
Abstract
Introduction
Behavioral Activation (BA) is a short-term cognitive behavioral therapy modality that stimulates activities that increase patients’ reinforcement experiences. Recent research verified the effect of brief BA. However, despite the short intervention time per session, BA is difficult to implement during hospitalization due to its long implementation period.
Objectives
To evaluate the clinical effectiveness of a brief BA program for people with depression in an inpatient setting.
Methods
This study employed a single-group pre-post design. Fifteen patients who met the inclusion criteria participated in the trial after providing oral and written informed consent. In addition to their usual care, participants received four weekly sessions administered by a nurse. The primary outcome measures included the Beck Depression Inventory (BDI-II), which indicated patients’ subjective depression severity. Clinical outcomes were measured at preintervention, immediate postintervention, and one-month postintervention.
Results
Fourteen participants completed the BA program and were receptive to treatment. For the primary endpoint, BDI-II, there was an improvement in scores (25.60 to 22.73 to 22.06) between the baseline, postintervention, and 1-month postassessment, but not a significant change. For EQ VAS score, there was no significant change, but there was an improvement in EQ VAS score (51.53 to 52.20 to 55.13) between the baseline, postintervention, and 1-month postassessment. The mean total Global Assessment of Functioning score increased from 40.20 to 57.00 across the pre- and postassessment points (p < .0001).
Conclusion
The study comprised a brief BA intervention, with results suggesting that participants could complete the program without feeling burdened. Although there was no significant improvement in the general outcome, depression levels, and other outcomes improved. Thus, while there is a need to rethink BA intervention, this program may be a practical approach to improving depression and other outcomes.
Keywords
Introduction/Background
The number of cases of depression has increased from 172 million in 1990 to 258 million in 2017, an increase of about 50% (Liu et al., 2000). The World Health Organization states that depression is a leading cause of mental and physical disability worldwide and a major contributor to the global burden of disease (World Health Organization, 2021). In a Japanese government survey, more than one million people with depression are receiving active treatment in Japan (Ministry of Health, Labour and Welfare, 2022). In Japan, the increase in depression has caused several social problems, including labor shortages and increased suicide rates (Ozaki, 2022). Thus, it is necessary to address critical issues related to depression urgently.
Individuals with depression often experience hopelessness (e.g., thoughts such as “I think I am not a person of value”) and tend to have negative thinking that leads to guilt; therefore, they are frequently affected by their internal emotional state. Therefore, European guidelines recommend cognitive-behavioral therapy (CBT) as the initial treatment for mild depression, which treats internal feelings (National Institute for Health and Care Excellence, 2022). Similarly, recent trends in Japan have indicated that CBT is the first treatment choice for mild to moderate depression. Cognitive behavioral therapy is implemented in various ways, with numerous experimental studies reporting significant treatment effects (Mathiasen et al., 2022; Stuart et al., 2022) and decreased medical costs (Pahlevan et al., 2020). With the expected effectiveness of CBT, it has become the mainstream treatment of choice as the first treatment for mild to moderate depression in Japan. In Japan, basic CBT for depression consists of 16 sessions completed over 2–3 months (Ministry of Health, Labour and Welfar, 2009). In Japan, currently, the average length of hospital stay is 42.6 days for mood (affective) disorders and 27.7 days for neurotic, stress-related, and somatoform disorders (National Federation of Health Insurance Societies, 2021). Because of the difficulty of completing CBT during the hospitalization period, structured CBT is generally administered on an outpatient basis. However, considering that depressive symptoms may worsen due to changes in the environment after discharge, it is important to conduct CBT during hospitalization. However, with the current number of sessions, it is not easy to complete CBT during hospitalization.
Nurses are expected to play a major role in practicing CBT due to their ability to provide total care, including physical management, medication guidance, psychological care, daily living support, and utilization of social resources. In practice, when compared to doctor-led CBT, advanced practice registered nurse (APRN)-led CBT is beneficial for clinical and service-related outcomes, including patient satisfaction, wait times, chronic disease management, and cost effectiveness (Htay & Whitehead, 2021). However, this report was limited to well-educated APRN-led CBT practices. Cognitive behavioral therapy is complex because training and employing nurses to administer the therapy is expensive; thus, many nurses want to implement CBT but are unable to as they feel that it is challenging.
Therefore, two challenges must be faced: ensuring the quality of CBT practiced by nurses and minimizing the number of sessions to complete CBT during hospitalization. Therefore, this study focuses on behavioral activation (BA), one of the CBT techniques, and attempts to create a CBT program that can be implemented by nurses in a short period of time, which might help to prevent recurrence in depressed patients.
