
Abstract
This cross-sectional study of individuals seeking outpatient musculoskeletal specialty care investigated whether lower general interpersonal trust, measured using the validated Interpersonal Trust Scale (ITS), is associated with worse patient experience as measured with the Trust and Experience with Clinician Scale (TRECS-7). A total of 294 adult patients completed TRECS-7, ITS, as well as measures of levels of unhelpful thoughts and distress regarding sensations, social health, and personal health agency. There was no correlation between ITS and TRECS scores. K-means cluster analysis identified four statistical subgroups of patient psychosocial factors. Higher mean TRECS-7 scores were observed in clusters characterized by high personal health agency and favorable psychosocial health, while lower mean clinician-specific trust scores were seen in clusters with low agency and problematic psychosocial health–independent of levels of general interpersonal trust. In the context of musculoskeletal specialty care, difficulty establishing trust with a patient may therefore signal relatively low personal health agency, highlighting a potential target for health and care strategies aimed at enhancing experience.
Level of evidence
III (Observational, Cross-sectional Study).
Keywords
Introduction
Background
Measures of patient experience, including perceived clinician empathy, communication effectiveness, and willingness to recommend care, are intercorrelated and exhibit substantial ceiling effects.1,2 When a notable proportion of patients assign the highest possible ratings, the capacity to detect meaningful variation and identify modifiable factors across clinicians or care settings becomes limited.3-5 To address this concern, our study team developed The Trust and Experience with Clinicians Scale (TRECS), a patient experience measure designed to produce a more normally distributed range of scores with reduced ceiling effects, in order to facilitate the investigation of psychosocial and contextual factors associated with ess favourable care experiences. 6
Rationale
Initial studies utilizing TRECS found that psychosocial factors, such as unhelpful patterns of thinking and feelings of distress, explain only a small proportion of the observed variation in scores among musculoskeletal patients.4,6 In light of this, two potentially relevant patient-level factors are the concept of interpersonal trust (an individual’s general tendency to trust others7,8) and personal health agency (a patient’s perceived ability and confidence to manage their own health and engage effectively in healthcare decisions9,10). Both constructs may plausibly influence clinician-specific trust: individuals with lower generalized interpersonal trust may also find it more difficult to trust clinicians, whereas those with lower personal health agency may report less positive care experiences when faced with decisions that emphasize active participation in health management, appropriate boundary setting and shared responsibility for care, rather than passive models of care characterized by low value tests and treatments.
Because patient-reported subjective measures tend to be interrelated, traditional multivariable analyses may be distorted by collinearity of the variables. To address this, the statistical technique of K-means cluster analysis can be used to identify groupings of people based on patterns in the relative mean scores across these measures (clusters) 11 .
Questions
In a cross-sectional survey of musculoskeletal outpatients, we asked: (1) Do levels of patient experience, as measured using TRECS-7, differ across statistical clusters defined by levels of generalized interpersonal trust, unhelpful thoughts, feelings of distress, social health, and personal health agency? and (2) Which factors are independently associated with patient self-reported trust and experience with the clinician?
Methods
Study Design and Setting
This cross-sectional study was conducted in an urban outpatient musculoskeletal specialty care setting. Eligible patients were recruited after a consultation with a specialist. Verbal informed consent was obtained, and survey completion constituted implied consent. A brief online survey was administered via REDCap (Vanderbilt University; Nashville, TN) using either a researcher-provided tablet or, in less than 10% of cases, a patient’s personal device–a method that was discouraged due to its association with incomplete records.
Inclusion Criteria
We enrolled new or return adult (18 years or older) patients with written and verbal proficiency in English or Spanish. Individuals were excluded if they had cognitive or physical impairments that precluded completion of the questionnaire.
Outcome Measures
Response Variables
The primary outcome was patient experience of care measured using the TRECS-7 (Trust and Experience with Clinicians Scale), a validated seven-item instrument with scores ranging from 7 to 35, where higher scores reflect greater trust in the clinician. 6
Explanatory Variables
General interpersonal trust was assessed using the 5-item Interpersonal Trust Scale (ITS; score range 5 to 25), with higher scores indicating greater levels of interpersonal trust. 8 Unhelpful thoughts and feelings of distress regarding symptoms were each measured using separate 3-item scales derived through factor analysis (range 3 to15). 12 Social health was assessed using a validated 9-item questionnaire (score range 9 to 45) 13 and personal health agency was measured using a brief, 3-item scale derived from the Patient Activation Measure (PAM);score range 3-15)9,10 Higher scores on the unhelpful thoughts, feelings of distress, and social health scales indicated more negative psychosocial health. Higher personal health agency scores reflected greater self-efficacy in managing one’s own health (agency).
