
Abstract
Missed appointments (no-shows) in primary care compromise timely access to care and contribute to higher healthcare costs. The expansion of patient portals, mandated by the 21st Century Cures Act, and the broader adoption of digital tools may transform how patients engage with their healthcare providers. We conducted a case-control study using electronic medical records from an academic family medicine clinic between April and May 2023. Eligible participants were patients 18 years and older. Cases were the no-shows. Two controls, patients who attended their appointments, were randomly selected for each case. Logistic regression was used to examine the association between patient portal access and no-shows, adjusting for sociodemographic and clinical covariates. Patients who missed appointments were less likely to have access to the patient portal (odds ratio: 0.43; 95% confidence interval: 0.30–0.59). Factors positively associated with no-shows included being non-Hispanic Black, Hispanic, and having public insurance or no insurance. Hypertension and osteoarthritis were negatively associated with no-shows. Access to patient portals was associated with lower odds of missed appointments, suggesting that digital engagement tools may improve adherence to primary care visits.
Introduction
Missed medical appointments present a substantial challenge to healthcare systems. In the context of primary care, such missed visits may compromise timely access to both primary and secondary preventive services, leading to poorer health outcomes, increased utilization of emergency services, and overall higher healthcare costs. 1
In primary care, approximately 15% of scheduled appointments result in no-shows, with reported rates ranging from 3% to as high as 48% causing a substantial economic impact to health systems and patients. 2 Missed medical appointments are estimated to cost the U.S. healthcare system approximately $150 billion annually. 3 In 1 single-center study, annual revenue losses exceeded $170,000, with each missed appointment costing nearly $300. 4
Previous research has identified numerous factors associated with patient no-shows across various clinical settings. Some of these factors include male sex, young adult age, non-White race, mental health comorbidities, and financial payer.5–9 A systematic review by Sun et al 10 examined the characteristics of diabetic patients who missed appointments, focusing on sociodemographic factors such as age, sex, race, ethnicity, education, and insurance status. The review found no significant association between sociodemographic factors and missed visits; however, limited access to transportation was significantly associated with higher no-show rates. 10
Patient portals are secure websites or mobile apps securely integrated into electronic health records that allow patients to view medical notes and test results, visit summaries, manage appointment schedules, receive appointment reminders, and update personal contact information. 11 These features are nearly universal to physician practices that utilize an electronic health record to provide timely and transparent healthcare. Since the full electronic health information access provisions of the 21st Century Cures Act took effect on October 6, 2022, patients have gained broader digital access to their medical records, potentially transforming how they engage with healthcare providers. 12 However, the impact of patient portals on no-show rates in primary care has not been fully examined since the implementation of the Cures Act. Prior to the Cures Act, 1 retrospective study in a family medicine office examined 46,544 patients between 2013 and 2016 and found that quarterly no-show rates were significantly lower among patients with portal access in 8 out of the 11 quarters. In the remaining 3 quarters, there was no significant difference between portal users and nonusers. 13 Additional studies have found a positive impact of patient portal use on appointment adherence.14,15 While previous studies have examined the impact of patient portals on no-show rates, more up-to-date assessments are needed in primary care, especially since the implementation of the Cures Act and the widespread adoption of mobile apps, which may be reshaping how patients engage with their healthcare providers. Additionally, physician burnout, a prominent wellness concern, is influenced by both patient and physician satisfaction and is exacerbated by schedule uncertainty and pressure to meet performance goals. 16
This study aims to evaluate the association between patient portal access and no-show rates in a primary care setting within a large urban academic medical center. We hypothesize that access to the patient portal is associated with a decreased rate of no-shows as it may enhance communication, appointment reminders, and overall engagement with care.
