 6 years following the onset of neurological symptoms but can also appear at the time of MS diagnosis in approximately 10% of cases. 6
Urological disorders are among the most detrimental social manifestations of MS. 7 Up to 70% of patients report bladder symptoms to be a “high” or “moderate” burden on their lives and are regarded as the major cause of morbidity and financial burden in this population. 7
Patients with LUTD commonly experience incontinence and difficulty voiding, which may necessitate self-catheterization. 8 Sensory impairment, urinary stasis, and catheter use are associated with an increased risk of urinary tract infections (UTIs), which may exacerbate the progression of the disease or mimic a flare-up.9,10
Identifying potential LUTD or infection at an early stage provides protection for the upper urinary tract, improves treatment, and enhances the quality of life. 8 In spite of the high prevalence of urinary disorders, urological examinations and treatments are not regularly conducted. 11
This study aims to determine the prevalence and clinical characteristics of LUTDs in patients affected by MS and investigate whether these disorders have led to any urological assessment.
Materials and methods
This cross-sectional study evaluated 517 MS patients at Tehran’s referral MS center and neurology clinics between 2018 and 2022. Participants were required to meet the following criteria to be included in this study: A minimum age of 18 years, MS diagnosis based on McDonald’s criteria, 12 clinical stability (no flare-ups in prior 3 months, or worsening of disabilities, defined as an increase of one point (if baseline Expanded Disability Status Scale (EDSS) 13 score was <5.5) or 0.5 points (if baseline EDSS score was ⩾5.5) confirmed 6 months apart and sustained at the end of the follow-up period), lack of urinary symptoms before MS diagnosis. The exclusion criteria were as follows: Preexisting urinary symptoms before MS diagnosis, a history of surgery or radiotherapy in the pelvic area, benign prostatic hyperplasia or prostate surgery, History of MS attacks within the previous month and corticosteroid use, and less than 6 months of clinical follow-up.