Review of Literature
Cognitive behavioral therapy has been shown to be as effective as medication in treating adult depression (Cuijpers et al., 2020), and it has used cognitive and behavioral techniques in combination to transform the nonfunctional cognition that is characteristically observed in depression. However, no difference has been found in effectiveness without the implementation of cognitive techniques, and the content of cognition does not mediate the improvement of depression through cognitive therapy (Burns & Spangler, 2001); thus, BA, consisting of behavioral techniques, was developed as an independent psychological support for depression. Behavioral Activation aims to stimulate activities that increase the patient's experience of receiving reinforcement (Cuijpers et al., 2020), and it can reduce depressive symptoms such as apathy, loss of pleasure, and avoidance by focusing on patients’ behaviors and positive reinforcement (Stein et al., 2021). Behavioral Activation is relatively simple compared to full CBT, and it is characterized by the fact that general counselors can provide it with less intensive and costly training (Richards et al., 2016).
Behavioral Activation for treating depression is broadly distinguished into four types (Cuijpers et al., 2019). Although these types share a common goal of improving depressive symptoms by increasing opportunities to receive positive reinforcement, their rationales and techniques differ. Behavioral Activations developed since 2000 have three common components (Lejuez et al., 2001; Martell et al., 2001). The first commonality is the focus on the reduction of avoidance behavior, where the therapist focuses on avoidance behaviors and works to decrease their activity. The second commonality is that behavioral analysis is based on functional contextualism. The therapist does not simply recommend that the patient engage in an activity susceptible to positive reinforcers; rather, they should emphasize the context in which the behavior occurs and its functional aspects and help the patient understand and work with the reinforcer entailments on their own. The third commonality is the incorporation of clarification of values and life goals to increase behaviors that are more likely to receive natural reinforcers. Natural reinforcement means that the natural consequences of behavior in the environment are the reinforcers, as opposed to arbitrary, artificially mediated reinforcement. These three components are essential to BA.
The BA protocol developed by Martell et al. (2001) often consists of 20–24 sessions, whereas that developed by Lejuez et al. (2001) is characterized as Behavioral Activation Treatment for Depression (BATD) and manualized to be implemented in a relatively short period of time. In recent years, BATD has been recognized as an independent, evidence-based treatment (Pass et al., 2018). Currently, it has a 10-session manualized protocol with Behavioral Activation Therapy for Depression – Revised (BATD-R) being developed, but the number of sessions can be reduced as needed. Behavioral Activation Treatment for Depression is characterized by its flexible format, and in recent years, it has been developed using mobile technology (Dahne et al., 2019; Moffett et al., 2022). Compared to CBT, BA can be expected to have a certain level of effectiveness without special training for counselors, and sessions can be structured in a more flexible form. In other words, BA could be adapted to inpatients whose duration of implementation is limited to a short period of time, and nurses without special training in BA could expect a certain level of effectiveness. In fact, the reports of completing BA in one to six sessions have been several (Stein et al., 2021), but they have not yet been adapted for clinical use. Therefore, in this study, three common elements of brief BA were incorporated, and a BA program was created for inpatients to be completed in four sessions. This pilot study conducts a trial on a brief BA program and validates its efficacy.
Methods
Design
This study employed a single-group pre-post design and was conducted between June 2017 and August 2018. Assessments were conducted pre-, post-, and one-month postintervention to measure clinical outcomes.
Research Questions
Can brief BA programs for inpatients reduce depressive symptoms?
Can brief BA programs for inpatients improve quality of life (QOL)?
Can brief BA programs for inpatients reduce the degree of impairment of function due to physical or environmental limitations?
Sample
Participants were recruited through psychiatrist referrals at the study site between June 2017 and June 2018 and screened via Beck's Depression Inventory (BDI). All aspects pertaining to the trial were explained to participants who met the inclusion criteria. They were then invited to provide written informed consent, their sociodemographic information, and a clinical interview. Sample size was determined using Gpower (Faul et al., 2007) as follows: the primary variable was BDI-II, and the sample size was based on a two-tailed test with significance level of 5%, a power of 80%, a correlation between groups = 0.5, and with an anticipated effect sised d = difference of means/ standard deviation = 1.19 based on a previous study (Samantha & Otto, 2017). Since the resultant required sample size was 12 cases, a target of 15 cases was set taking into account the number of potential dropouts.
