
Abstract
Introduction
Burnout among nurses has emerged as a critical issue in healthcare and is gaining considerable attention due to its profound negative effects. The pervasive nature and significant effects that burnout might hold underscore the crucial need to assess this issue and its contributing factors among nurses. However, there is an evident gap in research precisely addressing this issue among nurses working in private hospitals in the Gulf Region.
Objective
This study aims to assess the prevalence and associated factors of burnout among nurses at private tertiary hospitals in Saudi Arabia and the United Arab Emirates.
Method
This is a cross-sectional study, and the data were collected by an electronic self-administered survey. This multicenter study involved a sample of 616 nurses and was performed in six different private tertiary care hospitals which belong to the largest private healthcare group in the Gulf Region. The Maslach Burnout Inventory—Human Services Survey was utilized to assess burnout levels.
Results
The study's results revealed that the overall burnout level was 67.2%. Notably, 82.8% of the participants were identified as having high Emotional Exhaustion (EE), 56.8% for high Depersonalization (DP), and 44.6% for low Personal Accomplishment (PA). The mean score for the EE dimension was 36.79 ± 10.34, the DP dimension was 13.91 ± 6.65, and the PA dimension had a mean score of 32.37 ± 7.73.
Conclusion
The conclusions revealed a significant prevalence of burnout among nurses working within the private sector in Saudi Arabia and the United Arab Emirates. This underscores the persistent problem of burnout among nurses, which necessitates targeted interventions.
Introduction
Burnout is a serious issue driven by unrelenting work-related stress. Burnout is a combination of psychological, emotional, and physical strain resulting from increased exposure to workplace stressors (Maslach et al., 1997). Nurse burnout is emerging as a critical healthcare issue and has received considerable attention due to its subtle negative impact on various aspects, including quality of life, nurse productivity, turnover rates, and medication administration errors (Jun et al., 2021; Kelly et al., 2021; Khatatbeh et al., 2022; Montgomery et al., 2021). The nature and possible negative effects of burnout have been recognized as critical when addressing this issue and the responses it has provided to nurses. Meanwhile, there may be a criticism, particularly relating to the issue of nurses working in private hospitals in Gulf countries.
Review of Literature
Burnout is considered to be among the most prevelant and frustrating characteristics associated with work in different jobs (Schaufeli et al., 2009). According to the 11th revision of the International Classification of Diseases (ICD-11), burnout is referred to as an occupational phenomenon that results from severe stress in the workplace that should not be overlooked (Harrison et al., 2021). Continued work stress, excessive workload, long working hours, and poor employee retention are all factors that can lead to burnout (Al-Omari et al., 2019; Cañadas-De La Fuente et al., 2015; Lin et al., 2021; Rotenstein et al., 2023).
Burnout manifests itself in three main dimensions, including Emotional Exhaustion (EE), Depersonalization (DP), as well as a strain on Personal Accomplishment (PA), all of which can particularly have a significant negative impact on nurses (Jun et al., 2021; Maslach, 2003). EE occurs when an individual experiences pain and emotional distress beyond work hours, and seems to be unable to attract the most emotional support or companionship. Meanwhile, the dimension of PA is a reduction in the participation of any personal aspect of work. With higher levels of burnout, individuals are more likely to experience a positive decrease in their self-efficacy behaviors and tasks, while at lower levels of personal self-efficacy, individuals are more likely to experience a decrease in self-efficacy behaviors and job performance. The physical, psychological, and interpersonal/social symptoms of burnout persist over time (Maslach & Jackson, 1981).
