
Abstract
In a prior study, communication scholar ratings of clinician communication effectiveness did not correlate with perceived clinician empathy, which is one aspect of patient experience. We repeated the analysis with a different rating of communication effectiveness to increase confidence that the lack of association was not due to an inadequate rating tool. Video-recorded visits (108) were rated by 3 trained observers using the Communication Quality Analysis with acceptable reliability. Patients completed measures of perceived clinician empathy, pain accommodation, health anxiety, and depression symptoms. Negative binomial regression analysis sought factors associated with perceived clinician empathy. Only accommodation of pain met the criterion for entry into a multivariable model for perceived clinician empathy (ρ = 0.17; P = .08). No factors were associated with perceived clinician empathy, including independently rated communication effectiveness. The consistent finding of no correlation between communication effectiveness and patient perception clinician empathy using a second rating tool does not diminish the importance of effective patient–clinician communication, but it does reinforce the need to identify suitable measures of modifiable factors associated with poor patient experience.
Introduction
Background
Interpersonal skills and the ability to establish a genuine, trusting relationship with a patient are important nontechnical skills for clinicians. 1 There is evidence that higher patient ratings of their experience of care are associated with the quality rather than the duration of the visit. 2 Patient experience can be measured as perceived empathy, communication effectiveness, willingness to recommend, trust, and other factors.3,4 Communication competency can be enhanced by increasing the clinician's awareness of their opportunities for improved listening, respect, compassion, and guiding. 5
Musculoskeletal specialty care is a productive setting for studying communication effectiveness and patient experience of perceived empathy. In part because visits, tests, and treatments for musculoskeletal illness are largely discretionary. In addition, levels of musculoskeletal discomfort and incapability are notably related to mindsets and circumstances. Finally, previous studies found that orthopedic surgeons have lower ratings of communication effectiveness in comparison to other surgical and nonsurgical subspecialties. 6
Rationale
In a study of video-recorded musculoskeletal specialty care visits, communication scholars rated clinician communication strategies using the Liverpool Communication Skills Assessment Scale (LCAS) and found little to no association between those ratings and patient-rating of their clinician's empathy. 7 The LCAS is designed for evaluation of medical students in objective structured clinical examinations with actor patients. It measures five domains of communication including nonverbal behavior, respect and empathy, questioning, and giving information. 8 The findings that the Liverpool scale doesn’t correlate with patient-rated clinician empathy may indicate that more effective communication alone is not sufficient for patients to experience empathy, or it may be that the Liverpool assessment of communication effectiveness is inadequate for capturing factors associated with patient experience measured as perceived empathy. 7 One drawback of the LCAS is that it has substantial ceiling effects.1,7
The Communication Quality Analysis (CQA) utilizes real-time coding, assesses a broader range of communication aspects, including verbal and nonverbal aspects by incorporating Multiple Goals Theory, and does not exhibit ceiling effects.7,9,10 To improve patient experience, it would be helpful to identify aspects of communication that can be objectively measured, fed back to clinicians, coached for improved skills, and reassessed. 11 In secondary use of the videos of people receiving musculoskeletal specialty care, we applied the CQA and asked: Are there any factors associated with patient perception of clinician empathy, including the CQA rating, accounting for other factors?
Method
Study Design
In a prior cross-sectional study, adult (age 18 or greater), 120 new and return patients seeing a musculoskeletal specialist and fluent in English consented to have their visit video-recorded and to complete a set of questionnaires on a tablet after the visit. 2 Patients with cognitive deficiency or illiteracy were excluded.
Study Population
From the prior cohort, 12 were missing key elements of the visit needed for the CQA rating. This left 108 patients with videos that included all elements needed for rating in the video along with a complete set of associated data. The cohort was 56% men (60 of 108) with a mean age of 45 ± 15 years (Table 1).
Demographics and Ratings of the 108 Participants.