Inclusion/Exclusion Criteria
Participants were psychiatric inpatients in the psychiatric ward of a general hospital. The inclusion criteria were: (1) aged 20 years and above, (2) diagnosed with a depressive disorder listed in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-V), and (3) had a BDI-II score of 12 or more. The exclusion criteria included intellectual disabilities, dementia, neurocognitive disorders, antisocial personality disorder, active suicidal intent, and alcohol or drug dependency.
Ethical Consideration
This study was conducted in compliance with the principles of the Declaration of Helsinki. The ethics committee of the Miyazaki University of Health Sciences study protocol approved this study (approval number: I-0014-2) on January 10, 2017 approved this study. It was registered with the University Hospital Medical Information Network Clinical Trials Registry (ID: UMIN000026539). All participants provided verbal and written informed consent. They were informed of the study purpose and overview, protection of privacy, freedom to withdraw at any time, data storage and processing methods, publication of results, and the researchers’ contact information. In addition, information was shared with the attending patients’ doctors so that they could respond if they felt any emotional burden during the session. In managing the data, anonymity was ensured so that individuals could not be identified.
Interventions
The BA program in this study was designed for inpatients, and their behavior was expected to be restricted in a limited environment. Therefore, it focused on discussing life goals and values and interventions toward avoidance behavior observed in BA. The final goal was to increase antidepressive behaviors. Given difficulties in selecting content for these sessions, the researchers tried to incorporate the key features of BA. Essential components of the sessions included the following theoretical goals (see Table 1 for detailed stages):
Identification of behaviors that foment patient depression. Creation of a self-monitoring chart to track activities and their impact on mood. Identification of depression loops.
Overview of the Stages of Therapy.
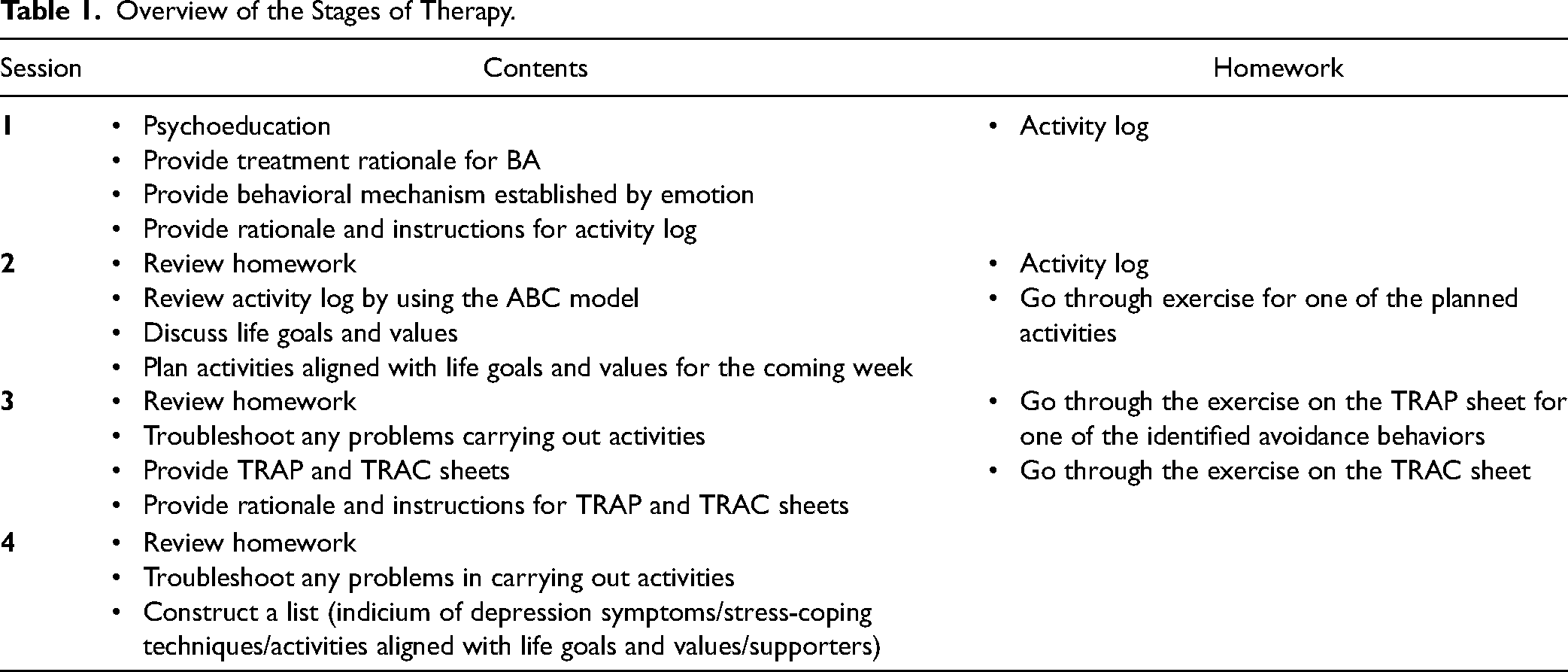
The BA program described above was provided on a weekly basis in the hospital, lasting 40–60 min per session. Therapists were nurses with at more than 3 years of psychiatric ward experience and 1–3 years of CBT training. The therapists participated in a 6-h workshop on BA to ensure treatment fidelity and discussed therapeutic difficulties and impasses with each other. Antidepressants and anxiolytics previously prescribed to patients at the baseline were continued and modified as needed throughout the study.