Methods
Study Design
We conducted a case-control study using electronic medical records (EMRs) from an academic family medicine clinic in a major urban center between April and May 2023. Eligible participants were patients aged 18 years and older. Cases were patients who missed their scheduled appointments (no-shows). For each case, 2 patients who attended their appointments on the same day as the cases were scheduled were randomly selected as controls. In the event that a case had missed more than 1 scheduled appointment in the study period, the patient was counted on the first missed appointment. We reviewed the EMR of participants to determine who had registered for portal access, our exposure variable. Patients were then categorized as exposed (those with access) or unexposed (those without access). We also collected information on potential confounders, namely, demography (age, race/ethnicity, and sex), time of appointment, proximity from the clinic, insurance, provider type, chronic morbidities (hypertension, diabetes, and osteoarthritis), and whether the patient was new to the clinic or an established patient.
Patient age was defined as the number of completed years as recorded in the patient records on the date of the scheduled visit included in this study. Race/ethnicity and sex information were extracted as stated in the EMR. We used the time of the scheduled appointment to create 3-time categories: 7:30 am to 8 am (extended hours to accommodate patients), 8 am to 12 noon, and after 12 noon to 5 pm (traditional hours). Patients’ residential addresses were used to estimate travel distance to the clinic via Google Maps, as distance has been shown to influence appointment adherence.17,18 Outliers were identified using normal distribution curves, and patients residing more than 45 miles from the clinic were excluded from the study. The proximity to the clinic was categorized into 4 groups: 0–5, 6–10, 11–14, and 15 or more miles. Patient insurance status was categorized as “Private,” “Public” (Medicare or Medicaid), or “None.” Provider type referred to the healthcare provider whom the patient had been scheduled to see: faculty (board-certified family physician), trainee (family medicine resident or fellow), or nurse, as there is a known higher no-show rate for medical trainees compared to faculty. 19