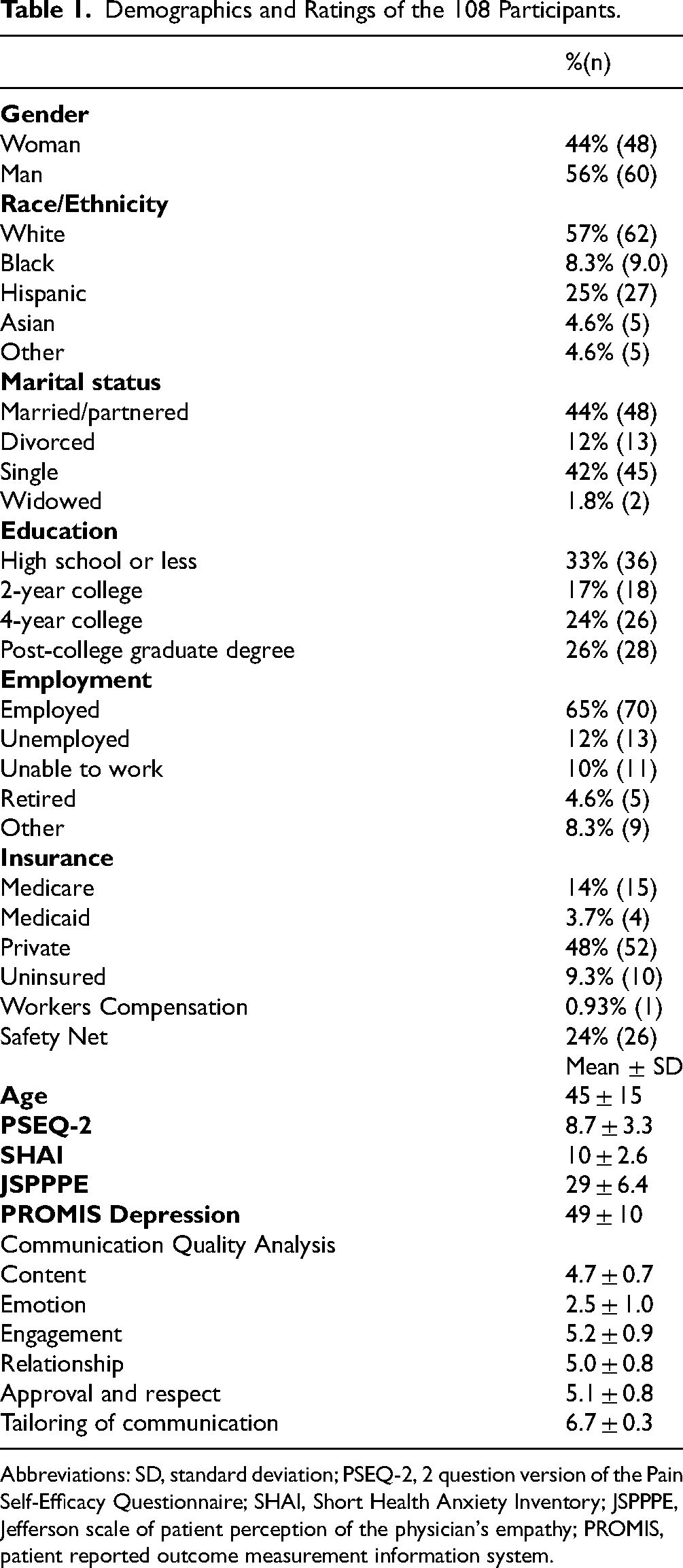
Abbreviations: SD, standard deviation; PSEQ-2, 2 question version of the Pain Self-Efficacy Questionnaire; SHAI, Short Health Anxiety Inventory; JSPPPE, Jefferson scale of patient perception of the physician's empathy; PROMIS, patient reported outcome measurement information system.
Outcome Measures
The outcome measure was the level of perceived clinician empathy as measured using the Jefferson Scale of Patient Perceptions of Physician Empathy measure (JSPPPE).
Other Variables
Personal data including self-described race/ethnicity, marital status, education status, employment status, income, insurance status, and comorbidities. Participants completed the Pain Self-Efficacy Questionnaire 2 (PSEQ-2), the Short Health Anxiety Inventory (SHAI), and the Patient-Reported Outcomes Measurement Information System (PROMIS) Depression Questionnaire.