Outcome Measures
The self-rating scales were administered preintervention (from the time consent was obtained until the start of the first session), postintervention (at the end of the program), and one month after treatment (follow-ups). Follow-ups were conducted through mail or directly during outpatient visits. Patients’ doctors administered the objective evaluation scale (Global Assessment of Functioning [GAF]) during pre- and posttreatment. The primary outcome was depressive symptoms, and the BDI-II was used as the scale because of its ease of comparison with previous studies. The secondary outcome measures included: Quick Inventory of Depressive Symptomatology (QIDS-J), EuroQol 5 dimensions 5-level (EQ-5D-5L) questionnaire, and GAF.
Beck Depression Inventory-Ⅱ
The primary outcome measured was the participants’ subjective severity of depression, which was assessed using BDI-II, which is a self-report scale of depressive symptoms experienced in the previous two weeks. The Japanese version of BDI-II has a Cronbach's α value of .89, indicating good internal consistency (Nishiyama & Sakai, 2009). The BDI-II consists of 21 items rated on a 4-point scale (0–3 points), with total scores ranging 0–63. The severity of depression among Japanese samples is categorized based on the following BDI-II scores: 13 or less as minimal (or in remission), 14–19 as mild, 20–28 as moderate, and 29 or greater as severe. Since this study was intended to screen participants, the cutoff point was set low. Therefore, in this study, the cutoff point (12/13) was set (Lasa et al., 2000).
Quick Inventory of Depressive Symptomatology
Quick Inventory of Depressive Symptomatology is a self-report measure developed to minimize the time to appraise depressive symptom severity. The questionnaire consists of 16 items: four items related to sleep (initial, middle, and late insomnia, as well as hypersomnia), two items related to appetite/weight (appetite increase and decrease, weight increase and decrease), two items related to psychomotor state (agitation and retardation), and six additional items (sad mood, concentration, energy, interest, guilt, and suicidal ideation/intent). Each domain is rated on a score of 0–3. The QIDS-J total score ranges 0–27, classifying the severity of depression as follows: a score of 5 or less as minimal (or in remission), 6–10 as mild, 11–15 as moderate, 16–20 as severe, and 21 or greater as very severe (Rush et al., 2003). The Japanese version of QIDS has a Cronbach's α value of .86, indicating good internal consistency (Fujisawa et al., 2010).
EuroQol 5-Dimension 5-Level Questionnaire
Health-related subjective QOL was measured using EQ-5D-5L (Wailoo et al., 2021). The EQ-5D is a questionnaire evaluating QOL and is used to calculate quality-adjusted life years (QALYs), which have been increasingly used in the economic evaluation of medical technology in recent years. EuroQol 5 dimensions is roughly divided into a five-item descriptive evaluation using the Visual Analog Scale (EQ VAS). The descriptive evaluation is a self-administered questionnaire, with the health status of the five items of mobility, self-care, usual activities, pain/discomfort, and anxiety/depression evaluated on a 5-point scale (1 = no problems to 5 = extreme problems). Respondents indicate their health status by choosing statements that represent their health condition. The numbers chosen for each health condition are converted to the EQ-5D-5L Index by calculating the values distributed from −0.025 to 1.000. Higher scores are interpreted as a higher Health-Related QOL. The EQ VAS records a cross (X) mark on a scale consisting of a vertical line segment from 0 to 100 that the subject perceives as representing their health status today. One hundred represents the best imaginable state of health, and 0 the worst. This information provides quantitative health data as determined by individual respondents. The Japanese version of the EQ-5D-5L has been shown to be reliable in the general population (Hidaka et al., 2021), and the Japanese version of the EQ-5D has a Cronbach's α value of .78, indicating acceptable internal consistency (Nakano et al., 2005).
