
Abstract
We aimed to measure the self-assessed level of competence among nurses working in the public hospitals of Al-Gharbia Region, a remote rural region of United Arab Emirates, and to explore the factors associated with the nurses’ self-perceived competency. The Nurse Competency Scale, which measures the self-assessed level of competency of nurses, has been validated in a variety of clinical settings, in facilities of various sizes, and in small and large cohorts. However, its application among an expatriate nursing workforce working in small hospitals and health facilities in remote and rural areas has not been examined. We used the Nurse Competency Scale to survey the nursing workforce in Al-Gharbia’s public hospitals in United Arab Emirates. All 435 practicing registered nurses with more than 3 months clinical experience in the network were invited to participate. Data were collected electronically and analyzed by international collaborators. Statistical analysis included analysis of variance, Kruskal–Wallis, multiple linear regression, χ2 test of independence, and Cronbach’s α. Totally, 189 responses were analyzed (43.4% response rate). Overall self-assessed levels of competence were uniformly “very good” across all competence categories. The overall score (84.3) was higher than those found in most other studies. Frequency of use was the most outstanding variable influencing self-assessed competence. Total years of experience were the next significant variable. Some items of the scale were not yet applicable to activities in the region, particularly those relating to supervision of students. The high scores achieved by expatriate nurses in the small hospitals of Al-Gharbia reflect well on the rigor of the recruitment process, ongoing cross-training and functional competency assessment. Policies and practices aimed at recruiting experienced expatriate nurses and providing opportunities to use competencies continue to be critical in providing a quality nursing service in a rural and remote region.
Keywords
The United Arab Emirates (UAE) has a high-quality health-care system, characterized by well-equipped, well-staffed, licensed hospitals; qualified and licensed health-care providers; and universal medical insurance coverage. The competency of nurses is taken seriously, with high stakes (including legal and immigration consequences) for malpractice. This study investigated self-assessed competence among an expatriate nursing workforce in Al-Gharbia, the geographically largest and least populated region in the Emirate of Abu Dhabi. In part, it represents an effort to find a relevant, useful, and practical assessment tool that may assist in maintaining high standards of nursing competency in Al-Gharbia. This study reports a survey conducted in 2015 in the region’s public hospitals network, which used the Nurse Competence Scale (NCS), a popular, validated survey instrument (Meretoja, Isoaho, & Leino-Kilpi, 2004).
This study has relevance for the emerging field of self-assessed competence as a marker for professional nursing competence more generally. It is relevant to modern, well-resourced regional hospitals with in-service training and preceptor programs, rural and remote health-care systems where nurses provide services across multiple clinical areas, often with limited frequency, and the management of expatriate nurses.
Background
Al-Gharbia
The Al-Gharbia region, Abu Dhabi, sits at the border between the UAE and Saudi Arabia and is largely sand desert. It is part of the Arabian Peninsula’s “empty quarter” (Figure 1). In 2014, Al-Gharbia had 8.9 persons per square kilometer and a total population of 313,000 people, of which 9.4% were UAE citizens. The remaining 90.6% were noncitizens, mainly employed in oil and gas production, regional development, and accompanying services. Of noncitizens, 84.4% were male and predominantly working age, with few aged over 60 years (Statistics Centre Abu Dhabi, 2015).
Al-Gharbia region, Abu Dhabi Emirate, UAE.
Al-Gharbia is medically well serviced. The region has seven rural townships with modern, licensed hospitals that are well-equipped and resourced. The public hospitals network provides primary, secondary, and selective tertiary care. It comprises six hospitals with an aggregate 358 bed capacity, three primary care clinics, and a family medicine center. The range and level of services has improved in recent years and more patients seek treatment locally. The highest risk patients are transferred to the city of Abu Dhabi.
The region has experienced rapid population expansion, and the public hospitals network has a proactive approach to resourcing. At the time of this survey, there were 585 budgeted nursing positions; 435 were filled and the remainder in process. Staffing is sufficient in the context of current occupancy rates and support staffing levels are good. Most patients are young, healthy, working-age expatriate men living away from family. This population does not have the same demands as a more gender- and age-distributed population. There are fewer female patients who are nursed on separate floors. Cultural values do not permit male nurses to work in female wards.
UAE National Licensure for Nurses
Sound professional competence is of vital interest to the UAE, and professional licensure is the gatekeeper. All practicing health professionals are licensed, registered, and hold medical indemnity cover. UAE entry standards for expatriate nursing staff include a minimum nursing education of 3 years and at least 2 years of experience. Nurses must pass a written examination in English before licensing, which is necessary to obtain a work permit. Nursing registration and licensure are under the jurisdiction of the Health Authority of Abu Dhabi, Dubai Health Authority, and the UAE Ministry of Health (Brownie, Hunter, Aqtash, & Day, 2015; UAE Ministry of Health, Health Authority Abu Dhabi, & Dubai Health Authority, 2014).