Generally, research shows that healthcare providers are at great risk of developing burnout due to the high level of stressors and being in a work environment that involves direct interactions with a high number of patients who have severe illnesses and deaths daily (Engelbrecht et al., 2008; Khamisa et al., 2013; Maslach, 2003). In reviewing previously published studies, the prevalence of burnout among nurses and other healthcare providers varies greatly and is influenced by the geographical region and the nature of work. While burnout prevalence was lowest in Central Asia and Europe, sub-Saharan regions of Africa reported the highest rates (Owuor et al., 2020; Woo et al., 2020). A high prevalence of burnout was reported among nurses (Frajerman et al., 2019; Khamisa et al., 2013; Rada & Johnson-Leong, 2004). Around 11.2% of nurses experience burnout worldwide (Woo et al., 2020). Around 37% of nurses in nursing homes and 33% of hospital nurses have experienced burnout (McHugh et al., 2011; Reith, 2018). A study reported that burnout levels were significantly associated with certain demographic factors, including nationality and the working unit. This suggests that these variables may play a key role in influencing burnout among nurses (Qedair et al., 2022). Another study also reported that demanding workloads and various aspects of the work environment, such as inadequate staffing ratios, poor communication between physicians and nurses, and a lack of organizational leadership, are commonly associated with burnout among nurses (Shah et al., 2024). Burnout has been well-documented among doctors, nurses, and frontline workers (Abdo et al., 2016), Egypt 2015 reported moderate burnout among 66% of the physicians and nurses in a tertiary care hospital, while (Youssef et al., 2022) Lebanon, reported moderate burnout among 90.7% of the study population. Puffer et al. (2017) demonstrated a burnout prevalence of 24.5% among U.S. physicians, while Wu et al. (2013) surveyed Chinese physicians of various specialities, demonstrating a burnout prevalence of 12.1%.
Upon reviewing the literature, it is evident that burnout can negatively impact well-being, job satisfaction, and mental health and is strongly associated with staff turnover, low morale, absenteeism, and other issues, all of which can have serious repercussions on the quality of patient care and safety (Al-Omari et al., 2019; Dall’Ora et al., 2020; Edú-Valsania et al., 2022; Lee et al., 2023; Salama et al., 2022). Given the profound negative influence that burnout can have on healthcare delivery and the limitedness of studies focusing specifically on nurses in private hospitals within Saudi Arabia and the United Arab Emirates, this study aims to assess the prevalence and associated factors of burnout among nurses at private tertiary hospitals in Saudi Arabia and the United Arab Emirates.
Method
Design
This study utilized an exploratory, descriptive, cross-sectional design. The data were gathered by an electronic self-administered survey that was distributed between January and March 2019, before the COVID-19 pandemic. Noting that the results reflect burnout levels in nurses before the onset of the pandemic, which may have had subsequent effects on burnout rates and healthcare work environments. This multicenter study was conducted in six private tertiary care hospitals belonging to the largest private healthcare group in Saudi Arabia and the United Arab Emirates. The data presented in this paper was gathered as part of a broader research project that aimed to explore the factors of burnout among private healthcare providers in Saudi Arabia (Al-Omari et al., 2019). While the original project included all healthcare providers, this article specifically focuses on nurses, narrowing the scope to provide a more detailed analysis of their burnout experiences. By concentrating on nurses, this study aims to identify key trends and associated factors that may otherwise be obscured in broader analyses involving multiple healthcare professionals.
Research Question
What is the prevalence of burnout among healthcare professionals in private hospitals in Saudi Arabia and the United Arab Emirates?
What are the key factors associated with burnout among healthcare professionals working in private hospitals in Saudi Arabia and the United Arab Emirates?
Sample
The study consisted of nurses working in the six selected private tertiary care hospitals across the Gulf region of KSA and the UAE, regardless of their nationality. This study focuses exclusively on the subset of nurses from the original project. From a total of 1,150 email invitations distributed, 900 responses were received. After removing incomplete, missing, and ineligible responses, 616 were included in the final analysis, allowing for a more in-depth analysis of factors specifically affecting nurses within the broader healthcare provider population. This study used a convenience sampling approach, and a power analysis was conducted prior to data collection to ensure that a sample of 616 would provide 80% power at a 95% CI to measure moderate effect sizes.