Global Assessment of Functioning
The GAF scale is useful for tracking an individual's general clinical improvement using a single measurement. It is used specifically for psychological, social, and occupational purposes, excluding functional impairment due to physical and environmental constraints. The scale is divided into 10 functional ranges 1–100, with lower levels reflecting increased impairment within the most adversely affected dimension. Assessing GAF requires selecting a singular value that best reflects the individual's overall functioning level. The scale has two components: (1) the severity of symptoms and (2) severe obstacles in social, professional, or school functioning. If an individual's symptom severity and functional level are inconsistent, the final GAF assessment will always reflect the worse level. The GAF scale is often used to evaluate the current episode of depression (Guaiana et al., 2022; Pos et al., 2019). It is further valuable to record the GAF score both before and after treatment. The reliability of GAF scores has not been examined in Japan but has proven acceptable outside of Japan under conditions where assessors are experienced and trained (Vatnaland et al., 2007).
Psychotropic Drug Usage (Chlorpromazine, Imipramine, and Diazepam-Equivalent)
The daily dose of psychotropic drug use was calculated for each antipsychotic, antidepressant, and anxiolytic drug, pre- and postintervention. Thereafter, chlorpromazine conversion values (CP-equivalent) for antipsychotics, imipramine conversion values (IMI-equivalent) for antidepressants, and diazepam conversion values (DZP-equivalent) for antianxiety drugs were calculated.
Statistical Analysis
The commonly used last observation carried forward was employed for subjects who attended at least three of the four sessions, following the intention-to-treat principle. For nonparticipants, the last data obtained were used as the endpoint assessment. Participants were considered to have dropped out if they withdrew from two or more sessions. Regarding the BDI, QIDS, EQ-5D, and EQ VAS, changes from the baseline at each visit were analyzed using repeated ANOVA and Tukey's HSD test. The remission cutoff point was defined as an endpoint BDI-II score of 13 or less (Hiroe et al., 2005), and the therapeutic response as a 50% reduction in BDI-II scores (Bech et al., 2000). Regarding the QIDS, remission was defined as a total endpoint score of six or less (Fujisawa et al., 2010), and treatment response as a reduction of at least 50% in QIDS scores.
The index values of the EQ-5D-5L were calculated, and results of the pre-, post-, and one-month-after-program evaluations were compared. In addition, the EQ-5D-5L presented data as a health profile by providing a table with the frequency/proportion of reported problems for each dimension level at the prescribed intervals (pre- and posttreatment, one month after treatment). The GAF pre- and post-scores were compared using a t-test. All statistical tests were two-tailed, and an alpha value of <0.05 was considered statistically significant. All data analyses were conducted using JMP Pro 16. Cohen's d effect sizes calculated the difference between the means of the two groups (pre- and postintervention mean) divided by the pooled standard deviation of the two groups. Effect sizes are categorized as small (d = 0.20), medium (d = 0.50), and large (d = 0.80; Vandekar et al., 2020).
To determine the daily average of psychotropic drug usage (CP, IMI, and DZP-equivalent), the converted amount was calculated and compared before and after the treatment and analyzed using Wilcoxon signed-rank tests.
The sample size for this study was calculated based on previous studies that conducted the BATD. However, as this study is a preliminary, exploratory study examining the effects of a brief BA program, a power analysis will be conducted on the present data that may be useful for future studies.
Result
A total of 15 patients were recruited through psychiatrist referrals. Oral and written informed consent were obtained from them prior to the study.
Sample Characteristics
Twelve (80%) participants were women, and seven (46.7%) were married or lived with their partners (Table 2). Moreover, 14 patients were diagnosed with recurrent major depressive disorder and one with single episode major depressive disorder. The mean length of stay for patients was 80.3 (±50.1) days, and the mean length of hospital stay before the start of BA intervention was 36.1 (±29.5) days. There were no participants with cognitive impairments or physical disorders.
Sample Characteristics (N = 15).

Conversions of psychotropic drug use pre- and postintervention were compared. The median daily doses at pre- and postintervention were as follows. The CP-equivalent dose was 0 mg (Min: 0 mg-Max: 600 mg), the IMI-equivalent dose was 37.5 mg (Min: 0 mg-Max: 212.5 mg), and the DZP-equivalent dose was 0 mg (Min: 0 mg-Max: 12 mg). There was no significant difference in the usage of the drugs at the two time points.
Research Questions Results
Treatment and Dropout
Good intervention adherence was defined a priori (attending ≥ 3 of four therapy sessions). In total, 14 participants (93.3%) completed the program. One female patient with recurrent major depressive disorder dropped out during the third session owing to concentration difficulties. The mean attendance was 3.8 (SD = 0.4). The flow of participants at each stage is shown in Figure 1.