Demographic information collected included age, gender, preferred language, marital status, educational attainment, employment status, annual household income, and insurance status. The recruiting researcher also recorded patient status (new or returning), clinic subspecialty, and treating clinician. Participants were additionally asked about prior employment in the healthcare sector and any previous negative healthcare experiences.
Statistical Analysis
Descriptive statistics were used to summarize participant characteristics. Continuous variables are reported as means and standard deviations, while categorical variables were reported as frequencies and percentages.
Subgroups with fewer than 15 observations were consolidated for statistical analysis. Participants identifying with a non-binary or other gender identity were randomly and evenly reassigned to male or female groups for analytic purposes. To identify natural groupings of participants based on measures of the subjective (e.g., interpersonal trust, unhelpful thoughts, distress, social health, and personal health agency), an unsupervised k-means cluster analysis was performed. The optimal number of clusters was determined using the elbow method and silhouette coefficients. Mean TRECS-7 scores were then compared across the resulting statistical groupings using ANOVA or Kruskal-Wallis tests, with post-hoc pairwise comparisons between clusters performed using chi-square tests and adjusted using Bonferroni correction.
Bivariate analyses, including t-tests, Kruskal-Wallis tests and Spearman correlations (depending on variable types), were used to assess associations between explanatory variables and TRECS-7 scores. Variables associated at p < 0.10 were entered into multivariable linear regression models to identify independent predictors. Statistical significance was set at p < 0.05. All analyses were performed using Stata version 18.0 (StataCorp, College Station, TX).
Sample Size Calculations
Sample size was estimated a priori using G*Power (version 3.1) for a one-way ANOVA to detect differences in TRECS-7 scores across three clusters. Assuming a moderate effect size (f = 0.25), α = 0.05, and 80% power, the required sample size was determined to be 159 participants (53 per cluster). To account for subgroup analyses, potential clustering instability, and missing or incomplete data (up to 20%), the target enrolment was increased to 300 participants.
Description of Study Population
Demographics of 294 New and Return Patients Presenting to the Musculoskeletal Specialty Clinic for Review
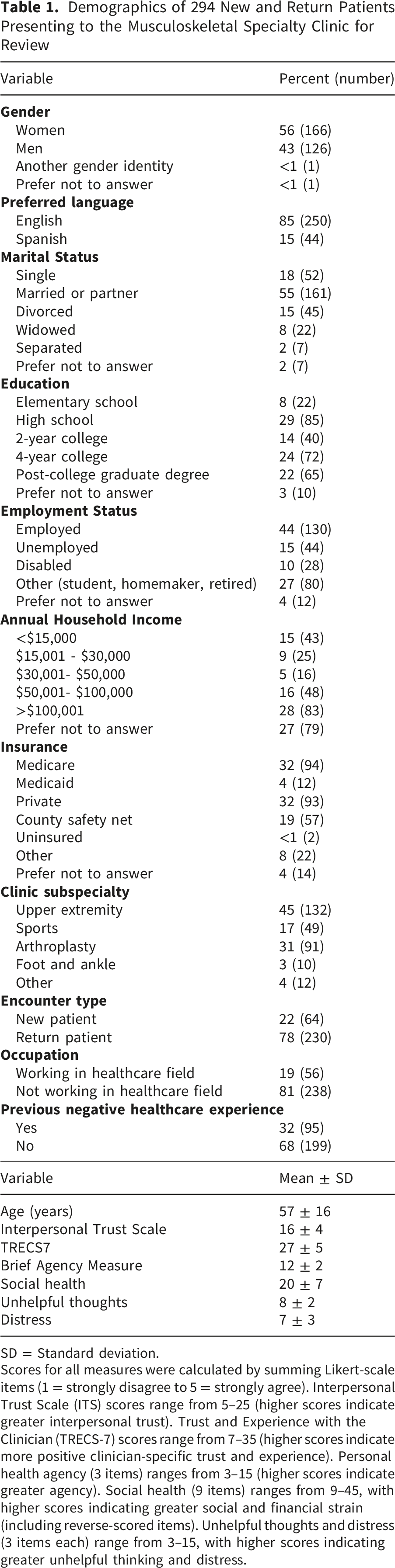
SD = Standard deviation.