Data Collection and Instruments
An anonymous self-administered electronic survey was distributed via nurses’ email. An online survey was chosen because it expanded the capability of reaching the needed number of participants instantly. One-time access for each user was set in the survey settings to ensure that participants could submit the survey only once, thereby preventing replication. To ensure that the required sample size for the study was reached, follow-up emails were systematically distributed at 3-day intervals. This approach aimed to enhance participant engagement and maximize response rates by providing repeated reminders, thereby increasing the likelihood of participation, including among individuals who may not check their emails regularly.
This electronic survey consisted of two parts: sociodemographics and the Maslach Burnout Inventory—Human Services Survey (MBI-HSS). The sociodemographics had five items, including which hospital they work at, their gender (male/female), marital status (single/married/divorced) citizenship (citizen/noncitizen), and total years of experience (1–5 years/6–10 years/11 years and above), whilst the MBI had a total of 22 items. The MBI-HSS was utilized to assess burnout levels based on three dimensions, encompassing EE, DP, and PA. According to the literature, MBI-HSS has been extensively examined in numerous studies, and its reliability and validity have been proven (Lin et al., 2022; Maslach & Leiter, 2016). The Cronbach's alpha value calculated in this study was .871, which further supports the reliability of the measurement. The Cronbach's alpha coefficients for the subscales were EE at .85, DP at .716, and PA at .795. High scores in EE and DP, along with low scores in PA, indicate a higher risk of burnout. Based on the third edition of the MBI-HSS, the established cutoff points for identifying high levels are a score of 27 or higher for high EE, a score of 13 or higher for high DP, and a score of 31 or lower for high PA. Burnout was identified based on the criteria that include either “high EE and high DP” or “high EE and low PA” (Lim et al., 2019).
Ethical Approval and Informed Consent to Participate
Ethical approval was granted by the Institutional Review Board of the selected institution (Approval No. RC 18.11.21). Participation was completely voluntary, and the study survey included a consent statement indicating an agreement to take part in the study. Confidentiality was maintained throughout the study. Participants were assured that the gathered information would be used for research purposes only.
Statistical Analysis
Data were first entered into an Excel spreadsheet. Afterwards, the data were imported into Statistical Package for the Social Sciences (SPSS) version 29.0.1 for the analysis process. Missing values were handled using missing value analysis. To analyze the gathered data, both descriptive and inferential statistics were carried out. Mean and standard deviations were calculated as part of the descriptive statistics. To predict the statistical significance between the variables, independent samples t-test, analysis of variance (ANOVA), and correlational analysis were performed as appropriate. The study tested specific hypotheses related to differences in burnout dimensions across demographic variables. The variables tested included gender, marital status, citizenship, and years of experience. Specifically, independent samples t-tests were used to compare mean differences in the burnout dimensions based on gender and citizenship variables, while ANOVA was applied to assess differences across multiple categorical groups, including marital status and years of experience. Statistically significant results were determined based on a confidence interval of 95% and a p-value of ≤ .05. These thresholds were applied to assess the significance of the observed differences in burnout dimensions between the different demographic groups. Confidence intervals were used to estimate the range in which the true population parameter is likely to fall, ensuring the robustness and reliability of the findings.
Results
A total of 616 nurses were included in the current study to assess the prevalence and predictors of burnout among nurses at private tertiary hospitals in Saudi Arabia and the United Emirates. The demographics of the current study showed that the majority of participants were female, and more than half were single. Approximately half of the participants had between 1 and 5 years of experience. As illustrated in Table 1, among the participants, 518 (84.1%) were female, 312 (52.3%) were single, and 279 (45.3%) were married, 584 (94.8%) were foreign nurses. 284 (46.1%) had 0–5 years of experience, and 267 (43.3%) had 6–10 years of experience.
Nurses’ Sociodemographics (n = 616).