Nursing Competency in Al-Gharbia
Competency requirements for nurses are determined by the Nation, the Emirate, and the employer, with input from the nursing profession (UAE Ministry of Health et al., 2014). The UAE National Qualifications Framework (competency model) has established requirements for assessing the competence of student nurses graduating in the UAE (UAE National Qualifications Authority, 2012); however, Al-Gharbia had only one Emirati nursing graduate at the time of this study. The public hospitals network nursing management (all registered nurses [RNs] with BScN and MScN degrees) has a well-established competency validation program based on nurse self-assessment of mandatory competencies and in-depth discussion with nurse managers as needed. This validation is separate from annual staff performance reviews (a human resources function). Competency validation is performed on an individual basis. The competency matrix defines the nature and scope of mandatory, general and unit-specific competencies and dictates the frequency of revalidation of a nurse’s competency. Mandatory competencies are validated by a preceptor or senior nurse during orientation and repeated yearly. General competencies are validated during probation and may be validated again during the course of employment. Unit-specific competencies are assessed in real nursing situations during probation and revalidated every second year. Competency assessment also includes examination at licensing, post in-service education, and competency validation by a preceptor in real-life situations. This competency validation program is designed to meet the region’s need for generalist nurses with specialist capability.
There are significant challenges in maintaining optimal nursing competency. Although Al-Gharbia has low population and high cultural diversity, rapid population growth means the public hospitals network undergoes constant expansion. The network depends on recruitment and retention of skilled, experienced expatriate nurses. In larger hospitals, nurses provide care based on their area of specialty, whereas the scope of practice is extended in smaller hospitals, and nurses are multicredentialed. Some clinical environments have low patient volumes and some medical events occur with low frequency (e.g., pregnancy and postpartum care). In response to low patient volumes (e.g., few postpartum care and high-risk specialist services), nurses are required to have competencies validated in more than one specialty. Around three quarters of nurses are crosstrained, and most have medical/surgical experience. In this remote, rural health system, nurses must undertake a range of duties and exercise sound autonomous judgement. Distance and desert conditions require that health facilities provide combined services, and nurses in this region must be flexible, responsive, and multiskilled.
Literature Review
The definition, measurement, and validation of nursing competence remain controversial (Garside & Nhemachena, 2013). Different methodologies have been used to define the concept of competency and describe the factors that constitute it. Researchers have employed expert interviews, questionnaires, focus groups, and expert panels to survey and gain consensus, often using a Delphi process (E. Hurme, 2009; F. Hurme, 2007; Meretoja, Isoaho et al., 2004). Some nations have also drafted policy, guidelines, and standards and instituted regulatory and credentialing processes to ensure competency (Brownie et al., 2015).
Measurement of a nebulous construct is difficult, and there is no consensus regarding the best way to measure competence. Providing hard evidence of competency is challenging for all layers of the nursing workforce and is costly in time, effort, and funding. Managers and researchers are often left to design their own tools and use multiple methods to confirm the results of their competency assessment. In seven focus groups with RNs and midwives across three hospitals in Australia, Fereday and Muir-Cochrane (2006) showed that the performance review process provided nurse clinicians opportunity to self-assess their ability and comfortability in performing their work and the chance to benchmark their own assessment against continual feedback collected from their peers and unfamiliar challenges. This self-declaration of competence has become a requirement for continuing nursing registration in parts of Australia, as part of a multimethod approach of defining competence by a set of outcome standards (Fereday & Muir-Cochrane, 2006; McCready, 2007; Nurses Board of South Australia, 2000).
As there is no set way of interpretation, the validation process may take many forms, including direct and indirect observation. Simulation drills are also used (Inman, 2016). Supervisors or preceptors (Butler et al., 2011) are deployed to observe skills and attitudes, question the knowledge base, coach, mentor, and ensure compliance. Checklists are used to aid these processes.
In the nursing profession, the frequency of use (FOU) of a competency and years of experience are positively correlated with self-assessed competency (Hengstberger-Sims et al., 2008; Meretoja, Isoaho, et al., 2004; O’Leary, 2012; Salonen, Kaunonen, Meretoja, & Tarkka, 2007). Additionally, self-assessment of competence is gaining traction as an important indicator of competence. The NCS (Meretoja, Isoaho, et al., 2004) is a prominent scale among various validated competence self-assessment tools, including the Six Dimensional Scale of Nursing Performance (Schwirian, 1978), European Healthcare Training and Accreditation Network (ETHAN) Questionnaire (Cowan, Wilson-Barnett, Norman, & Murrells, 2008), and the Competency Inventory for RNs (Liu, Yin, Ma, Lo, & Zeng, 2009). The NCS was developed, tested, and validated in a Finnish University Hospital (Meretoja, Isoaho, et al., 2004). The intended use was nurses and managers assessing nurse competence using self-assessment. The NCS has good internal consistency and good content validity; however, “concurrent and predictive validity testing with large samples was needed in the future” (Meretoja, Isoaho, et al., 2004, p. 131).