The distribution of the independent or exposure variable, and the covariates among the cases and controls were compared using a t-test for continuous variables and chi-square or Fisher's exact test for categorical variables, as appropriate. Bivariate logistic regression analysis was performed to establish associations between no-shows and access to patient portals, as well as the covariates. We then assessed independent associations between access to patient portals and no-shows in a multivariable logistic regression model, adjusting for covariates that were statistically significant at the bivariate level.
A post-hoc power analysis was performed. Associations were reported as odds ratios (ORs) with corresponding 95% confidence intervals (CIs). Statistical significance was defined as p < 0.05. We used STATA19.5 (StataCorp LLC, College Station, TX, USA) for the analysis.
This study was approved by our Institutional Review Board and did not meet the informed consent requirement.
Results
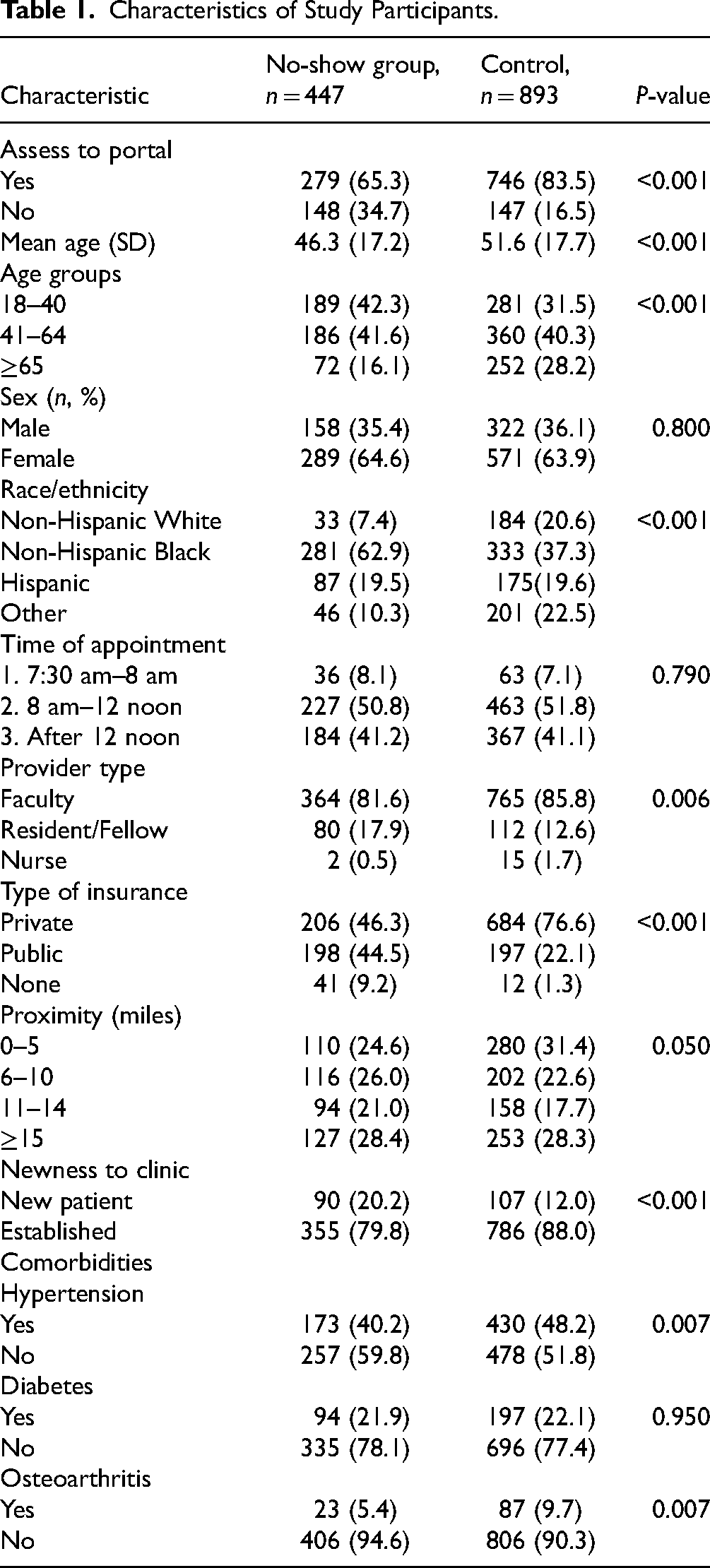
The total number of 1340 patient records was analyzed, including 447 no-show cases and 893 controls. Sixty-five percent (279) of the cases and 83.5% (746) of the controls had access to the patient portal, p < 0.001. Table 1 is a detailed description of the distribution of cases and controls by the independent variable and relevant covariates. In addition, cases were significantly less likely to be younger and more likely to be non-Hispanic Black. They were also more likely to have public insurance and were less likely to have a clinic appointment with a faculty member (as compared to a trainee physician or a nurse).
Characteristics of Study Participants.
On bivariate analysis, missed appointment (no-shows) was significantly associated with access to the patient portal (OR = 0.37, 95% CI = 0.28–0.48). Older age (OR = 0.98, 95% CI = 0.98–0.99) was significantly associated with missed appointments. Other covariates significantly associated with missed appointments were race/ethnicity, provider type, type of insurance, proximity to the clinic, and whether the patient was a new or an established patient to the clinic. In addition, the presence of chronic comorbidities, hypertension, and osteoarthritis was associated with missed appointments. Table 2 provides a detailed summary of the bivariate associations between cases and the covariates.
Association With “No-Show” on Bivariate Analysis.