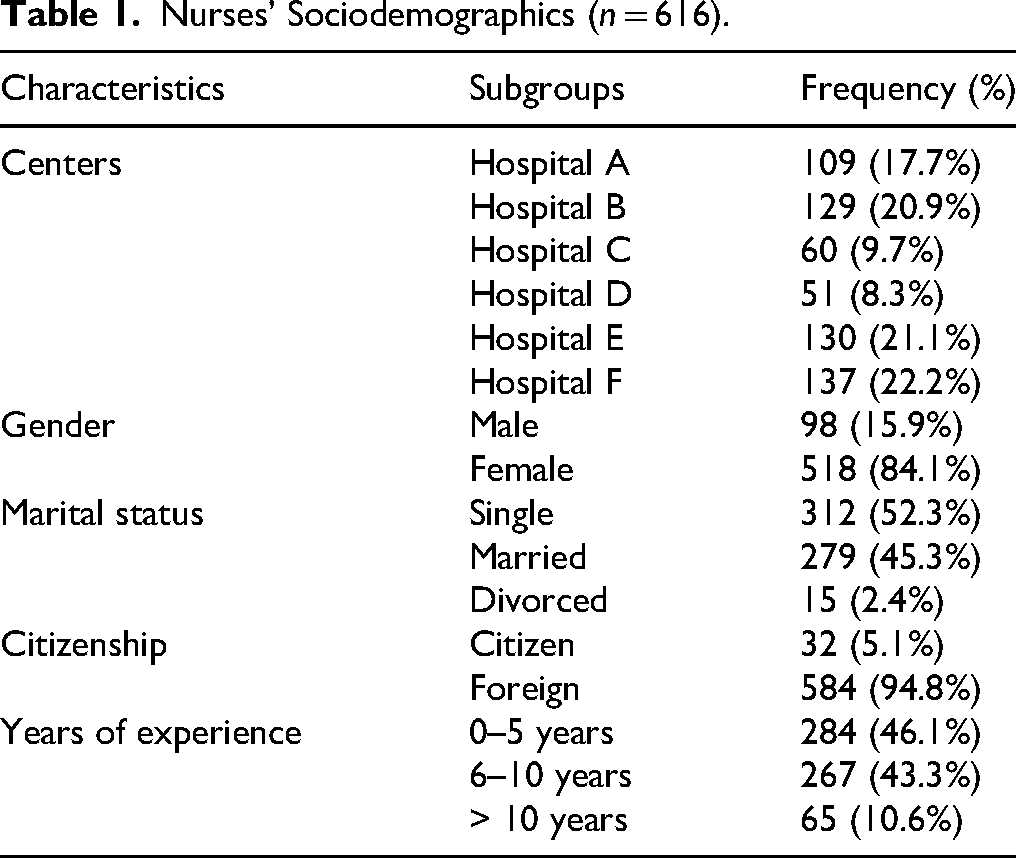
Table 2 presents descriptive statistics for burnout dimensions. The mean score for the EE dimension was 36.79 ± 10.34, the DP dimension had a mean score of 13.91 ± 6.65, and the PA dimension had a mean score of 32.37 ± 7.73.
Descriptive Statistics for Burnout Dimensions.

Table 3 presents the prevalence of burnout and its dimensions among nurses. The analysis indicated that 82.8% of the participants were identified as high for EE, 44.6% high for DP, and 56.8% for low PA. The overall burnout level was 67.2%.
Prevalence of Burnout and its Dimensions Among Nurses.

The relationship between the dimensions using inferential statistics, and their correlation was calculated and examined by heatmap correlation and computed by Pearson's Correlation r. EE and DP have the strongest correlation (r = .62), suggesting that as EE increases, DP also tends to increase. PA is positively correlated with both EE and DP (r = .29 and .30, respectively), but these correlations are weaker compared to the correlation between EE and DP (Figure 1).