The NCS has been used in numerous studies by the Meretoja group in both large and small cohorts (Meretoja & Koponen, 2012; Numminen, Leino-Kilpi, Isoaho, & Meretoja, 2015). Underlying indicators of competent nursing practice have been validated (Meretoja, Eriksson, & Leino-Kilpi, 2002). The NCS has been tested in intensive care, high dependency, and emergency units (Salonen et al., 2007); different hospital environments (Meretoja, Leino-Kilpi, & Kaira, 2004); and with graduating student nurses (Kajander-Unkuri et al., 2014; Wangensteen, Johansson, Björkström, & Nordström, 2012). It has been translated from Finnish into English (Meretoja, Numminen, Isoaho, & Leino-Kilpi, 2015), Italian (Dellai, Mortari, & Meretoja, 2009), German (Müller, 2013), Norwegian (Wangensteen et al., 2012; Wangensteen, Johansson, & Nordström, 2015), and Lithuanian (Istomina et al., 2011) and tested in Australia (Hengstberger-Sims et al., 2008), Iran (Bahreini, Shahamat, Hayatdavoudi, & Mirzaei, 2011), Ireland (McCarthy, Cornally, O’Mahoney, White, & Weathers, 2013), and Switzerland (Müller, 2013). Supplementary questions have been added (McCarthy et al., 2013), and it has inspired the development of new tools (Donilon, 2013).
The construct validity of the NCS has received criticism, with previous studies finding redundancy and that they could not confirm the seven category (across 73 competency items) model (Müller, 2013; Wangensteen et al., 2015). In a reanalysis of 2007 dissertation data, Wangensteen (2010) could not confirm the original NCS seven category model. Müller used confirmatory factor analysis and Rasch modeling with data generated in a 2007 study, and found a “reduced set” of six categories and 54 items that “removes redundancy among items, is free from item bias and constitutes six uni-dimensional scales” (Müller, 2013, p. 1410). Missing values are also a recurring feature with the NCS (Numminen et al., 2015; Wangensteen, 2010; Wangensteen et al., 2015), and the reasons for this phenomenon have not been addressed. Treatment for missing values has been rejection of responses with values under 50% or substitution with the mean.
The NCS has mainly been tested in large teaching hospitals in metropolitan settings, where nurses operate within distinct clinical environments and have predictable nursing responsibilities. Increased perceived competency has been associated with increased FOU of a competency item (Meretoja, Isoaho, et al., 2004; Meretoja & Leino-Kilpi, 2003; Numminen, Meretoja, Isoaho, & Leino-Kilpi, 2013). Nurses usually perceive their competency as “good” (Meretoja, Isoaho et al., 2004), and managers generally perceive their nurses to have higher competency than do nurses themselves (Numminen et al., 2015).
There is limited research into rural/remote nursing competencies, including measurement or assessment. The available literature suggests rural nurses are often required to be skilled and knowledgeable generalists, capable of providing patient-centric nursing regardless of clinical specialty (Hunsberger, Baumann, Blythe, & Crea, 2009; Montour, Baumann, Blythe, & Hunsberger, 2009). Lovelace (2015) also noted that rural nurses have a greater scope of practice than their urban counterparts and are generalists who “must have at least some specialty knowledge in multiple areas of nursing.” Rural nurses must also know when to assess their patients, stabilize them, and transfer them safely to an advanced level of care for more specialized treatment (Lovelace, 2015, p 1). In remote areas, this can involve longer distances, limited ambulances, or other transport and poor roads. Lovelace suggested that “independence, flexibility and a strong sense of adventure” (p. 1) are necessary characteristics for rural nurses (Lovelace, 2015). Resourcefulness and innovativeness are important, as nurses must deal with absence of economies of scale and sometimes poor access to resources (including Internet and library access). Rural nurses usually live and work in the same small communities, meaning they are visible and lack anonymity. In rural communities, a nurse’s competence can even be judged on their children’s behavior (Bushy, 2002). Personal characteristics, behaviors, and attitudes become more important in this context and understanding the community and cultural competencies are critical in rural and remote environments (Morgan & Reel, 2003).
In her doctoral dissertation, Hurme (2007) used a Delphi panel of rural nursing experts to identify rural nursing competencies most associated with critical access hospitals. She highlighted similarities and differences between urban and rural nursing competencies and identified competencies specific to the rural environment in a Louisiana population. These included the importance of possessing knowledge of and ability to assess patients across the life span and being certified in both pediatric advanced life support and advanced cardiac life support. However, there are no examples of the NCS having been tested in rural and remote settings.
Study Purpose
The primary purpose of the present study was to measure the self-assessed level of competence (SALC) among nurses working in the Al-Gharbia public hospitals network and explore factors associated with nurses’ self-perceived competency. The secondary purpose was to use a popular, validated tool that permitted the results to be compared with those from other countries to help identify areas for future professional development.
Research Questions
The research questions for this study were (a) What is the overall level of self-assessed competence? (b) How do nurses rate themselves in specifically defined areas of competence? (c) What differences in self-assessed competency occur between clinical areas and facilities? (d) What variables are associated with nurses’ perception of their competence?