Flow of the participants.
Primary Outcome of the Program
No significant improvement in BDI-II scores was observed between the baseline, postintervention, and one-month postassessment (Table 3). However, the mean total score of BDI-II decreased from 25.60 to 22.73 to 22.06 across the three stages, respectively. Although the level of depression was clinically moderate and remained unchanged, the postintervention and follow-up scores (FU) were lower than the preintervention score. Three patients (20.0%) were evaluated to be therapeutically responsive, and three (20.0%) were considered to have achieved remission. The effect size was 0.30 (small to medium). The power (β-1) was 0.19.
Primary and Secondary Outcomes of the Program (N = 15).

Note: Time points: Pre (baseline), post (4 weeks), and FU (one-month follow-up). These are analyzed using repeated ANOVA and Tukey's HSD test, the GAF score analyzed using a t-test. *p < .05, significant difference in post comparisons with Pre.
BDI-II = Beck Depression Inventory second edition; QIDS = Quick Inventory of Depressive Symptomatology; GAF = Global Assessment of Functioning; EQ-5D-5L index values = EuroQOL 5 dimensions 5-level; EQ VAS = EuroQol 5-Dimension VAS.
Secondary Outcome of the Program
The mean QIDS-J score decreased from 18.80 to 15.86 to 15.53 across the three assessment points. Although the scores remained indicative of clinically moderate depression, postintervention and FU scores were lower than the preintervention score. According to this scale, four patients (26.7%) were judged to be therapeutically responsive, and two (13.3%) to have achieved remission. The effect size was 0.47 (medium range).
The GAF score, the only objective index in this study, improved significantly between pre- and postintervention (<.0001). The mean total GAF score increased from 40.20 to 57.00 across the pre- and postassessment points. According to a Code Description of Functioning of the GAF Score, this indicated that mental symptoms changed from serious (e.g., suicidal ideation, severe obsessional rituals, frequent shoplifting) to moderate symptoms (e.g., flat and circumstantial speech, occupational panic attacks). Furthermore, social occupational or social functioning changed from severe impairment (e.g., no friends, unable to keep a job) to moderate difficulty (e.g., few friends, conflicts with coworkers).
The calculated EQ-5D-5L index values and EQ VAS data are presented in Table 3. The EQ-5D-5L index values did not change postintervention, and no significant improvements in EQ VAS scores were observed between the three assessment points. However, the postintervention and FU EQ VAS score were higher than at preintervention. Thus, participants may have felt an improvement in their current health status postintervention and one month later.
When asked to rate their health status on the EQ-5D-5L's five items, the majority of respondents reported problems with everyday activities, pain and discomfort, and anxiety and depression. Across the three phases, the percentage of respondents who reported usual activity was 86.6%, 86.6%, and 73.3%, respectively, showing a decrease. Similarly, the percentage of respondents who reported problems with pain/discomfort was 80.0%, 80.0%, and 73.3% across the three phases, demonstrating a decrease.
Discussion
The results of this study showed that a short-term, four-week BA intervention by psychiatric nurses can be effective. However, the mean total of BDI-II and QIDS scores decreased over time, and no significant improvements were observed between the baseline, postintervention, and one-month postassessment. The health assessment results of the EQ-5D-5L's five items showed fewer respondents who reported problems in their usual activity and pain/discomfort. EQ VAS scores were also higher postintervention and at follow-up than the pre-scores, with no significant improvement. However, the GAF objective index scores improved significantly from pre- to postintervention (p < .0001). The program that were investigated had a low dropout rate (6.7%) and good treatment acceptability.
Depressive Symptoms
Although the intervention showed an improvement in depression rates, there were no significant differences in BDI-II scores or QIDS scores. The effect size was also not as large as in previous studies (Ciharova et al., 2021; Cuijpers et al., 2023., Stein et al., 2021). Inpatients are less likely to benefit from psychological treatment than outpatients due to the presence of comorbidities and other conditions and a high recurrence rate (Cuijpers et al., 2011). In fact, more than 90% of the subjects in this study were relapsed patients, which may have resulted in the lower effectiveness of psychological treatment compared to previous studies. However, considering that BA reduced symptoms of depression and that the effect size, although small, was demonstrated, this program could be helpful with improvements.