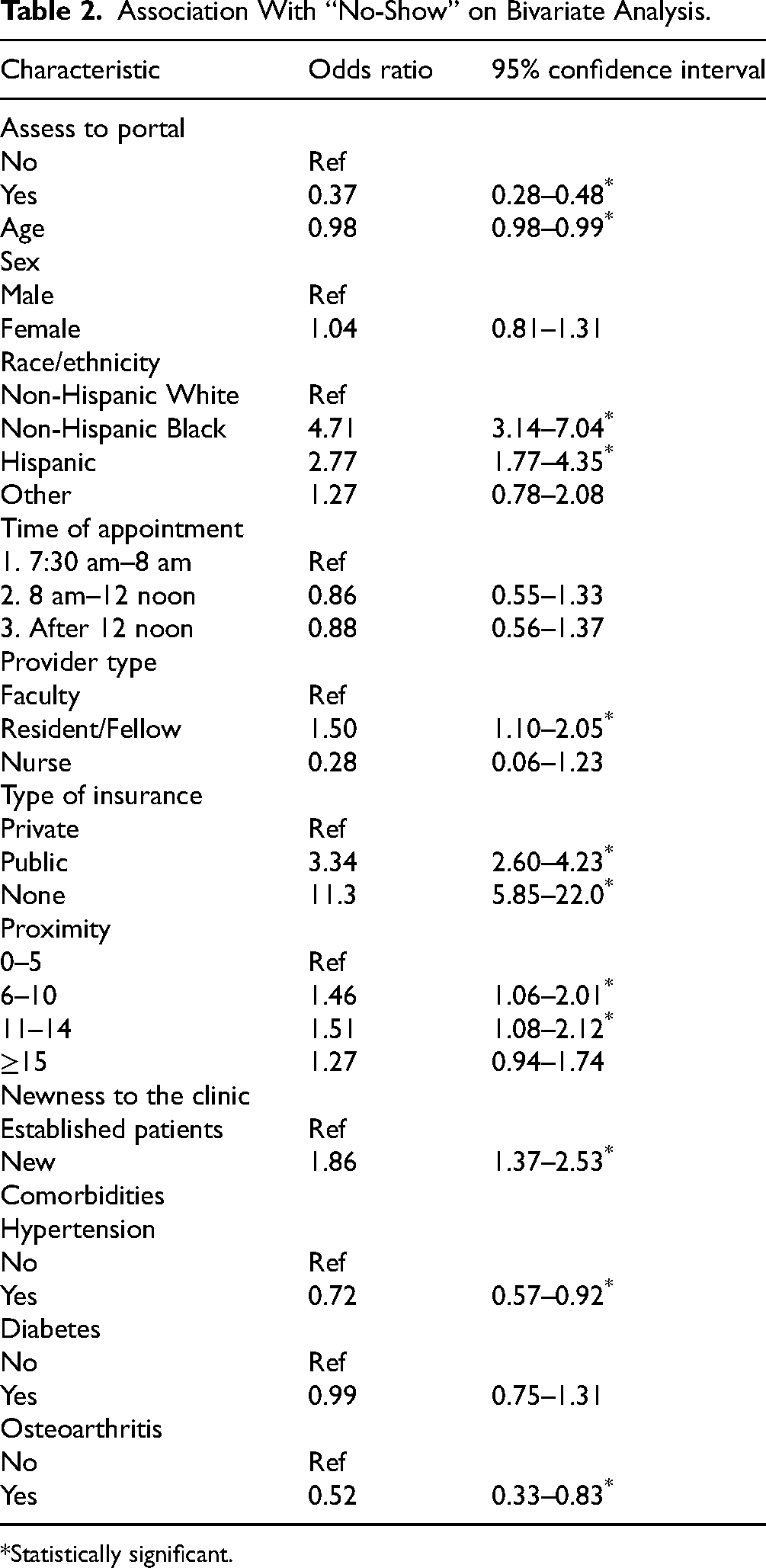
Statistically significant.
In a multivariable logistic regression analysis adjusting for covariates significant at the bivariate level, patient portal access was associated with a 57% reduction in the odds of missing an appointment, OR = 0.43, 95% CI = 0.30–0.59). Older age (OR = 0.98, 95% CI = 0.97–0.99), as well as having hypertension (OR = 0.70, 95% CI = 0.50–0.98) or osteoarthritis (OR = 0.55, 95% CI = 0.31–0.98), were associated with lower odds of missing appointments. In contrast, being non-Hispanic Black (OR = 4.32, 95% CI = 2.69–6.92) or Hispanic (OR = 2.29, 95% CI = 1.36–3.85) was associated with significantly higher odds of missed appointments compared to non-Hispanic White patients. Compared to those with private health insurance, patients with public insurance (OR = 3.31, 95% CI = 2.47–2.43) and those without insurance (OR = 7.05, 95% CI = 3.40–14.6) were also more likely to miss appointments. Table 3 shows the association between access to patient portals and no-shows after adjusting for relevant covariates.