Heatmap of Burnout Levels/dimensions. EE: Emotional Exhaustion, PA: Personal Accomplishment, DP: Depersonalization R = −1 to +1.
Table 4 presents the associations between participants’ sociodemographic characteristics and burnout dimensions. The study revealed significant differences in EE based on citizenship and years of experience, while gender and marital status did not show statistically significant differences. Foreign nurses exhibited higher EE levels (36.99 ± 10.24) compared to citizens (33.06 ± 11.68, p-value = .036), suggesting that noncitizen nurses may experience greater work-related stress, possibly due to challenges related to workplace integration and job security. Similarly, nurses with less experience (0–5 years) had significantly higher EE levels (37.48 ± 9.29) compared to those with over 10 years of experience (33.66 ± 10.80, p-value = .027), indicating that early-career nurses may be more susceptible to burnout due to increased job demands and limited coping strategies. However, there were no significant differences in EE between male (37.15 ± 10.39) and female nurses (36.73 ± 10.34, p-value = .717) or across marital status categories (p = .153). Differences in EE, PA and DP levels were found across different hospitals. PA and DP did not show significant variations across any of the remaining sociodemographic variables.
Participants’ Sociodemographics and Burnout Dimensions Mean Comparisons (n = 616).

Note. EE = emotional exhaustion; PA = personal accomplishment; DP = depersonalization.
**p-value ≤ .05.
Generalized Linear Model Between Burnout and Demographic Factors
A multivariate generalized linear model (GLM) is a type of regression model that is applied to measure the strength of the relationship between burnout levels (multivariate) and other associated factors. Table 5 presents the GLM for predicting different dimensions of burnout based on demographic variables. In this case, the dependent variables considered were EE, PA, and DP while the independent variables consisted of gender, marital status years of experience, centers, and nationality. The multivariate GLM analysis used to model and predict burnout dimensions based on demographic factors showed that for centers, there were highly significant effects across all burnout dimensions: EE (F = 21.638, p-value < .001), PA (F = 6.624, p-value < .001), and DP (F = 1082.762, p-value < .001). These results suggest that burnout levels differ significantly across centers. As for gender, no significant effects were found with EE (F = 0.056, p-value = .813), PA (F = 0.025, p-value = .875), or DP (F = 0.209, p-value = .648), indicating that gender does not play a significant role in burnout.
Multivariate GLM of Modeling and Predicting Different Burnout Dimensions With Demographics.