Method
Design
A cross-sectional study design was used to allow the public hospitals network to determine the current level and nature of competence of the region’s nursing workforce. A literature review identified several scales that could have been used for the survey (Cowan et al., 2008; Gardner, Smyth, Renison, Cann, & Vicary, 2012; Lakanmaa et al., 2014; Liu et al., 2009). Permission to use the Clinical Competence Questionnaire was initially obtained (Liou & Cheng, 2014). However, the present research team selected the English version of the NCS for two main reasons. First, the NCS has been used in many studies worldwide, including several European countries and Iran in the Middle East, and in a number of languages. In those studies, the NCS appeared to be stable and had good Cronbach’s α values compared with other scales. Secondly, the NCS was the best fit for this study, as it focuses on (a) self-perceived competency and (b) FOU of the competencies. These two areas were the focus of competency concern for the nursing leadership in Al-Gharbia. As previously mentioned, nurses in smaller facilities (critical access facilities) often do not use some of their competencies for periods of time. This may negatively affect nurses’ perception of being competent as well as their ability to actually perform certain skills safely. The NCS was regarded as the best tool to capture these two areas.
Use of the NCS allows comparison of the present results with those from other countries, benchmarking Al-Gharbia’s expatriate nursing workforce competency in an international context. The NCS has not previously been validated in a small hospital context, in rural or remote conditions, in an expatriate or multicredentialed workforce, and in the Arab world or across an entire nursing workforce. Although this context makes Al-Gharbia unique, individual factors are experienced internationally. The development of the NCS was guided by Benner’s stages of clinical competence framework. This suggests that to acquire and develop clinical skills and competence, nurses should pass through five levels of proficiency: novice, advanced beginner, competent, proficient, and expert (Benner, 1984).
Sample
This study used a purposive sample of 435 RNs, which was the public hospitals network entire nursing workforce. This permitted maximum population validity within the network’s nursing workforce. Inclusion criteria were RNs who had worked in the network for a minimum of 3 months and who provided direct nursing care. Newly hired nurses (those who had worked in the network for less than 3 months), practical nurses (UAE Ministry of Health et al., 2014), and those working entirely in administrative positions were excluded. This is consistent with approved NCS methodology.
Ethical Considerations
This study was approved by the Institutional Research Ethics Committee of the public hospitals network. Copyright permission to implement the NCS was obtained from the publishers, and NCS methodology was followed as required (Meretoja, Isoaho et al., 2004). Informed consent was obtained from all participating nurses. At the beginning of the questionnaire, respondents placed a checkmark next to a statement indicating their agreement to join the study and complete the survey. Participation was voluntary and no incentives were offered. Respondents were guaranteed anonymity. The survey was administered online via Google Forms and did not include identifying material.
Survey Instrument
Permission to use the NCS was contingent on using the complete scale. No modifications to the scale (Meretoja, Isoaho et al., 2004) were made. The NCS measures self-perceived competency in 73 nursing items grouped into seven competency categories (areas of competence). The NCS uses a Visual Analogue Scale (VAS) with a range from 0 to 100. Respondents rate their level of competence by placing a mark on a line with 0 at one end and 100 at the other. The VAS is suited to a paper environment and is not able to be used in Google Forms. Instead, respondents were asked to rate their competency out of 100. A 4-point Likert-type scale is used to measure the FOU of each NCS competency item.
Competence measure
NCS competency items are grouped into seven categories: helping role (seven items), teaching–coaching (16 items), diagnostic functions (seven items), managing situations (eight items), therapeutic interventions (10 items), ensuring quality (six items), and work role (19 items; Meretoja, Isoaho et al., 2004). For each item, respondents were asked to place a number from 0 to 100 in the designated box, with 0 being very low and 100 very high. This measure reflects the SALC. “Item SALC” represents the SALC for each item. “Category SALC” means the average of Item SALCs within that category, and “Overall SALC” refers to the average of the seven Category SALCs. These SALC measures can be calculated for a respondent, for sub-groups of respondents or for all respondents. The term “SALC” is used throughout this article to introduce rigor to terminology and avoid confusion with actual competence. For analysis, the NCS methodology breaks the SALC measure into four overlapping integer groups: 0 to 25 is low, 25 to 50 quite good, 50 to 75 good, and 75 to 100 very good. In the present sample, this was modified slightly for clarity, with 0 to 24, 25 to 49, 50 to 74, and 75 to 100 as the integer ranges for the groups.
Frequency of use
A 4-point Likert-type scale (0 = not applicable in my work, 1 = used very seldom, 2 = used occasionally, 3 = used very often in my work) was used to capture the FOU of each item (Meretoja, Isoaho et al., 2004). Respondents were asked to indicate “the frequency with which this item is actually used in clinical practice.”
Data Collection
An explanatory e-mail was sent to all RNs in the public hospitals network inviting participation in the survey. The NCS was coded in Google Forms and made available for completion online between May 26 and July 16, 2015. Nurses were then e-mailed a link to the website where the survey could be completed. Two reminder e-mails were sent.