As demographic and clinical characteristics, age, sex, education, age at MS diagnosis, disease duration, clinical course ((relapsing-remitting multiple sclerosis (RRMS), primary-progressive multiple sclerosis (PPMS), secondary-progressive multiple sclerosis (SPMS), CIS (clinically isolated syndrome)), disability, and LUTS prevalence were considered.
As defined by the International Continence Society, urinary symptoms are classified as follows: voiding (weak stream, split stream, intermittent flow, hesitancy, straining, and terminal dribbling), storage (frequency, nocturia, urgency, urge incontinence, stress incontinence, leakage, nocturnal enuresis), postmicturition (incomplete voiding or postmicturition incontinence), or other (dysuria) symptoms (Table 1).14,15
The prevalence of urinary symptoms based on patient’s characteristics.
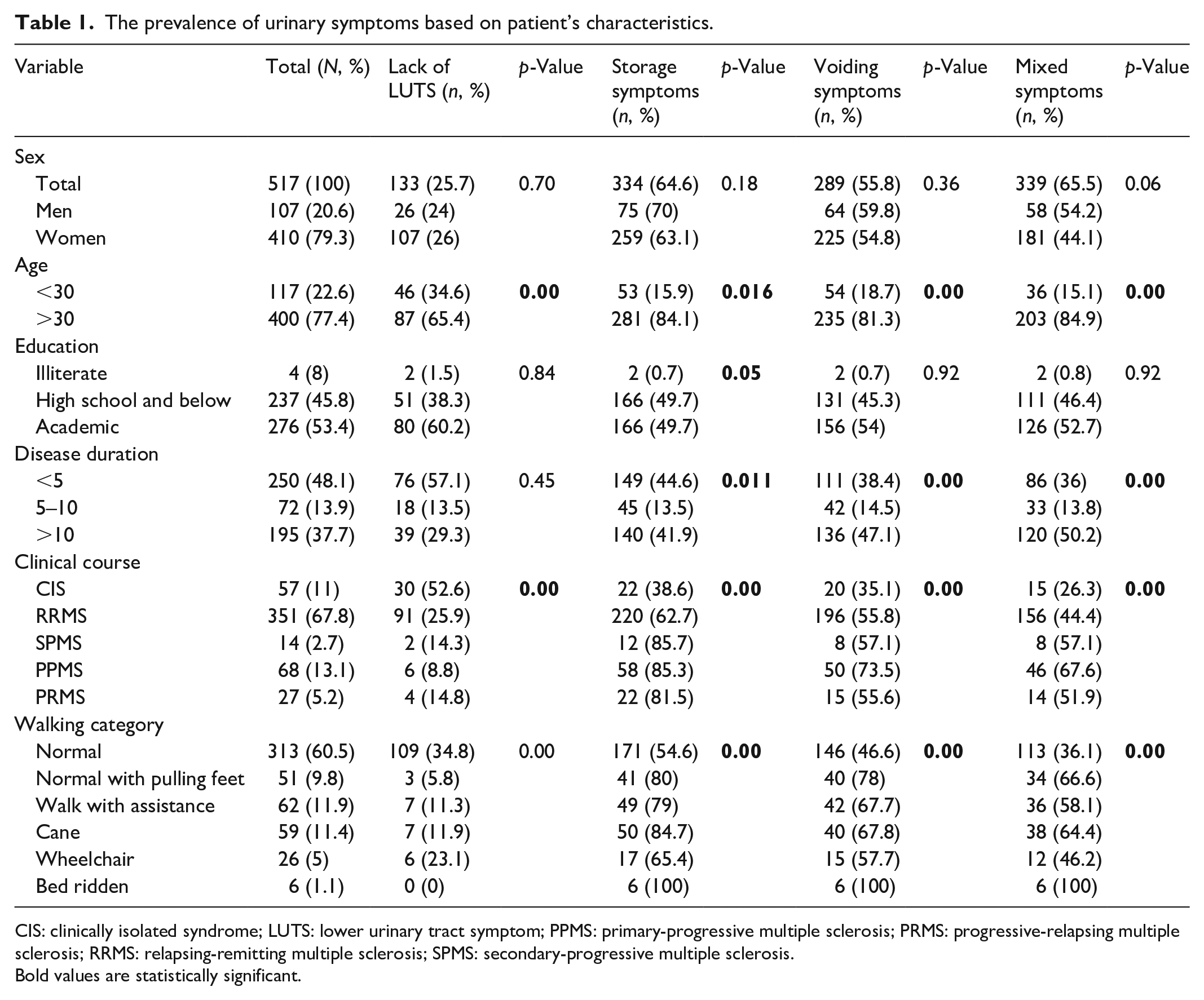
CIS: clinically isolated syndrome; LUTS: lower urinary tract symptom; PPMS: primary-progressive multiple sclerosis; PRMS: progressive-relapsing multiple sclerosis; RRMS: relapsing-remitting multiple sclerosis; SPMS: secondary-progressive multiple sclerosis.
Bold values are statistically significant.
The International Consultation on Incontinence Questionnaire short-form questionnaire, 16 was used to assess the presence and frequency of LUTS in our patient cohort. The questionnaire has been validated and widely used in clinical and research settings to evaluate urinary symptoms and quality of life. In addition to the questionnaire, a trained research center staff member conducted individual patient interviews to further assess and clarify the presence and characteristics of LUTS. The interviews were conducted in a private setting, with a standardized script to ensure consistency across patients. The staff member was trained and supervised by a urologist to ensure a proper understanding of LUTS and the protocol for conducting the interviews. Participants filled out informed consent forms after ensuring their decisional capacity. For illiterate individuals, written informed consent was taken from their legally authorized representatives. As part of the final assessment, urological examinations, including urine analysis (U/A) and ultrasonography, were evaluated.