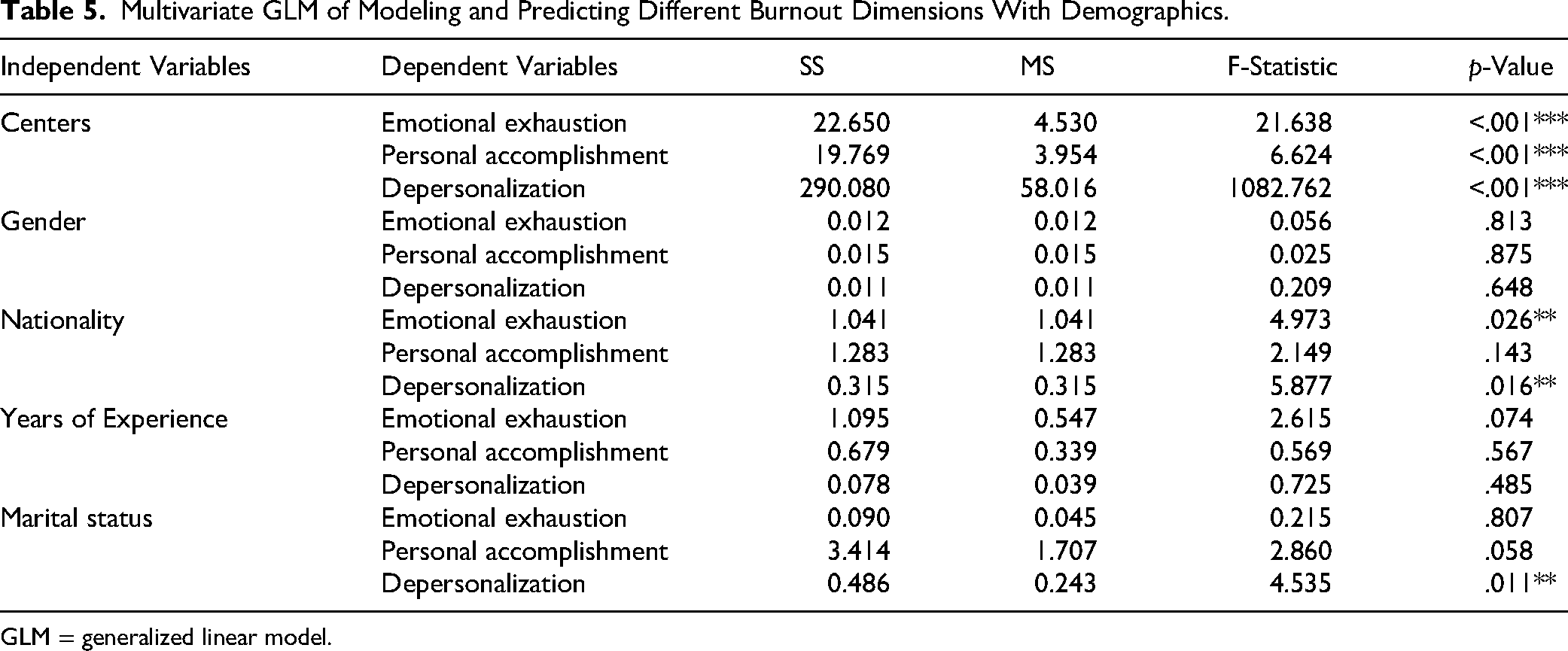
GLM = generalized linear model.
Nationality had a significant effect on EE (F = 4.973, p = .026) and DP (F = 5.877, p = .016), but not on PA (F = 2.149, p = .143), suggesting that foreign nurses may experience higher emotional exhaustion and depersonalization compared to citizens. Years of experience did not show significant effects for EE (F = 2.615, p = .074), PA (F = 0.569, p = .567), or DP (F = 0.725, p = .485). Lastly, marital status was not significantly related to EE (F = 0.215, p = .807), but had a marginally significant effect on PA (F = 2.860, p = .058) and a significant effect on DP (F = 4.535, p = .011), suggesting that marital status may influence depersonalization (Table 3).
Discussion
The study revealed that the overall burnout level was 67.2%. Notably, 82.8% of participants were identified as high for EE, 56.8% for high DP, and 44.6% for low PA. These findings collectively indicate a significant prevalence of burnout among nurses working in the private sector among nurses from six different centers. Further analysis of burnout levels on sociodemographic variables revealed perceived differences. The foreign nurses recorded higher levels of EE (36.99 ± 10.24) than their mother counterparts (33.06 ± 11.68, p-value = .036), suggesting that nonmother nurses may experience greater work-related stress, possibly because my returns mimic the hams of workplace adaptation or lack of job security. Similarly, experience level played a role in burnout, with nurses with maybe 0–5 years of experience showing higher EE (37.48 ± 9.29) compared to those with higher individual experience (33.66 ± 10.80). Al-Omari's (2019) study, which is more extensive in scope, agrees with recent studies in highlighting that nurses experienced a higher rate of burnout compared to other health care professionals. The same study recognized nursing as a profession in particular with high levels of EE and burnout. The high rate of burnout observed in this study has been consistent with previous reports from other Gulf Region countries (Abdelrazek & Higazy, 2023; Chemali et al., 2019; Elbarazi et al., 2017). Similarly, recent studies have reported high rates of job compliance among nurses in Iran, a neighboring Gulf country (Khammar et al., 2018; Sohrabi et al., 2022). The case of those who have been dismissed can be explained in terms of lack of time and excessive workload. A review of 91 research papers theorized that high workload, lack of work and long shift times were associated with higher levels of compliance among nurses (Dall'Ora et al., 2020). The excessive workload and inadequate training resulting from deficiencies in nursing skills can contribute to higher levels of DP, namely more awareness of psychological and physical health problems of nurses.