Statistical Analysis
Statistical analyses were performed with the R package (R x64 3.2.2). Microsoft Excel was used for summary statistics and graphics.
Categorical variables
Demographic variables included gender, age-group, highest level of education, marital status, ethnicity/nationality, total years of experience, years of experience in the public hospitals network, current position, facility, and clinical area. These were collected as categorical variables. Intervals between points on the FOU scale are not equal and therefore cannot be interpreted as numerical values. These data were captured, stored as text, and analyzed as categorical variables.
Missing values
Respondents with 50% or more missing values were excluded, consistent with NCS methodology. If a respondent was missing SALC for every item in a category, their Category SALC was recorded as “not available.” Otherwise, their Category SALC was the average of the available Item SALC. Overall SALC was calculated as the average of the available Category SALC. If a variable was used in an analysis and a respondent had a missing value for that variable, that respondent was excluded from the analysis. For the multiple linear models for each item, only respondents with Item SALC, Item FOU, and all demographics were included.
Merged responses
As some response categories had small counts, similar demographic groups were merged for analysis. For “age-group,” nurses aged ≤ 25 years and 26–35 years were merged. For “marital status,” separated and divorced nurses were merged. For “clinical area,” merging occurred between critical care and operating room, medical/surgical and managerial positions (managerial positions were nurses who worked in senior charge nurse capacity and had a medical/surgical background), outpatients and emergency, and pediatrics and obstetrics. The four nonhospital facilities were merged. Decisions regarding merging clinical area response categories were made by the lead researcher, a nurse, and proper consideration of Al-Gharbia conditions.
Aggregated data
When an analysis found small numbers of responses in cells, data were aggregated to increase the strength of statistical analysis, where the test required the expected values of each cell to be ≥ 5. This occurred in the pediatrics/obstetrics clinical area and in the first-two FOU levels.
Statistical tests
Statistical tests used to assess the significance of relationships included: analysis of variance (ANOVA) to test the association of individual demographics with SALC; the Kruskal–Wallis test, a nonparametric test for differences in median where the numbers of responses were small and not normally distributed; the χ2 test of independence where two or more categorical variables were included; Cronbach’s α to test internal consistency; and Tukey’s multiple comparisons of means for post hoc analysis of differences.
Because FOU only occurs at the item level, testing the association of FOU with SALC required a multiple linear model for each of the 73 items, with FOU and demographic variables as independent variables and item SALC as the dependent variable. The significance of models was tested with regression ANOVA, and an independent variable was deemed to be significant if at least 1 of its levels was p < .01.
Results
In total, 227 responses were received from all network facilities and clinical areas (response rate 52.2%). After excluding responses with 50% or more missing values, 189 responses were analyzed, representing 43.4% of the nurse workforce.
Respondent Characteristics
Respondent Characteristics.

Percentages may not add to 100% due to rounding.
Overall SALC
The overall SALC for the study sample was very good at 84.3.
SALC in Defined Areas
Categories
All RNs rated themselves as very good (the highest competence level) in every category. They assessed themselves as most competent in management situations and least competent in ensuring quality and teaching–coaching situations (Figure 2). At the item level, mean SALC scores were mostly in the very good range and occasionally were in the good range (Table 2).
Self-assessed level of competence by category. SALC, FOU, and Significant Variables Associated With SALC. Note. SALC = self-assessed level of competence; FOU = frequency of use; n/a = not applicable; SD = standard deviation; F = FOU; A = age: Ed = education; Et = ethnicity; Yr = total years of experience; Yr N = years in the network; Fa = facility. Percentage of respondents who rated themselves < 50 on the Visual Analogue Scale. At least one level of the variable was significant at p < .01.

Reliability analysis within categories
Reliability of Categories in the Scale.

Low SALC items
Items where individual RNs recorded SALC less than 50 (excluding nonresponses), were “coordinating student nurse mentoring in the unit” (19.6%), “supporting student nurses in attaining goals” (15.5%), and “taking student nurse’s level of skill acquisition into account in mentoring” (14.1%). These items also had the greatest nonresponse.
Differences in Competency Ratings in Nurses Working in Different Clinical Areas and Facilities
The four clinical areas did not show significant differences in overall SALC (ANOVA; p = .177). Although SALC means for all network facilities were in the broad classification of very good (=75+), there were significant differences (ANOVA; p = .0001), as shown in Figure 3. Post hoc analysis of these differences using Tukey’s multiple comparisons of means with a 95% family-wise confidence level showed there were no significant differences between pairs of hospitals, but that RNs from primary care clinics had significantly lower scores than four of the six hospitals. Nonhospital-based facilities had the lowest overall SALC (75.7), with ensuring quality (71.6), “work role” (72.5), and “therapeutic interventions” (73.0) having the lowest category SALCs.