Three independent, trained raters (two communication scholars and one trained medical student) independently scored communication effectiveness using real-time CQA. Raters trained by watching six training modules that discuss the categories being assessed using CQA, Multiple Goals Theory, and how to code the visit. Raters assigned a score from 1 (not at all) to 7 (to a great degree) for six domains (content, engagement, emotion, relationship, face [approval and respect], and accommodation [tailoring of communication strategies to the individual]) of communication for every 5-min video segment. The 3 raters then each scored the same 10 videos, tested reliability, reviewed codes together, and resolved any discrepancies through discussion and mutual consensus. Three rounds of practice visits were scored, reviewed, and discussed. The agreement of the 3 raters was within an acceptable range of interclass correlation coefficient 0.58 (95% Confidence interval 0.53 to 0.64).
Statistical Analysis
Descriptive statistics were performed for all demographics of the included patients. Continuous demographic data was reported as mean with the standard deviation, and categorical demographic data was reported as percentages with numerical values.
The distribution of patient-perceived clinician empathy was non-Gaussian according to a Shapiro-Wilk test. We sought correlations of explanatory variables with perceived empathy using Spearman rank correlation for continuous variables, Mann-Whitney test for dichotomous variables, and Kruskal Wallis for categorical variables (Appendix 1). In the bivariate analysis, the association with perceived physician empathy is reported Spearman rank correlation for continuous variables, and median with interquartile range for categorical variables. Variables with association with P < .10 in bivariate analysis were moved to negative binomial regression analysis to account for confounding. All P values below .05 in the multivariable analysis were considered statistically significant.
Results
Factors Associated with Patient Perception of the Clinician's Empathy
Only pain self-efficacy (PSEQ-2) met the criterion for entry into the multivariable model for perceived clinician empathy (rho = 0.17; P = .08; Appendix 1). In negative binomial regression analysis, there were no factors associated with patient perception of clinician empathy, including the CQA rating. Observer ratings of the clinician were highest regarding their ability to tailor communication and lowest in expressing emotion and providing emotional support (Table 1).
Discussion
Effective communication is an important nontechnical skill for clinicians. Finding effective methods to assess and quantify the effectiveness of clinician communication strategies could be a useful part of interventions to improve the patient and clinician experience of care. Patient experience can be measured as perceived empathy, communication effectiveness, willingness to recommend, trust, and other factors, all of which are notably correlated to one another and seem represent a single factor that might be considered “relationship” or “trust.”2,3,12-14 Prior studies have assessed the association of patient social and cultural factors in perceptions of clinician empathy, but many of these factors including race, education, and income, and other personal factors such as thoughts and feelings regarding sensations, have limited or mixed association with measures of experience such as empathy.3,14-17 A prior study using a measure intended for Objective Structured Clinical Examinations of medical students shows little or no correlation with patient ratings of the clinician's empathy. 7 To address the possibility that the lack of association was due to using a less suitable measure of communication effectiveness, we rated the videos again using a measure intended to quantify clinician communication effectiveness and found no correlation with patient perceptions of clinician empathy. This increases our confidence that the lack of association between the clinician's communication strategies and the patient's experience is reproducible and accurate. This finding does not diminish the importance of effective, empathic patient–clinician communication, but it does reinforce the need for additional study to identify suitable measures of modifiable factors associated with patient experience.