Similarly, recent studies reported a high prevalence of job burnout among nurses in Iran, a neighboring country to the Gulf (Khammar et al., 2018; Sohrabi et al., 2022). Such findings might be explained by the staff shortages and work overload. A review of 91 research papers theorized that high workload, staffing shortage and long shift hours are linked to higher levels of burnout among nurses (Dall’Ora et al., 2020). Work overload and insufficient training resulting from nursing staff shortages may contribute to higher DP levels, making nurses more prone to psychological and physical health problems.
This study found that study members exhibited higher levels of EE compared to DP and PA. Possible reasons for this include staff shortages and workload. A systematic review and meta-analysis suggested that nurses, particularly in primary care who care for chronically ill patients, often develop empathy and close relationships with their patients (Monsalve-Reyes et al., 2018). This relationship may enhance the quality of care, thereby reducing DP and promoting a greater sense of personal achievement (Bicker et al., 2015). The study results are in agreement with the literature reporting on burnout when using the MBI-HSS tool. Nurses often reported that EE was due to the complex nature of the care they provide (Poku et al., 2020). In addition, one study found that reducing overload and increasing safety can prevent burnout (Gómez Sánchez et al., 2009). Nurses who experienced EE were more likely to exhibit higher levels of DP, because emotional strain increased feelings of detachment and loyalty. The complexity of this interplay increased the psychological and physical demands of the nurses and could be reflected in the mutual reinforcement traces of EE and DP. One study in the literature has investigated the relationship between demographic characteristics and dimensions of burnout (Al-Turki et al., 2010; Cañadas-de La Fuente et al., 2014; Chen et al., 2022; Choi et al., 2018; Galvez-Arevalo et al., 2023; Ramirez-Elvira et al., 2021). In this study, there was a positive association between health levels and EE, with foreign nurses showing higher levels of EE compared to their peers. In this study, samples from private institutions were the most common among foreign institutions, accounting for 94% of the sample. Because foreign nurses showed higher levels of EE, the study identified the potential for increased burnout as a pressing issue within the private sector. This observation is highly supported in the literature, as non-Saudi nurses experienced better EE compared to their Saudi counterparts (Al-Turki et al., 2010). Recently, a study found that Saudi nurses are more likely to be emotionally aware than their foreign counterparts, highlighting other issues (Qedair et al., 2022). In this study, high EE scores were affected by the years of experience. This aligns with a previous research article, in which it was reported that poor professional experience is one of the main factors associated with burnout (Ramírez-Elvira et al., 2021). A higher PA score in nurses with more advanced work experience could be associated with their own more positive attitudes toward their abilities, having the same years of experience (Faria & Maia, 2007; Hussein, 2018). The results of our study found no positive effects of marriage and marital age on measures of burnout. Similarly, many studies have observed that burnout does not affect marriage and marital survival. In contrast, recent studies have reported differences in the traces of the effects of marriage and marital age, except for one study by Choi et al. (2018) reported that marriage is associated with higher EE due to balancing family and work responsibilities. Additionally one study (Cañadas-De La Fuente et al., 2015) found that being male and being single or divorced was associated with higher levels of burnout among nurses. In a study by Al-Omari et al. (2019) when EE was examined particularly among nurses, no significant differences were found between male and female nurses, although there was a significant difference in EE levels among the whole sample of the healthcare. The specific pattern being observed is that men in other healthcare professions were more likely to have lower levels of EE, while women in other professions are more likely to have higher levels of EE.