Factors Associated With “No-Show” in Multivariable Model.
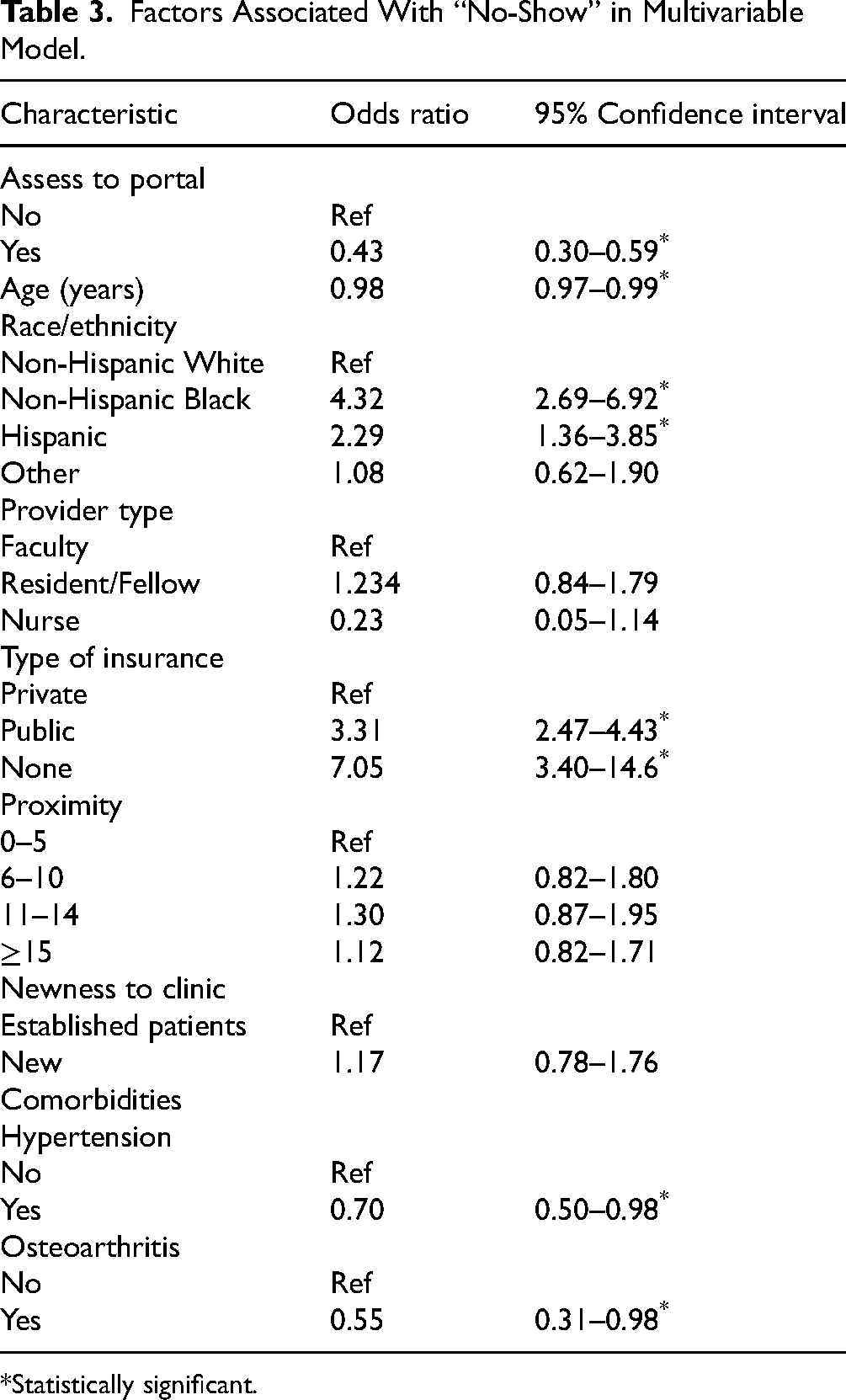
Statistically significant.