The Ethics Committee of the Shahid Beheshti University of Medical Sciences’ Urology and Nephrology Research Center approved all procedures involving human participants in the study with number: IR.SBMU.UNRC.1397.4
The single population proportion formula was used to estimate the required sample size. (n = (Za/2) 2 p(1 − p)/d2), with the assumptions of Z = 1.96, confidence interval = 95%, a margin of error (d = 0.05), and the proportion of MS (p = 0.12) from the study done in Iran. 17 The total sample size was 517 after subtracting 10% of the no retrieval rate. The statistical analysis was performed using the “Statistical Package for Social Science (SPSS)” program. Continuous variables are represented as mean ± Standard Deviation, while categorical variables are represented as frequencies. The chi-square (χ2) test and independent t-test were used for statistical analysis. A p-value of <0.05 was considered statistically significant.
Results
Study population
Among the 517 patients, 410 (79.3%) were females, and 107 (20.7%) were males. The mean age was 37.9 ± 9.5 years, while the mean age at the MS diagnosis was 27.7 ± 9.6 years. As expected, the majority of patients were female (79.3%). The most common clinical phenotype was RRMS (66.7%, n = 351), followed by PPMS (12.9%, n = 68). The demographic data were shown in Table 1.
Urological disorders
Overall, 73% of participants (n = 384) had urological symptoms. The most prevalent symptom was urgency (44.8%, n = 232), followed by frequency (43.5%, n = 225) and feeling of incomplete voiding (40.4%, n = 209). Women had a higher prevalence of urinary intermittency (p = 0.004). Tables 1 and 2 summarizes data on individual symptoms and pattern.
Lower urinary tract symptoms.

Bold values are statistically significant.
According to the findings, mixed symptoms (combination of storage and voiding symptoms) were the most prevalent (65.5%), followed by storage and voiding symptoms at 64.6% and 55.8%, respectively. Moreover, 26% of women and 24.2% of men were free of urinary symptoms. Based on the Chi-square test, no statistically significant differences were found between the two groups regarding urinary symptoms (Tables 1 and 2). A significant difference was found in the prevalence of urinary symptoms between individuals of different ages and with varying clinical courses and disease durations (Tables 1 and 2).
There was a significant increase in urinary symptoms among patients with older age at the time of evaluation, longer disease durations, and progressive forms of the disease (p < 0.001) (Table 1).
Among patients with urinary complaints, 129 (37.3%) were assessed by U/A while 64 (18.7%) were examined by ultrasound. In the group of patients who have experienced MS attacks, 157 (37.5%) had U/A performed while 75 (17.9%) had undergone ultrasound (Table 3).
Inter-pattern chi-square analysis of urinary symptoms and MS attack with urological assessment.

U/A: urine analysis; MS: multiple sclerosis.
Discussion
As is well known, MS is characterized by a multifocality of demyelinating lesions and varied clinical manifestations.18,19 A high prevalence of urological disorders affects these patients and is detrimental to their quality of life. 7
Over half of the 517 patients with MS in our study reported urological symptoms during assessment. There was a higher prevalence of urological disorders among older individuals, with longer disease duration, progressive clinical course, and greater functional disability. A study by Seddone et al. 20 found a 52.9% prevalence of LUTS, compared to a 92% by Khalaf et al. 11 and an 87.6% prevalence in a study by Nazari et al. 21
There was an insignificant higher prevalence of urinary symptoms among men, according to our results. The same findings were reported in the study by Sand et al., 22 where 60% of men and 50% of women reported mixed urinary symptoms. However, several studies did not find a significant correlation between LUTS incidence and gender.21,23 Accordingly, a study in the United States reported a similar prevalence among men (91.1%) and women (93.8%). 11
Over half of the participants in the present study experienced mixed symptoms, with storage symptoms being more prevalent than voiding symptoms. However, Dillon et al. 24 found that patients with MS were more likely to have voiding symptoms. According to a study conducted in Turkey, mixed urinary symptoms were more prevalent among MS patients (70%) than either storage (25%) or voiding symptoms (5%). 25 Also, according to a cross-sectional study, storage symptoms (48.2%) were more prevalent in MS patients than voiding (36.8) or postmicturition symptoms (29.9%). 26 In Western countries, storage symptoms are the most common urinary tract symptoms among MS patients, whereas, in Eastern countries, voiding symptoms predominate. 27