Scores for all measures were calculated by summing Likert-scale items (1 = strongly disagree to 5 = strongly agree). Interpersonal Trust Scale (ITS) scores range from 5–25 (higher scores indicate greater interpersonal trust). Trust and Experience with the Clinician (TRECS-7) scores range from 7–35 (higher scores indicate more positive clinician-specific trust and experience). Personal health agency (3 items) ranges from 3–15 (higher scores indicate greater agency). Social health (9 items) ranges from 9–45, with higher scores indicating greater social and financial strain (including reverse-scored items). Unhelpful thoughts and distress (3 items each) range from 3–15, with higher scores indicating greater unhelpful thinking and distress.
Participants reported moderate interpersonal trust, high personal health agency and high measured trust in the clinician, while social health, unhelpful thoughts, and distress were all generally moderate to low (Table 1).
Results
Clusters Associated With Trust and Experience in the Clinician
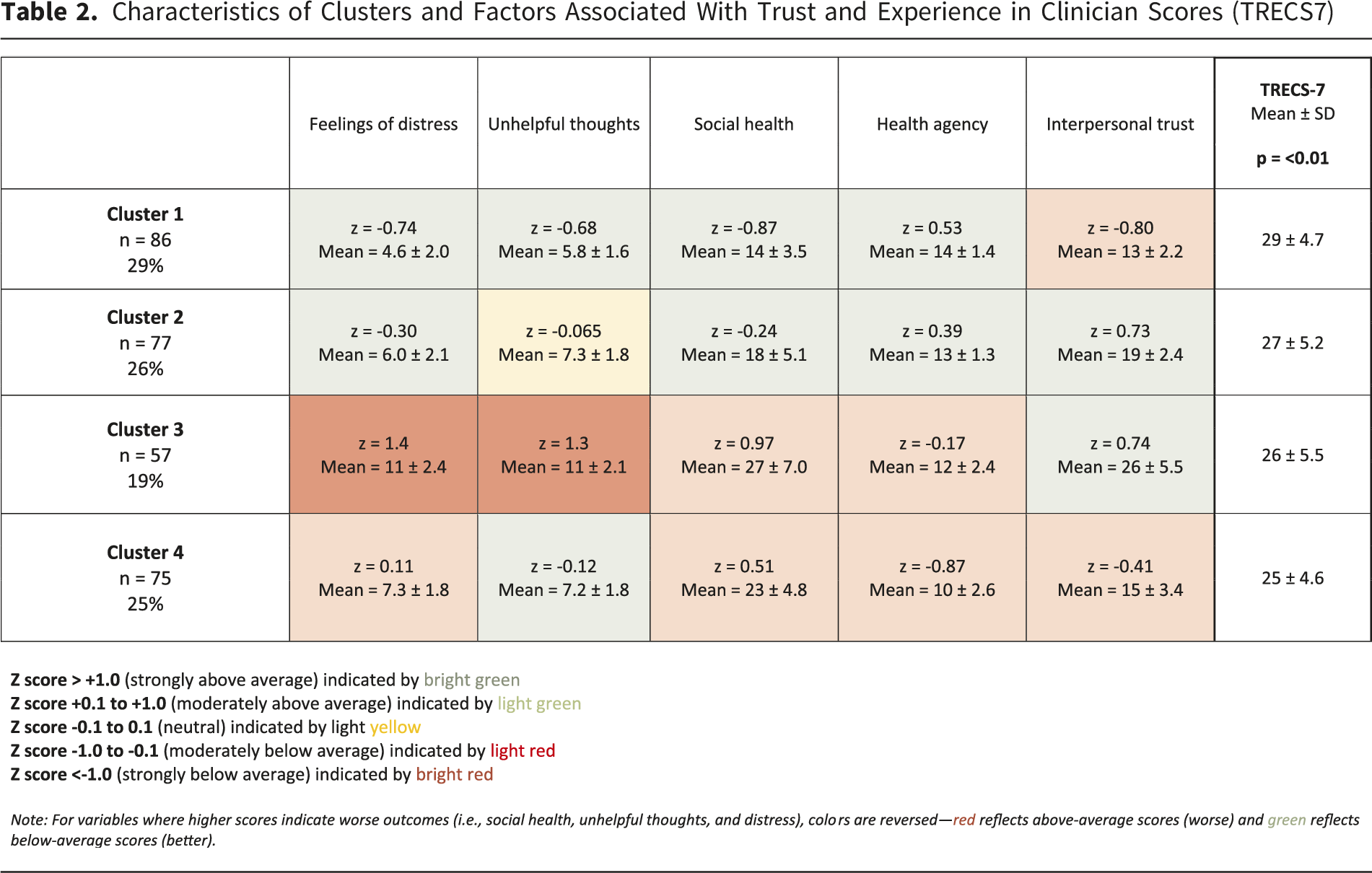
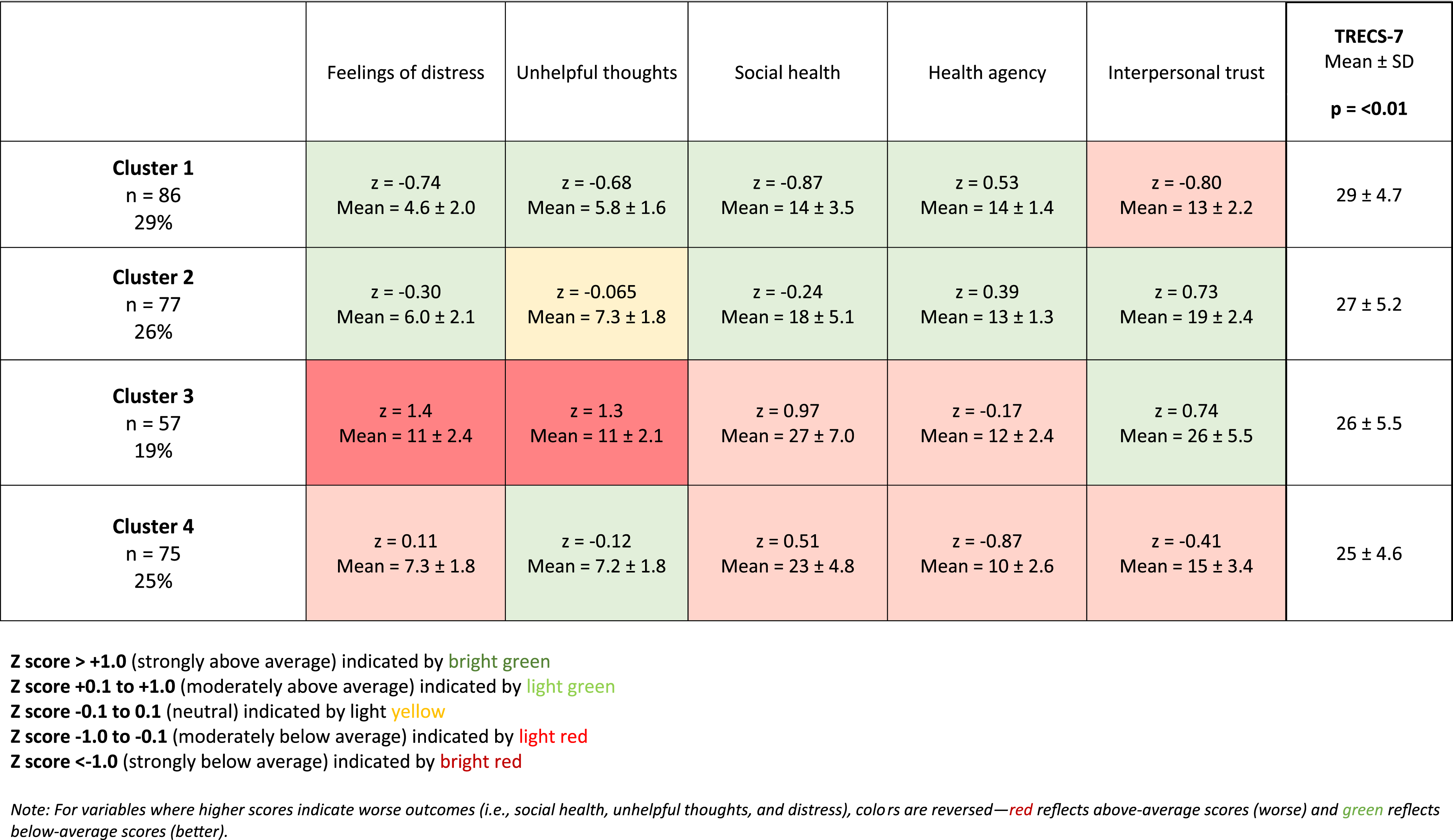
Characteristics of Clusters and Factors Associated With Trust and Experience in Clinician Scores (TRECS7)
Post-hoc Pairwise Comparisons of TRECS-7 Scores Between Clusters
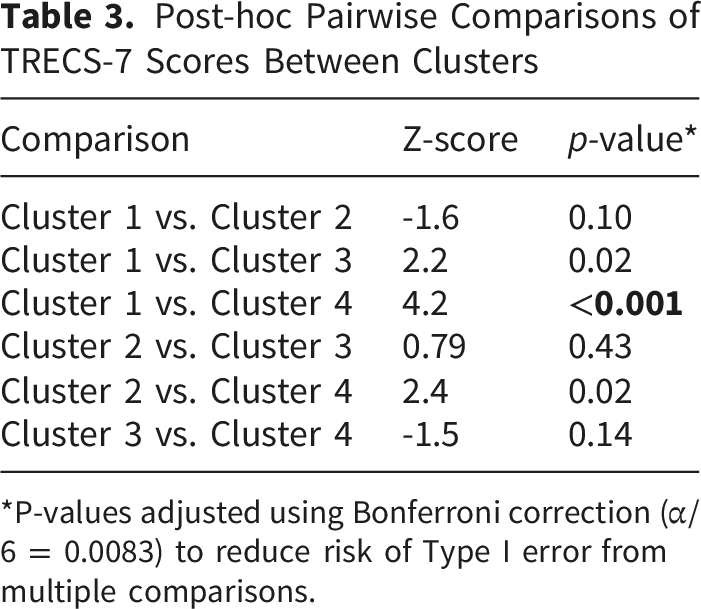