Strengths and Limitations
The main strength of the study is including nurses from multiple private-sector institutions in Saudi Arabia and the United Arab Emirates. The study captures a broader and more representative snapshot of burnout prevalence. The main limitation of the study is the use of convenience sampling methodology may introduce selection bias to some extent and can therefore limit the generalizability of findings. Participants of the study may not represent the broader population, potentially affecting the external validity of the results. Additionally, self-reported data could be subject to response bias. Additionally, while this design is sufficient for assessing the prevalence of burnout, it provides limited insight into the intention to leave the profession due to burnout. Future research could address this limitation by employing a longitudinal or qualitative study to explore this aspect in more depth.
Implications for Practice
The findings of this study have significant implications for healthcare management and policy in private hospitals across Saudi Arabia and the United Arab Emirates. By identifying the prevalence and associated factors of burnout among healthcare professionals, this research highlights the urgent need for targeted interventions to support staff well-being and sustain workforce productivity. Implementing organizational policies that promote work–life balance, recognition, and professional development may help mitigate burnout risks.
Conclusions
The findings revealed a significant prevalence of burnout among nurses working within the private sector in Saudi Arabia and the United Arab Emirates. The results of this study underscore the pervasive problem of burnout among nurses, highlighting the need for targeted interventions. Given that the risk of burnout was higher among foreign nurses and those with less experience, targeted interventions specifically for those groups should be developed to tackle this issue. Interventions should focus on providing support, cultural competence training, and stress reduction programs. Additionally, newer nurses with less experience should receive mentorship and professional development to build resilience. Further research is needed to explore the long-term subsequent effects of burnout on quality indicators within clinical practice. Future studies should also investigate the effectiveness of specific interventions in reducing burnout, improving job satisfaction, and enhancing patient care outcomes, while also examining the role of organizational support and leadership in mitigating burnout among healthcare workers.
Supplemental Material
sj-doc-1-son-10.1177_23779608251350578 - Supplemental material for Prevalence and Associated Factors of Burnout Among Nurses at Private Tertiary Hospitals in the Gulf Region: A Cross-Sectional Multicenter Study
Supplemental material, sj-doc-1-son-10.1177_23779608251350578 for Prevalence and Associated Factors of Burnout Among Nurses at Private Tertiary Hospitals in the Gulf Region: A Cross-Sectional Multicenter Study by Abbas Al Mutair, Kawthar Alsaleh, Awatif Alrasheeday, Noura Almadani, Hanan Alyami, Muhammad Daniyal and Sana Almahmoud in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608251350578 - Supplemental material for Prevalence and Associated Factors of Burnout Among Nurses at Private Tertiary Hospitals in the Gulf Region: A Cross-Sectional Multicenter Study
Supplemental material, sj-docx-2-son-10.1177_23779608251350578 for Prevalence and Associated Factors of Burnout Among Nurses at Private Tertiary Hospitals in the Gulf Region: A Cross-Sectional Multicenter Study by Abbas Al Mutair, Kawthar Alsaleh, Awatif Alrasheeday, Noura Almadani, Hanan Alyami, Muhammad Daniyal and Sana Almahmoud in SAGE Open Nursing
Footnotes
ORCID iDs
Author Contributions
Conceptualization: A.A.M. and A.A.; methodology: S.A. and A.A.M.; formal analysis: A.A.M., H.A., M.D., and K.A.; data curation: S.A. and K.A.; writing—original draft preparation: S.A., A.A., H.A., M.D., and N.A.; writing—review and editing: K.A. and S.A.; supervision: A.S. and A.A.M.; All authors have read and agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Princess Nourah Bint Abdulrahman University Researchers Supporting Project number (PNURSP2025R386), Princess Nourah Bint Abdulrahman University, Riyadh, Saudi Arabia.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.