Our study found that storage symptoms were more prevalent than voiding symptoms without any significant gender-related differences. A cross-sectional study, however, demonstrated a higher prevalence of storage symptoms among women (23.8%) than men (12.6%). 28 Additionally, a study in Turkey found that voiding symptoms, such as urinary hesitancy, intermittency, weak stream, and feeling of incomplete voiding, occurred most often among men, whereas stress urinary incontinence (UI) was more common among women. 29 According to their study, storage symptoms did not differ significantly between men and women. 29 According to a study conducted in Japan, polyuria accounted for 94.8% of symptoms in men, followed by weak stream (92.0%), diurnal polyuria (88.2%), and urgency (70.0%). 30
In the current study, the prevalence of mixed urinary symptoms was significantly higher among patients older than 30 (55.1%) compared to patients younger than 30 (46%). The study by Chapple et al. 31 indicates a high prevalence rate of LUTS among men and women with a minimum age of 40 years and a significant increase in the prevalence of LUTS with age, ranging from 49.9% at the age of 40–44 years to 69.7% at the age of 60 or older. The study by Boyle et al. 32 found a positive correlation between LUTS and age among women, since younger men had a lower prevalence of LUTS and older men had a higher prevalence than women of the same age. The significant positive correlation between aging and urinary symptoms has also been demonstrated in other studies.33,34 These findings suggest that aging may exacerbate urinary disorders in MS patients through potentiating pathophysiological factors. 35
According to the current study, LUTS was found to be more common in patients with academic degrees than in those without an academic degree or who were illiterate; however, the difference did not reach statistical significance. In line with our study, an Austrian cross-sectional study found no significant correlation between LUTS and the level of education in men. 36 In contrast, an Iranian cross-sectional study of 602 patients found that LUTS prevalence was significantly higher among people with a lower level of education compared to those with a high school diploma or academic degree. 37
We found that storage symptoms were more prevalent in patients with shorter disease durations, whereas mixed LUTS was more prevalent in patients with longer disease durations. Furthermore, a study conducted in Brazil found a slightly positive correlation between the duration of the disease and the prevalence and severity of LUTD. 38 In a further study, it was found that disease duration and level of disability were only significantly associated with more severe urinary symptoms in women. 39 Based on data compiled by the American Research Committee on Multiple Sclerosis, the severity and prevalence of LUTS increased with disease duration. Accordingly, 32.1% of patients 0–5 years after diagnosis had LUTS, compared to 45.9% of patients with an 18-year history. 40
According to our results, although all patients were supported by officially approved foundations related to MS disease, more than 70% of MS patients had urinary symptoms. Patients who had a progressive clinical course exhibited a significantly higher prevalence of mixed LUTS. As reported by Wang et al., 41 patients with CIS had the lowest overactive bladder symptom score. According to de Almeida et al., 38 prevalence rates for RRMS and PPMS were 63.5% and 100%, respectively.
According to Khalaf et al., 42 although LUTS incidence increased with the progression of the disease, the severity or duration of disability was not related to these symptoms. Furthermore, Nakipoglu et al. 43 did not find a statistical correlation between LUTS and disease characteristics. Due to the dynamic nature of MS as well as the fact that LUTS are likely to change over time, it is imperative that patients with MS receive a regular assessment. 31
According to our study, among MS patients with urinary symptoms and a history of MS attacks, more than half had not undergone a urological evaluation, neither by a U/A nor by ultrasonography. In a study by Brucker et al., 44 lack of communication (Never asked or referred) was rated as the most significant obstacle to obtaining urological care, with finance, health insurance, distance, and transportation being less significant.