*P-values adjusted using Bonferroni correction (α/6 = 0.0083) to reduce risk of Type I error from multiple comparisons.
Factors Associated With Trust and Experience in the Clinician
Bivariate Analysis of Factors Associated With Trust and Experience in the Clinician (TRECS7)
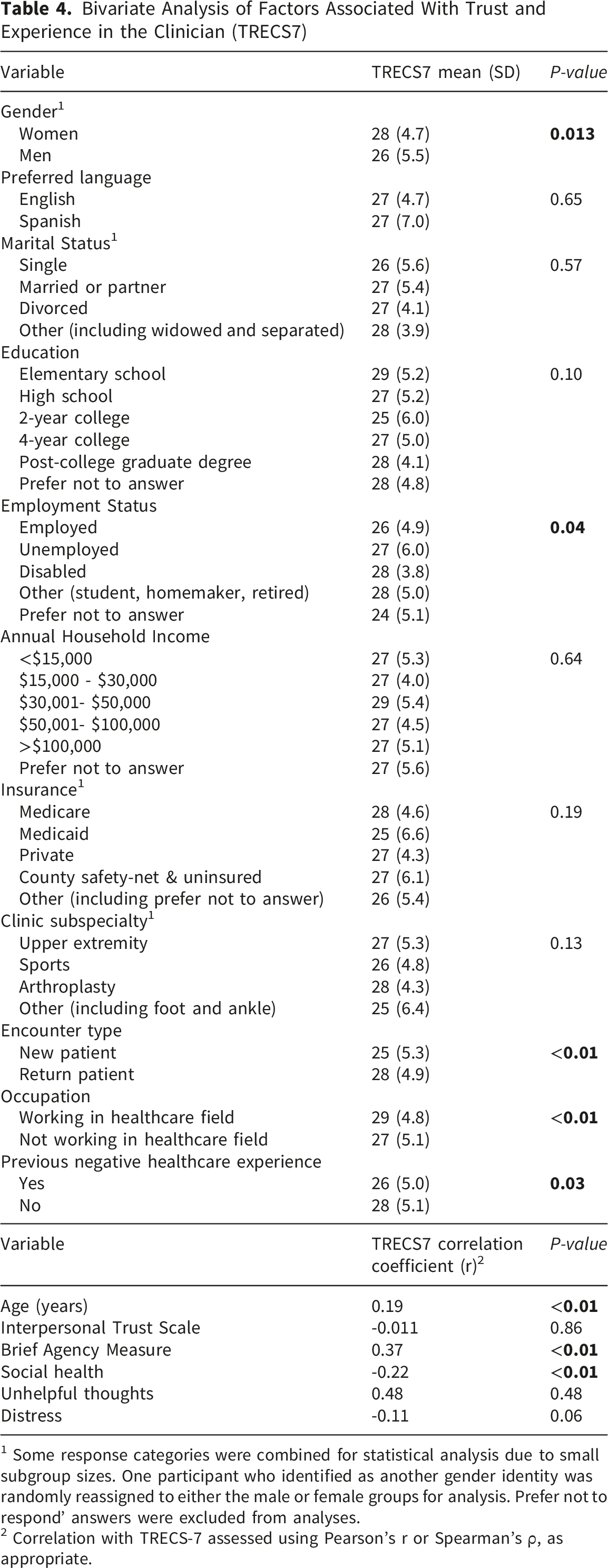
1 Some response categories were combined for statistical analysis due to small subgroup sizes. One participant who identified as another gender identity was randomly reassigned to either the male or female groups for analysis. Prefer not to respond’ answers were excluded from analyses.
2 Correlation with TRECS-7 assessed using Pearson’s r or Spearman’s ρ, as appropriate.
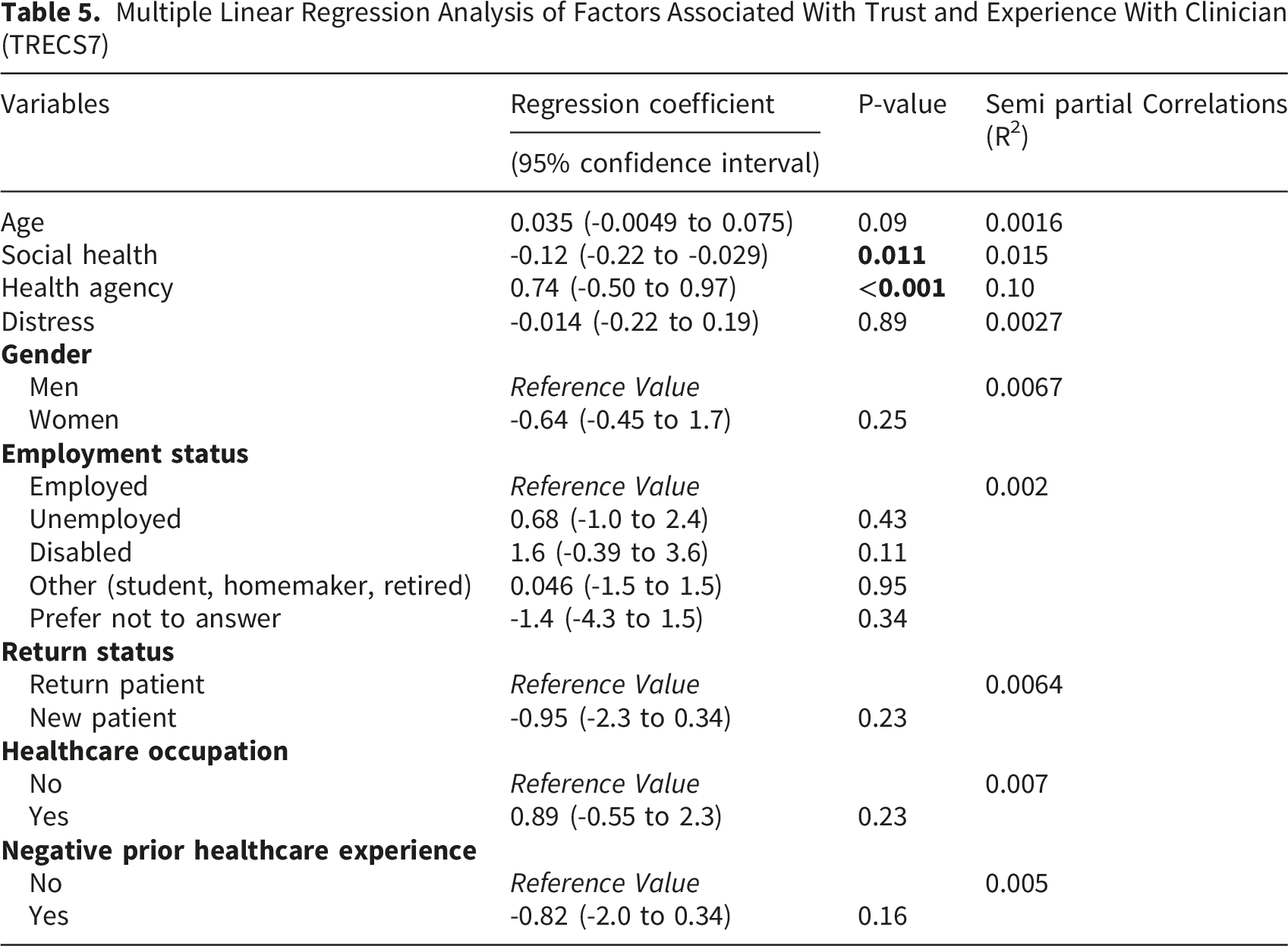
Multiple Linear Regression Analysis of Factors Associated With Trust and Experience With Clinician (TRECS7)
Discussion
Background, Rationale, and Key Results
Patient trust in the clinician is a key determinant of overall care experience. We hypothesized that people who find it difficult to trust others in general (low interpersonal trust) may similarly struggle to trust their clinician. In this cross-sectional study, we tested this hypothesis and found that greater trust and experience with the clinician was instead associated primarily with greater personal health agency, and, to a lesser degree, with better social