The average length of hospital stay for the subjects in this study was about three times longer than that in a previous study showing high efficacy with BA in hospitalized patients (Hopko et al., 2003). The prolonged length of hospitalization that characterizes Japanese psychiatric care can provide adequate treatment, but it has the disadvantage of a longer period of time away from contact with activities that promote positive reinforcement. Behavioral Activation promotes a decrease in depressive symptoms by increasing the patient's activity level. However, it is not only about increasing activity but it is also important to adhere to behavioral tasks to improve depressive symptoms. This is because completing assigned activities presumably increases response-conditioned positive reinforcement. Completing assigned activities, which means living life according to value-based activities, may lead to greater self-efficacy, a greater sense of accomplishment, and a reduction in depressive symptoms (Ryba et al., 2014). This suggests that BA improves depressive symptoms by increasing patients’ contact with diverse and stable sources of positive reinforcement and adherence to those behaviors. However, during hospitalization, the range of daily activities is limited, and time constraints exist; thus, the types of activities that can be provided are also limited. Merely participating in group-based ward activities is of relatively limited value in an individualized formulation and treatment plan (Curran et al., 2007). Supposing the hospitalization environment is relatively understimulating with only a few sources of positive reinforcement, patients may quickly descend into a ruminant thinking cycle, and their depressive symptoms could worsen. Therefore, when implementing BA for inpatients, even with many restrictions, greater benefits may be achieved by fully considering activities based on the person's values and helping them properly complete these activity tasks.
Quality of Life
The mean EQ-5D-5L index values and EQ VAS scores did not change significantly between the pre- and postintervention in this study. In a previous study of patients with chronic psychiatric disorders, the mean QOL score was reported to be 0.62 (van de Willige et al., 2005). The current study's mean EQ-5D-5L index value was 0.64 preintervention, 0.63 postintervention, and 0.64 one month after treatment. The mean EQ-5D-5L index values for pre- and postintervention were approximately the same for patients with chronic psychiatric disorders. EQ-5D-VAS was previously demonstrated to increase from 55.9 to 66.0 through an intervention of higher relational continuity of care that included informational continuity, management continuity, and relational continuity (de Cruppé et al., 2023; mean EQ-5D-VAS value of 51.53 at preintervention, 52.20 postintervention, and 55.13 one month after treatment). The interventions in the current study did not significantly increase EQ-VAS values compared to these previous studies. One such study (Burström et al., 2014) indicated that the mood dimension strongly influences EQ VAS scores when assessing one's current health status. It is possible that depression affected the results of the QOL because this study targeted patients with acute mental illness.
In this study, more individuals had problems with their usual activities, pain/discomfort, and anxiety/depression while they were hospitalized. A previous study comparing the five EQ-5D questionnaire items between inpatient and regional groups demonstrated similar results, with significantly more individuals in the inpatient group than the community group having problems with their usual activities and anxiety/depression (Takahashi et al., 2010). However, in the present study, FU scores showed improvement in usual activity and pain/discomfort items. Patients are forced to be inactive or restricted during hospitalization due to hospital treatment and examinations. Low activity associated with inpatient treatment of disease leads to the deterioration of functions necessary for activities of daily living (ADL) through various processes. Hospital-acquired disability, which causes a decline in physical function and ADL following hospitalization, has been shown to impair physical and cognitive function (Chen et al., 2022). In other words, it is presumed that the effect of BA appeared after discharge, although it was not possible to increase the amount of usual activity as an effect of BA in the hospital environment where movement was restricted. Previous studies also found significant mental health benefits of participating in physical activity (Pearce et al., 2022), although this was limited to the back pain and pain self-efficacy of people with nonspecific chronic pain. The effects of exercise are also known (Gilanyi et al., 2023). Therefore, it is possible that BA during hospitalization increased usual activity after discharge, resulting in less pain/discomfort.
Level of Functioning
The level of functioning was evaluated using the GAF score, the only objective index provided by a professional doctor. This measure can be used to understand how depression affects a patient's daily life and the degree of overall functioning. It is evaluated across two dimensions: the “severity” of mental symptoms and the “functional level” in society and occupation. In this study, the GAF score showed a significant improvement postintervention, although the subjective indicators of depression and QOL did not improve substantially. Results demonstrated that the subjective and objective indices were significantly different components. Depressed patients have a cognitive bias toward negative automatic thoughts (Chahar, 2020). Individuals with depression who undergo partial recovery display increased metacognitive monitoring, which is the ability to judge one's cognitive processes successfully; however, those with acute depression did not have this indication (Sheppard & Teasdale, 2004). The participants in the present study were inpatients in the acute phase of illness and in the middle of recovering from psychiatric symptoms. Therefore, they did not display sufficient metacognitive monitoring or the ability to judge their own cognitive processes accurately. Thus, there may have been a discrepancy between the subjective and objective indices. When providing BA intervention to people with acute mental distress, one must ensure that there are no significant discrepancies between subjective and objective indicators and that patients can monitor their metacognition. It is also necessary to cautiously monitor and evaluate patients’ mental states and place a balanced emphasis on the subjective and objective aspects of evaluation.