Boxplot of overall self-assessed level of competence score by facility.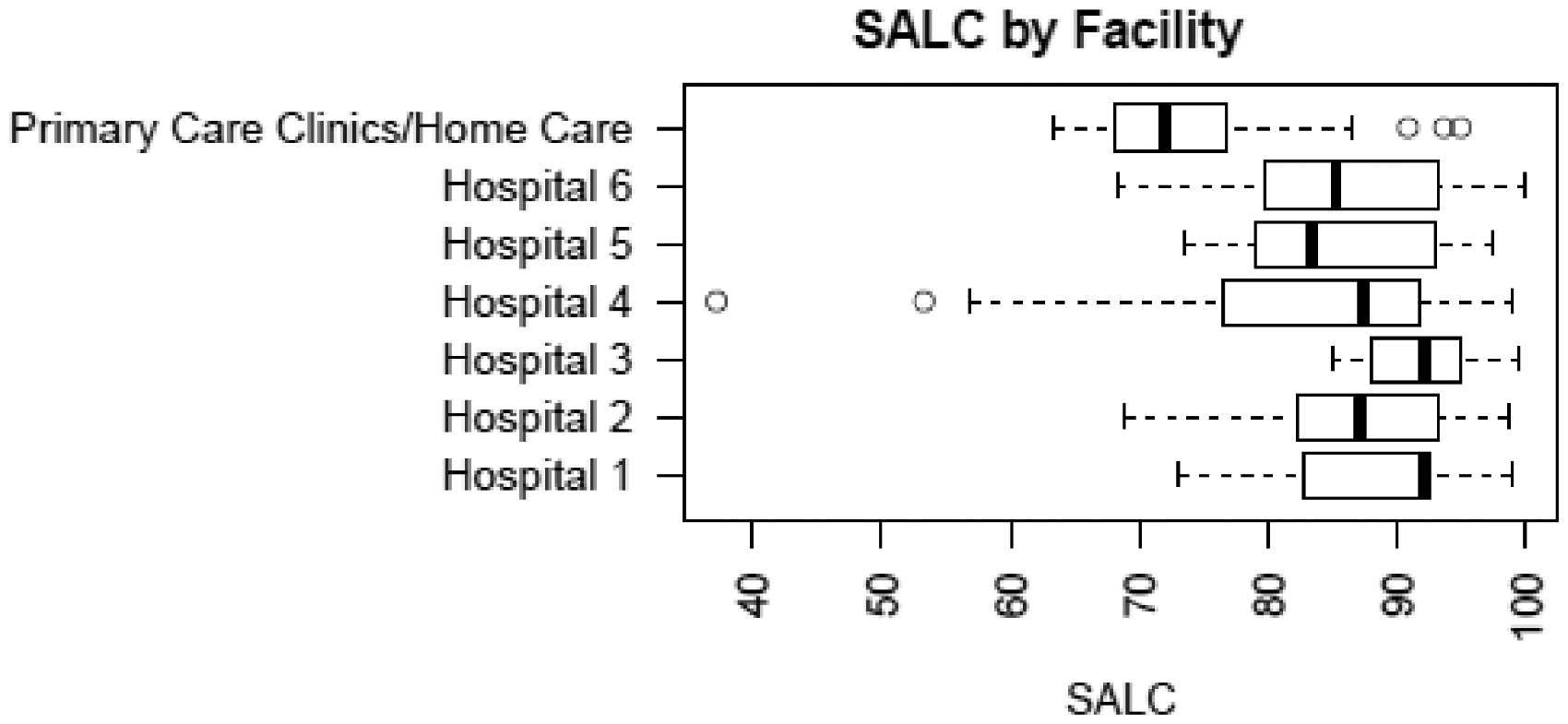
Item FOU
For the majority of RNs, “not applicable” items were related to student nurses. These items were “coordinating student nurse mentoring in the unit” (50.0%), “supporting student nurses in attaining goals” (49.7%), and “Taking student nurse’s level of skill acquisition into account in mentoring” (44.4%). The next item most frequently identified as not applicable was “mentoring novices and advanced beginners’ (15.8%). Both “orientation for new nurses” and “guiding staff members” were not applicable for over 6.5% of RNs. All other items were not applicable for fewer than 6.5% of RNs (Table 2).
Items with the highest FOU were “documentation of patient care” (87.0%), “equipment maintenance” (86.4%), “individualized patient education” (84.5%), “planning patient care” (82.3%), “ability to recognize life threatening situations” (79.4%), “modifying care plans to suit needs” (78.1%), and “finding optimal timing for patient education” (78.1%).
Differences in FOU by Clinical Area
Fourteen items had significantly different FOU across clinical areas (χ2; p < .01). Nurses in outpatient, emergency, critical care, and operating room environments reported the highest FOU for most competency items. Pediatrics/obstetrics had the highest FOU for “coaching others in duties within my responsibility area” and “professional identity serves as resource in nursing.” Medical/surgical RNs reported the lowest FOU for all significant items, except “coordinating multidisciplinary team’s nursing activities,” where pediatric/obstetric nurses had a lower FOU.