health, but not with general interpersonal trust. When clinicians encounter difficulty in developing trust with a patient, this may therefore serve as a potential indicator of relatively low personal health agency and signal a need to implement care-team strategies that enhance agency and address social disadvantage.
Limitations
There are several possible limitations to consider when interpreting the findings of this study. First, the results may be most applicable to people seeking musculoskeletal specialty care in our region from the participating clinicians, although the observed associations may be reproducible to the degree that they correspond with human traits. As a cross-sectional study, these findings reflect associations and do not establish causal relationships. Second, the use of self-reported measures introduces potential sources of bias, including recall bias, selection bias, and social desirability bias. These concerns are particularly relevant given the sensitive nature of items related to interpersonal or clinician trust, mental, and social health. Since the sample consists of individuals actively seeking care, there may be an inherent selection bias toward people who are more trusting of clinicians. Steps were taken to mitigate the risk of social desirability bias, including assuring patients of anonymity, clarifying that survey responses would not impact clinical care, and use of a scale developed to reduce ceiling effects (TRECS7). 6 While there is evidence that patients may not complete mental health measures forthrightly,14,15 this limitation may blunt, but does not eliminate, the ability to detect meaningful associations.
Clusters Associated With Trust and Experience in the Clinician
The finding that clinician-specific trust among musculoskeletal outpatients clusters according to patients’ psychosocial profiles, independent of general interpersonal trust, highlights the relative importance of unhelpful thoughts, distress, social health and personal health agency in shaping patient experience. This aligns with evidence that generalized interpersonal trust is more closely associated with stable personality traits, including self-esteem, optimism, extraversion, agreeableness, and cognitive complexity, rather than with specific care experiences.16,17,18 Interpersonal trust also varies according to broader social norms and community structures, with cross-sectional research indicating trust in close relationships (i.e., family members or neighbors) tends to be consistently high across societies, while trust in strangers often varies considerably between cultural contexts.19,20 Notably, even in cultures characterized by lower generalized trust in outsiders, trust in physicians often remains high– further supporting the lack of association between general interpersonal trust and clinician-specific trust.21,22
The identification of statistical groupings of similar levels of psychosocial factors associated with differing levels of clinician-specific trust should not be interpreted as encouragement to categorize patients, as this may inadvertently reinforce mental health stigma. Rather, these groupings are a necessary part of the statistical technique (used to limit distortion in traditional multivariable models) and serve to illustrate how measures of the subjective relate to one another and to the outcome. Psychosocial factors, including mental health, exist on a continuum and should be interpreted accordingly. The near-linear relationship observed between personal health agency and clinician-specific trust in this study supports the validity of these measures and underscores the relevance of psychosocial factors in shaping patient experience across their full range. Clinically, the findings indicate that lower clinician-specific trust is associated with modifiable factors, such as low personal health agency, social disadvantage, and less healthy mindsets–providing actionable targets for interventions aimed at improving patient experience.