Dropout Rate
The completion rate for the BA program was 93.3%, with only one dropout. Previous studies reported inpatient completion rates of 71% (Bot et al., 2019) and 56% (range 48–100%; Pott et al., 2022) for BATD, indicating variation in the rate depending on the research. The completion rate in this study may result from trusting relationships between the therapist and participants, potentially established through communication. This study consisted of a four-session BA intervention, allowing participants to participate in the program until the end without feeling any burden of completion. The individual who dropped out had completed higher education and had milder depressive symptoms than the other participants (the baseline BDI-II score was 14 points). In contrast, a previous study showed that dropouts were associated with lower education and depression levels (Nakao et al., 2001). Therefore, carefully considering the factors behind this dropout is necessary to implement a BA program effectively.
Strengths and Limitations
The strength of this study is that it showed low attrition rates among participants and high levels of participation in the program, indicating a low burden on patients. The amount of medication used by patients differed widely, but overall there was no change in each individual's medication dosage during the intervention. Although it was possible that drugs did not primarily affect the results, the possibility that drugs and other treatments may be a confounding factor must be considered. In addition, the design of this study is relatively weak; the sample size was also small, with varying levels of depression severity and with many outcome indicators. Thus, a more extensive research study must unify the severity level of depression with medications and treatments to understand the impact of BA on depression comprehensively. A more long-term effectiveness study must be conducted to examine the effectiveness of the program not only during the period of hospitalization under observation but also under the management of the patient.
Implication for Practice
In this study, participants had low attrition rates and strong participation in the program, indicating a low burden on patients. It was suggested that a short-term BA program for hospitalized patients might improve depressive symptoms by encouraging behavior based on the value-based activities. Therefore, the BA program in this study was possibly useful in preventing relapse after discharge from the hospital. However, the program did not significantly improve depression or QOL. The preliminary and exploratory nature of this study and the very small sample size of 15 participants may have affected the power in the analysis. Power calculated ex post was 19%, and the sample size originally required was calculated (two-tailed, effect size = 0.3, α = .05, β = 0.20), resulting in a sample size of 90 participants. Consequently, it is necessary to consider the sample size from the present results when conducting this survey. Recommendations for further research focus on obtaining large amounts of data that may help determine the effectiveness of interventions. By including more sites over a longer period, it may be possible to more accurately determine whether the observed results are due to the intervention or other factors.
Conclusion
In this study, a BA program completed in four sessions for hospitalized patients was piloted. The results showed that the program did not significantly improve depressive symptoms or QOL. However, considering that BA reduced symptoms of depression and that the effect size—although small—was demonstrated, this program could be helpful with improvements. During hospitalization, the scope of daily activities is limited, and time constraints limit the types of activities that can be offered. Therefore, in improving this BA program, when implementing BA for inpatients, it is important to fully consider activities based on the patient's values and to assist the patient in performing the activity tasks appropriately. It is necessary to establish a short-term BA program that can be completed during the hospitalization period in order to prevent the recurrence of depressive symptoms due to sudden environmental changes after discharge from the hospital.
Footnotes
Acknowledgments
The authors are grateful to Mr. Yuuma Aiboshi and Ms. Haruka Ikeda (University of Miyazaki Hospital) for assisted in data collection; Editage (![]() ) and Mr. Joel Hensley (Miyazaki Prefectual Nursing University) for English language editing. This study is a part of the study conducted with grant JSPS KAKENHI (Grant Number: 16H07085 to SK).
) and Mr. Joel Hensley (Miyazaki Prefectual Nursing University) for English language editing. This study is a part of the study conducted with grant JSPS KAKENHI (Grant Number: 16H07085 to SK).
Authors’ Contribution
SK, HT, and YI conceptualizated the study. SK and JF took a role in the investigation, and SK and HT methodology. SK witting - original draft, All authors witting - review and editing, critically revised the first manuscript for important.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
This study was approved by the Miyazaki University of Health Sciences study protocol approved this study (approval number: I-0014-2) on January 10, 2017. It was registered with the University Hospital Medical Information Network Clinical Trials Registry (ID: UMIN000026539).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:This work was financially supported by JSPS KAKENHI (Grant Number: 16H07085 to SK).