Post-hoc Power Analysis
Using number of cases as 400 and a 1:2 matching, with a level of significance of 0.05 and the observed probability of exposure among our controls of 0.85, the estimated power to observe an OR of 0.43 was 99%.
Discussion
In this study, we examined the association between patient portal access and missed clinic appointments at a large urban academic family medicine practice during April and May 2023, adjusting for known confounding variables. We found that patients with access to the portal were 57% less likely to miss appointments compared to those without access. We also found that older adults, patients with hypertension, and patients with osteoarthritis were less likely to miss appointments. In contrast, compared to non-Hispanic White patients, non-Hispanic Black and Hispanic patients were more likely to miss appointments. Additionally, individuals with public insurance (such as Medicaid or Medicare) and those without insurance were more likely to miss appointments than those with private insurance. Proximity to clinic, provider type, and whether the patient was new or established were not associated with no-shows.
Our observation that access to patient portals is associated with a decreased likelihood of missed appointments aligns with previous research. For example, Zhong et al 13 reported significantly lower no-show rates among portal users compared to nonusers. Similarly, Varady et al 15 found that patients undergoing orthopedic surgery who used a patient portal had a lower no-show rate than nonusers (6.8% vs 7.2%). Horvath et al 14 also observed comparable trends in their study, reinforcing the link between access to the patient portal and decreased no-shows.
Patient portals enable patients to take a more active role in their healthcare by providing immediate access to their medical information. This direct access facilitates improved communication between patients, their caregivers, and the medical team. Through the portal, patients can ask questions, report concerns, and schedule appointments. 20 Portals can also be used to send appointment reminders to patients. This enhanced communication may partly account for the observed association between patient portal use and a lower incidence of missed appointments. Consistent with this, 1 study found higher overall patient satisfaction among those who used the portal. 15
However, while portals promote transparency and engagement, they may also generate anxiety or confusion when patients access results before physician review, potentially leading to misinterpretation.21,22 This concern is particularly relevant following implementation of the Cures Act, which mandates the immediate release of medical records to patients. 12
While patient portals can enhance communication between patients and healthcare providers, their use is influenced by personal factors such as age, ethnicity, education level, health literacy, and overall health status. 23 In a recent study, Gordon et al 24 reported that Latino and Chinese adults in Northern California with limited English proficiency used the portal less often than their counterparts without language barriers. Surveyed patients attributed this gap to lower educational levels, reduced health literacy, and limited access to digital tools. 24
Our findings corroborate previous research demonstrating that demographic and clinical characteristics, including age, race/ethnicity, insurance status, and the presence of chronic conditions, are associated with appointment adherence. Consistent with earlier studies, older age and having private insurance, compared with Medicaid or no insurance, were associated with a lower likelihood of missed appointments.2,5–7,9,13,19 Similarly, the presence of chronic conditions, particularly hypertension and osteoarthritis, was positively associated with attending scheduled visits. Several mechanisms may contribute to these patterns. Older adults may have a stronger sense of responsibility for managing their health and more frequent follow-up needs, with appointment coordination and transportation often facilitated by caregivers. The higher likelihood of missed appointments among patients with public or no insurance may reflect language barriers, financial barriers, and limited scheduling flexibility. Chronic conditions may heighten the perceived importance of timely care, reinforcing regular attendance. The influence of race and ethnicity is likely multifactorial, shaped by cultural attitudes toward healthcare, social support networks, and the local delivery context. These patterns may also reflect underlying socioeconomic differences that contribute to disparities in digital health equity.