A number of studies have also reflected this sentiment, with some MS patients believing that “medical staff ignores their bladder and bowel problems.”45–47 Also, MS patients may be reluctant to seek assistance with continence issues. Due to the length of MS patient visits and the fact that bladder and bowel dysfunction is not usually a priority, assessments of urinary symptoms are time-limited. 44 It has been extensively studied that people are averse to seeking treatment for UI in general. 48 Patients fail to bring up these issues due to a variety of factors, including the severity of the symptoms and the misconception that LUTS is inevitable, incurable, and an inevitable part of the disease.48–50 Recently, a survey found that embarrassment was the main barrier to seeking medical care. 48 However, the patient usually needs to address the issue on their own. 51 Approximately 85% of women who consulted a physician about incontinence initiated the conversation. 51
MS patients are at an increased risk for UTIs. However, since these patients may have impaired sensory function and urinary tract dysfunction, UTIs may be asymptomatic.52,53 A subacute relapse or MS attack is one of the hallmark characteristics of the disease. 54 A pseudo-relapse is a type of neurologic disease worsening that is not characterized by new demyelinating activity in the CNS but rather is an old symptom exacerbated by stressors like infections, temperature changes, or fever. 55 In the case of UTIs, the “absence of infection” can be assessed differently by each physician; some will evaluate for signs of infection systematically, while others will prescribe corticosteroids without ruling out infection except by asking the patient whether they have symptoms of infection. 56 An active untreated bacterial infection may be aggravated by corticosteroids, leading to complications such as pyelonephritis and urosepsis. 56
In this cross-sectional study, certain limitations apply, including the impossibility of determining the time at which urological disorders onset, the grading of symptoms, and a correlation with neuroimaging results. According to ethical considerations due to the outbreak of coronavirus disease 2019 (COVID-19), we were not able to have the U/A of all participants. Our study involved a large collection of patients with MS, in which we found a high prevalence of urological disorders. There is evidence that these disorders may adversely affect the quality of life and may lead to further complications. All patients with MS should be examined for NLUTD, irrespective of their urological complaints. Some easy-to-collect parameters such as post-void residual, micturition frequency, UTI rate, incontinence, and uroflowmetry can complete the neurological assessment standards to ameliorate diagnosis and management of NLUTD in patients with MS. 57
Conclusion
This study describes a broad MS population with a high prevalence of LUTDs/NLUTD. Even though the prevalence of LUTDs and UI is high, many patients do not receive a urological examination, and most are not treated. Since these symptoms generally worsen with the progression of MS and the availability of treatments and prevention strategies, accurate diagnosis and treatment of LUTDs should be part of the clinical evaluation of individuals with MS. People suffering from MS should be encouraged to overcome their embarrassment and ask for help. Therefore, detection of lower urinary tract dysfunction at an early stage during the follow-up is critical for preserving the upper urinary tract, optimizing treatment, and improving quality of life.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231178047 – Supplemental material for Multiple sclerosis and lower urinary tract symptoms: A survey of prevalence, characteristic and urological evaluations
Supplemental material, sj-docx-1-smo-10.1177_20503121231178047 for Multiple sclerosis and lower urinary tract symptoms: A survey of prevalence, characteristic and urological evaluations by Farzaneh Sharifiaghdas, Behzad Narouie, Maryam Taheri, Saba Jalali, Bita Shalbafan, Mohaddeseh Azadvari, Mehdi Dadpour, Hamidreza Rouientan, Mohadese Ahmadzade and Hamideh Hanafi Bojd in SAGE Open Medicine
Footnotes
Acknowledgements
None.
Author contributions
Farzaneh Sharifiaghdas: Conceptualization, Project administration, Review & editing
Behzad Narouie: Supervision, Project administration, Review & editing
Bita Shalbafan: Conceptualization, Project administration
Mohaddeseh Azadvari: Investigation, Data curation
Maryam Taheri: Project administration, Investigation, Data curation
Saba Jalili: Supervision, Investigation, Data curation
Mehdi Dadpour: Investigation, Data curation
Hamidreza Rouientan: Writing – original draft, Methodology, Formal analysis
Mohadese Ahmadzade: Writing – original draft, Methodology, Formal analysis
Hamideh Hanafi Bojd: Investigation, Data curation, Review & editing
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval for this study was obtained from The Ethics Committee of the Shahid Beheshti University of Medical Sciences’ Urology and Nephrology Research Center approved all procedures involving human participants in the study with number: IR.SBMU.UNRC.1397.4.
Informed consent
Written informed consent had been completed by the participants after ensuring their decisional capacity. For the illiterate individuals written informed consent was taken from their legally authorized representatives.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.