Variables That Influenced Nurses’ Perception of Their Competence
To determine the association between FOU and SALC in the context of demographic variables, regression models were produced for each item. All models were significant (ANOVA, highest p value was .0058). FOU was a significant variable for 62 of the 73 items. For 34 of these items, it was the only significant variable. Total years of experience was significant for 20 items, facility for seven items, ethnicity for six items, education for five items, years in the network for two items, and age-group for one item (Table 2). Gender, marital status, current position, and clinical category were not significant in any model. No variables were significant for seven items (Table 2).
For four items, FOU was not significant, but other variables were: “years of experience” was significant for “evaluating critically own philosophy in nursing”; years of experience and “years in the network” were significant for “developing documentation of patient care,” with over 15 years in the network having a negative association; years of experience was significant for “incorporating relevant knowledge to provide optimal care”; and facility was significant for “able to recognize colleagues’ need for support and help,” with hospital RNs scoring higher than those in clinics.
Discussion
Overall SALC
The Overall SALC in Al-Gharbia was 84.3 or very good (Table 2). This was high compared with almost all other studies of a reasonable sample size that used the NCS. It was most similar to an Iranian study, in which RNs with BScN qualification working in a range of areas achieved 87.03 in “Type 1 University Hospital” and 71.07 in “Type 2 University Hospital” (terms not defined; Bahreini et al., 2011).
In Finland University Hospital(s), results were 56.1 for RNs with limited work experience (Salonen et al., 2007), 63.7 for RNs in medical/surgical environments (Meretoja, Isoaho et al., 2004; Meretoja, Leino-Kilpi, et al., 2004), 63.9 for 81 staff nurses working in a variety of environments (Meretoja & Leino-Kilpi, 2003), and 66.0 for RNs with broad range of experience in four clinical environments (medical, surgical, pediatric/obstetric, and psychiatric; Meretoja et al., 2015). Previous studies showed Overall SALC was 59.0 for those aged 20–29 years, 65.0 for those aged 30–39 years, 70.1 for those aged 40 years and over (Meretoja et al., 2015), and 66.7 for graduating student nurses in their final clinical placement (Kajander-Unkuri et al., 2014).
Understanding self-assessed competency in nurses in Al-Gharbia
The high overall SALC in this study population may be understood in the context of the nursing workforce in Al-Gharbia. All expatriate nurses undergo rigorous testing as part of the due diligence for their appointment. It is Abu Dhabi’s practice to screen all nurses for qualifications, experience, character, and fluency in English before licensing, registration, immigration, and appointment. These are experienced nurses and Meretoja et al. (2015) found self-assessed competence increased with age, with those aged 40 years and over having higher ratings than those aged 20–29 years by a difference of 11.1 percentage points. Their rating for younger staff (59.0 for 20- to 29-year olds) was consistent with that of RNs with limited work experience (56.1) found by Salonen et al. (2007).
In Abu Dhabi, nurses are interviewed before employment and deployment. There are strong motivators for nurses to maintain and develop competencies. Residence in the UAE is dependent upon employment, and work permits are renewed at the end of a 3-year period. Expatriates may not become citizens and must leave the UAE after employment ceases. Most expatriates send remittances home to support families, meaning their sense of dedication to work is heightened by a desire to remain in the UAE and earn money to send home. The Al-Gharbia nursing workforce is stable, with most nurses staying more than 5 years.
A culture of competence and professionalism exists among nurses in Al-Gharbia, who access continuing practice development opportunities as offered. Nursing management provides extensive orientation, training, and testing to ensure continued competence. Management also screens nurses entering the region with clinical scenarios and has an established program of continuing education and performance appraisals. Nurses in Al-Gharbia are accustomed to assessment post in-service training.
In Al-Gharbia, as with many rural or remote settings, nurses can see that their presence makes a difference to health care. Nurses invariably have ready access to supplies and the latest equipment necessary to do their job. Hospitals and clinics are modern, clean, and well supported by cleaning and administration staff. With a younger, generally healthy population, nurses may also have less exposure to conditions that can create “burn out.”
Self-Assessed Competence in Defined Areas
In this study, there were no significant differences by clinical area, meaning the overall SALC (84.3) can be compared with that in studies involving a range of clinical areas (63.7; Meretoja et al., 2015) and medical/surgical areas (66.0; Meretoja, Isoaho et al., 2004). If permission to use the scale had allowed flexibility for modification, redundant items could have been removed. Student-related competencies are not required in Al-Gharbia, where all expatriate nurses are educated and experienced. Therefore, it is unsurprising that participating nurses were least confident in items relating to students (SALC: 65.7–70.4; Table 2). The poorest Item SALC was for coordinating student nurse mentoring in the unit, with 50% of RNs indicating it was not applicable. However, it is interesting that around a quarter of responses indicated the FOU for student-related items was “very often.” These items might have been misinterpreted to mean new staff. RNs with more regional experience were involved in orienting and coaching new staff on probation and other staff in tasks such as the “use of diagnostic equipment” and “mastering rapidly changing situations,” where SALC was reported as very good.