This study has several limitations, including most of the limitations of the original study such as the inability to blind video raters regarding the clinician (although 2 raters did not know any of the clinicians), the high ceiling effect of the empathy measure, and no record was kept of the few patients who declined participation. A limitation of the current study is that the CQA is a relatively new rating with limited testing. Regarding the choice of empathy/experience measures, the JSPPPE has lower ceiling effects than other experience measures such as the CARE measure. 18 The CQA addresses many aspects of patient-clinician interaction, including emotion and both verbal and nonverbal aspects of communication. It was developed as a goal-oriented communication analysis instrument, which is what we desired for ratings of patient-clinician interaction. The alternative was to develop our own rating. We preferred the CQA instrument which was aligned with our needs, carefully developed, and used in prior studies. Finally, the CQA has the factors that we felt it was important to address, but there may be other important factors besides empathy associated with patient experience. But it's not clear what other factors exist and if they can be measured. In addition, while a Kappa value of 0.58 is generally considered moderate—and adequate—agreement, there are variations in how Kappas are interpreted and this level of reliability could have influenced the findings. In our opinion, an important relationship should be detectable even with this amount of variation between raters. One of the raters knew some of the clinicians, but based on the reliability ratings, this did not have much influence on the ratings. This study was also conducted in a single, specialized musculoskeletal practice with a sample size of 108 which can limit the generalizability of our findings. Our feeling is that there was sufficient diversity in clinician communication style and patient backgrounds and mindsets that the lack of association is likely representative of other settings, but it merits investigation. Some clinical practices may not routinely collect measures of pain intensity, as they can influence opioid prescribing, which could also affect patient perception of clinician empathy, and thus our findings may not be applicable in these patient populations. We have an effective opioid strategy and rarely prescribe them except for several days after surgery, so this is unlikely to have affected our findings. Furthermore, we believe these findings are likely to hold across various pathophysiologies to the degree that they represent aspects of human illness and communication behavior. One might wonder if the observed lack of association between the CQA and JSPPPE was due to floor effects (a high percentage of very low ratings of empathy) given the track record of orthopedic surgeons, but there was a Gaussian distribution with somewhat of a ceiling effect (Table 1). 6 It has also been well documented that patients want to feel heard and understood from all clinicians. Therefore, it's reasonable to conclude that patients expect empathy from their orthopedic surgeon. This would also support that the floor effects of our communication and empathy measures would not explain our lack of observed association. Finally, we have strategic opioid policies and disputes over medication are not part of our daily practice. Changes in practice including no longer collecting ratings of pain intensity are relatively unlikely to influence the results of this study.
The finding that communication scholar ratings of clinician communication strategies are not associated with the patient-perceived physician empathy is confirmatory and underlines the need for additional study to identify modifiable factors associated with patient experience. There is limited and inconsistent evidence suggesting that patient experience measured as satisfaction, met expectations, perceived empathy, communication effectiveness, trust, and involvement in decisions may have small correlations with mindset factors such as levels of despair and unhelpful thinking.4,9,11,19,20 Given the association of levels of discomfort and incapability with both experience and mindsets,15,17 one might expect a stronger association between experience and mindsets. Although experience measures tend to correlate with one another, there is a limited correlation with mindset factors in many studies.12,13,21 It seems that effective clinician communication strategies are important, but not sufficient for patient ratings of perceived empathy, a key aspect of a good patient experience. It's possible that an experience measure with a more Gaussian distribution and less ceiling effect is needed and there is some work in that direction.22-24 It could also mean that there are untested patient factors, such as personality disorders, that may play a role in the patient experience, but more work is needed in this area.
Conclusion
Using an existing dataset, we found that a different measure of clinician communication effectiveness did not associate with levels of perceived clinician empathy. The consistent findings confirm a limited correlation between independent measures of clinician performance and perceived clinician empathy. It's useful to know that effective communication strategies are not sufficient for good patient ratings of their experience such as ratings of the clinician's empathy. Possibilities meriting investigation include the prospect that specific medical interactions are inherently unsatisfying, perhaps because the diagnosis and treatment options leave a lot to be desired, and some people express their frustration with this in terms of low patient experience (perceived empathy, trust, effective communication, willingness to recommend, etc). Other areas that merit investigation are nonlinear relationships between measures of experience and measures of clinician behavior (investigated perhaps with cluster analysis and other statistical techniques), the use of experience measures based on natural language processing, controlling for social desirability bias, and other possibilities.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735251323674 - Supplemental material for Does Communication Effectiveness Assessed by Communication Scholars Correlate with Patient Perception of Clinician Empathy?
Supplemental material, sj-docx-1-jpx-10.1177_23743735251323674 for Does Communication Effectiveness Assessed by Communication Scholars Correlate with Patient Perception of Clinician Empathy? by Haley Ponce, Rafael Cordero, Jacinta Tran, Natalie Wellman and David Ring in Journal of Patient Experience
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.