Addressing these disparities will require tailored strategies rather than a 1-size-fits-all approach. At the institutional level, efforts can focus on improving digital access and digital health literacy. Patients can be screened for digital access at check-in, with those needing support referred to appropriate resources. In addition, digital health literacy can be enhanced by employing digital health navigators to assist patients, particularly those new to the portal, with onboarding and effective portal use. In contrast to some prior studies, we observed no association between no-shows and travel distance, provider type, or patient newness to the facility.17–19 These results suggest that patients’ adherence to clinic appointments may be influenced by a complex set of factors, and that engagement through tools such as the patient portal may play an increasingly important role, particularly in light of broader digital access following the Cures Act.
Missed appointments remain a persistent challenge in primary care, with significant cost implications. In response, institutions have implemented various strategies to improve access and mitigate losses. While overbooking is 1 approach, it often leads to unpredictable schedules and increased patient wait times when appointments are kept, diminishing satisfaction for both patients and clinicians. In contrast, expanded patient portal access is a relatively recent intervention that not only empowers patients to engage more actively in their care but also provides frequent real-time reminders and convenient options to electronically reschedule visits.
Although our findings align with earlier studies, they offer a more contemporary perspective on no-shows in relation to patient portal access.13–15 Given the rapid technological advancements of recent years, modern portals offer significantly more features than those available a decade ago, when most prior studies were conducted. Our results support continued efforts to promote portal registration, with targeted outreach to younger patients, Hispanic and non-Hispanic Black patients, and those with public insurance.
Limitations
One of the limitations of this study is that although we assessed whether patients were registered for the portal, we were unable to determine whether they actively used it. However, given that registration was optional, it is reasonable to assume that individuals who chose to register were inclined to use it. Because our exposure variable reflected access, that is, registration for the portal and not actual use, some participants classified as exposed may not have meaningfully engaged with the portal. This may create nondifferential misclassification, which would be expected to weaken the association, leading to an underestimation of the true effect of the exposure. In addition, there may be variations in the use of the portal among the exposed group. Our study could not determine whether missed appointments were intentional or unintentional because this information was not captured in our data. Future studies could reevaluate the no-show rate among individuals who have logged in to read the appointment confirmation message within the patient portal. This study also utilized data from a single center over a 2-month period. However, the no-show rates are similar month to month in this large urban academic center serving a demographically diverse population. Our sample consists primarily of urban residents, which may restrict the external validity of the results, particularly when applied to rural populations or settings with different healthcare access patterns. In addition, the pattern of missed appointments over the 2-month period used may be affected by seasonal variations, further limiting the external validity of the results. Lastly, this study did not evaluate the impact of English proficiency or digital literacy on patient portal enrollment or on appointment adherence.
Conclusion
Access to the patient portal was associated with decreased missed appointments. This study is among the first since the implementation of the Cures Act to evaluate how patient portal registration influences missed appointments. Given the Act's emphasis on providing immediate access to their health information, understanding the portal's role in promoting timely care is particularly relevant. By offering real-time appointment reminders, improving communication between patients and providers, and fostering active patient engagement, the portal has the potential to reduce missed appointments, improve healthcare delivery, and, in turn, lower healthcare costs while enhancing satisfaction for both patients and physicians.
Footnotes
Acknowledgments
Not applicable.
Author Contributions
Shira Goldstein: Conceptualization, methodology, writing of original draft, review and editing, approval of final draft. Kaylee Buuck: Data curation, methodology, review and editing of final draft. Hannah Thompson: Data curation, methodology, review and editing of final draft. Renee Yu: Data curation, methodology, review and editing of final draft. Nicole Small: Data curation, methodology, review and editing of final draft. Jude des Bordes: Conceptualization, methodology, drafting of original draft, review and editing of final draft, data analysis. Nahid Rianon: Methodology, data analysis drafting of original draft, review of final draft. All authors approved the final version of the manuscript.
Data Availability
Data for this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Committee for the Protection of Human Subjects of the University of Texas Health Science Center (UTHealth) (HSC-MS-22-1037).
Informed Consent Statement
This study was deemed ineligible for informed consent and was therefore granted exemption by our institutional review board.