In addition, items relating to family were expected to have low FOU (except in female wards). However, around half of the RNs indicated FOU was very often for these items. Nurses also rated their overall SALC in these items as very good which might relate to prior experience. These results indicate there may be issues with the practical application of the NCS and may also point to reliability and validity issues. These concerns are discussed in the limitations section and will be elaborated in a future article. RNs in this study sample indicated comparative weakness (still very good) in “utilizing research findings in relationships with patients” (77.0), “Utilizing research findings in nursing interventions” (78.5), “utilizing research findings in further development of patient care” (79.9), and “making proposals concerning further research and development” (72.9). These were also lower frequency items, with 31–39% of respondents rating FOU as very often.
Limitations
Data collection
The decision to collect age, overall years of experience, and years of experience in a categorical format reduced the ability to be definitive about the strength of the association of these variables with SALC.
Face validity
The NCS has been tested for face validity as a measure of self-assessed competence and stands as a subjective measure. This study did not assume that it represented other measures of competence, such as objective tests or supervisor assessment.
Construct validity
The construct validity of the NCS has received criticism for redundancy and nonconfirmation of the seven category model (Müller, 2013; Wangensteen et al., 2015). In this study, the high Cronbach’s α for the categories also suggested a level of inbuilt redundancy. In addition, several NCS items were not relevant for the present study population, specifically those related to students and research. Items about student supervision and management are found in the NCS “teaching–coaching” and “work role” categories. Items relating to research are in the “helping role,” “therapeutic interventions,” and “ensuring quality” categories.
Bias
There remains a possibility of a compliance bias if participating nurses were trying to please nursing management; however, response rates were similar to other studies that used the NCS. If Al-Gharbia nurses felt under duress to respond, a much higher response rate and lower missing values would be expected.
Missing values
As for other NCS studies, missing values were a feature of survey returns (Kajander-Unkuri et al., 2014; Meretoja, Isoaho et al., 2004; Meretoja & Leino-Kilpi, 2003; Meretoja, Leino-Kilpi, et al., 2004; Numminen et al., 2013; Salonen et al., 2007). This adds complexity to the analyses and reduced instrument practicality and user friendliness.
Practicality of the NCS
There is no clear published methodology for online implementation of the NCS (Meretoja, Isoaho et al., 2004) and no definition, scope, or examples given for any item to aid nurses in understanding item statements. The lack of clear instructional methodology required to implement the NCS as a management tool suggests that the prime audience for NCS is researchers of nursing competency rather than nursing managers or nurses themselves.
Implications for Nursing Management
This study provided preliminary benchmarking material, affirmation for nursing management regarding the impact of training and competence screening policies and insight as to where to focus management attention. The study also highlighted that although FOU is clearly significant, it is possible for nurses operating in low-frequency event environments to achieve high self-perceived competence.
When a health system takes proactive responsibility for encouraging actual nursing competence (e.g., prescreening nurses, assessing and reassessing applied knowledge and skills, and targeting in-service training to address the known challenges of the population and catchment area), nurses’ professional self-esteem is likely to be high. Given that Al-Gharbia remains reliant on an expatriate nursing workforce, the message to management is that their investment in ensuring the competency of expatriate nurses is as vital as investment in modern equipment and infrastructure, and this investment is paying off. Such positive management behavior may contribute to nurse migration to this remote rural region and encourage retention and workforce stability.
Conclusions
The NCS was implemented to measure the SALC among RNs working in the public hospitals network in Al-Gharbia, UAE. This population produced a higher overall SALC score (84.3) than found in most previous studies. Public hospitals network nurses rate their professional competence as very good, and FOU is the variable most associated with SALC; results consistent with a stable nursing labor force. Al-Gharbia’s remote, rural, and desert environment appears to encourage resilience and adaptability.
The public hospitals network management encourages continual revalidation of the knowledge, skills, and competencies of its nurses. In this population, NCS items relating to students might have been open to interpretation and the associated FOU improbable. Even so, the reported SALC might be valid. As UAE-trained graduates and students are introduced into Al-Gharbia’s nursing workforce, such items will become more relevant. The present exploration of factors associated with nurses’ self-perceived competency found that the FOU of a competency item and “years of experience” had the most influence on self-assessment of competency.
This experience of using the NCS and the corresponding analyses provides insights for future managerial guidance. If implementing the NCS again, the present authors would consider scoping or explaining each item, removing irrelevant items, and developing strategies to address and minimize missing data. Collecting numerical data rather than categorical data for variables such as age, years of experience, and FOU would also enhance the analyses.
While use of the NCS as a management tool remains to be fully tested, the NCS provides guidance for directing future effort. Nursing management can investigate the adequacy of documentation, application of research into practice, and heightened use of existing data to support the sustainability of sound nursing outcomes. The alignment of the NCS with the existing performance-oriented competency matrix can also be examined.
Footnotes
Author Contributions
All the authors have contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.