Factors Associated With Trust and Experience in the Clinician
The finding that trust and experience with the clinician is notably associated with personal health agency, with social health contributing an important additional independent association, offers practical guidance for structuring effective care strategies. Clinicians can prioritize trust-building in every encounter and recognize difficulty establishing trust as a potential indicator of lower personal health agency. Supporting patients’ confidence in managing their own health–for instance, through strategies that foster personal health agency, such as emphasizing independent exercises rather than “physical therapy” (by both the musculoskeletal specialist and the physical therapist), or by guiding patients toward effective over-the-counter options rather than defaulting to prescription analgesia –may reinforce autonomy. 10 However, the impact of these strategies on patient experience may vary depending on the patient’s mindset. For patients with lower personal health agency, who may prefer to take a more passive approach to their health and care, this strategy may not align with expectations and could adversely affect experience metrics in the short term. Accordingly, clinicians should tailor their approach to the patient’s level of readiness, with the aim of gradually fostering greater health agency over time. 10
Evidence from other clinical contexts supports the relevance of this approach. For example, in patients with diabetes, greater self-efficacy has been associated with higher trust in physicians and has been shown to mediate the relationship between trust, treatment adherence, and clinical outcomes.23-25 Most previous work, however, has focused on task-specific self-efficacy (e.g., glucose control or inhaler use), rather than broader constructs such as personal health agency. Future research might examine how care strategies designed to prioritize and nurture general health agency influence patient experience. In practice, when clinicians observe that a patient is having an unpleasant care experience or difficulty developing trust, this may prompt attention to their own communication and relationship-building strategies as well as engagement of the broader health team to support greater health agency. Conversely, care teams that effectively promote personal health agency may occasionally receive unfavorable patient experience ratings. In such instances, infrequent negative feedback related to appropriate boundary setting may be an inherent component of high-quality, effective care.
The greater distress, unhelpful thinking, and compromised social health observed in groups with lower health agency are themselves also modifiable. Tactics for improving agency and patient experience may therefore benefit from concurrently addressing psychosocial aspects of health. Limited trust and worse experience with the clinician intersect with patient personal factors.1,4,7 Understanding this can inform comprehensive care approaches designed to improve personal health agency, reduce distress, and guide people to a healthier understanding of their condition. Additionally, the modest association between greater social disadvantage and lower trust and experience with clinicians aligns with previous findings that unmet social needs can erode patients’ trust in the healthcare system.26,27 Similarly, trust in physicians has also been linked to social capital, defined as the strength and extent of an individual’s social networks. 28 Paradoxically, evidence suggests patients of lower socioeconomic status, despite often exhibiting decreased trust in clinicians, are generally less likely to question medical advice and more likely to adhere to recommendations.29-32 This dynamic creates a risk that distrust among this group may go undetected by clinicians, thereby limiting opportunities for timely intervention.
Conclusion
In this study of musculoskeletal outpatients, general interpersonal trust was not associated with trust in the treating clinician, suggesting that trust in clinicians is context-specific rather than a fixed personal disposition. Notably, patients with less healthy mindsets, social health and lower global trust still reported high levels of clinician-specific trust, emphasizing that therapeutic trust can be cultivated through effective interpersonal engagement regardless of a patient’s psychosocial background. These findings highlight the importance of addressing modifiable factors, particularly by enhancing patients’ sense of personal health agency, as a priority strategy to strengthen patient-clinician trust and improve overall experience in musculoskeletal care.
Footnotes
Acknowledgments
The authors gratefully acknowledge Nicole Esonwune for her valuable contributions to the conception and design of this study.
Ethical Considerations
Ethical approval for this study was obtained from the University of Texas at Austin Institutional Review Board (approval number: STUDY00004831). Verbal informed consent was obtained from participants.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
De-identified data may be made available on reasonable request to the corresponding author.