
Abstract
Nonurgent emergency department (ED) visits continue to rise despite efforts to reduce ED overcrowding. This study aimed to explore factors influencing ED utilization and perceptions of alternative healthcare services among patients of nonurgent ED visits. Conducted at an academic, level-1 trauma center, the study identified nonurgent visits using the emergency severity index 5-level triage acuity scale and utilized a 3-part qualitative survey to gather data on demographics, reasons for ED visits, and perceptions of the ED, primary care physicians (PCPs), and urgent care centers (UCCs). Survey responses from 586 patients were analyzed, demonstrating common themes such as ED accessibility, physician qualifications, and the need for diagnostic testing. Although participants generally expressed satisfaction with PCPs and UCCs, the frequency of nonurgent ED visits remained high. The study suggests that many nonurgent cases could have been managed using alternative healthcare services; additionally, the findings align with existing literature and support the need for enhanced patient education on appropriate ED use and the benefits of utilizing alternative healthcare options.
Introduction
Emergency department (ED) overcrowding is a significant health crisis that is worsening over time. 1 Negative consequences include discontinuity of patient care, provider stress, dissatisfaction with patient care, and increased risk of error, wait times and cost.2-5 Many factors have been proposed as contributing to overcrowding, including ED closures, increased volumes, hospital boarding, and staffing shortages. 1 Among these, nonurgent ED use is increasingly recognized as a contributor, but is critically understudied.
As nonurgent ED visits may be a correctable cause of overcrowding, it is an area of interest for research and possible interventions. While prior efforts have focused on systemic solutions like expanding urgent care access 6 or cost-sharing, 7 a significant gap remains in understanding why patients with nonurgent conditions continue to choose the ED, especially when other care options are available. By analyzing why patients utilize the ED for nonurgent reasons despite alternatives like primary and urgent care centers (UCCs), there is an opportunity to develop more direct and sustainable solutions. This study explores patient decision-making and perceptions, insights that are essential for introducing new and efficient approaches.
In 2013, a literature review 8 on ED utilization in the United States concluded that 37% of all ED visits were attributed to nonurgent chief complaints. A suburban tertiary care center conducted a similar assessment 9 in 2013, concluding 44.6% of nearly 700,000 patient encounters were nonurgent and could have been treated with alternative healthcare services. In a more recent study, 10 59.2% of patients who qualified for primary care services were classified as emergency severity index (ESI) levels 4 and 5, suggesting more than half potentially had the option to visit their primary care providers (PCPs).
Multiple interventions such as financial disincentives, copayments for ED visits, expanding the use of premiums and cost-sharing in Medicaid, patient education on appropriate ED use, and introduction of new UCCs have been implemented by hospitals and insurance payers in attempts to decrease the number of nonurgent ED visits.7,8,11-13 However, the effects of these interventions remain controversial. A study by Allen et al 6 showed that introducing UCCs reduced ED volumes, but only among privately insured patients. Cost-sharing for medical services may create a barrier for patients with lower incomes to obtain care 7 ; and increased cost-sharing has been associated with a reduction of preventive and primary care services and decreased medication adherence, leading to increased ED use.14-16 Studies of cost-sharing for ED visits have been contradictory. A study by Sabik and Gandhi 17 analyzed data from nonelderly adult Medicaid enrollees and found that copayments may be an effective tool for reducing the use of the ED for nonurgent care. However, another study by Siddiqui et al 18 did not show a significant change in patterns of ED use with copayments for nonurgent visits.
Prior research and interventions have not adequately addressed the underlying causes for nonurgent ED visits, due to a lack of information on the factors that drive patients to use the ED. Recent literature19,20 has noted that potential reasons include patient perspectives on what constitutes an emergency and the ease of accessing advanced resources. A study by Tapia et al 20 that surveyed patients signing into the ED with ESI levels 4 and 5 found that the most common reasons were self-reported emergencies and the inability to get a timely appointment, while simultaneously noting that 4000 appointments are unfilled monthly within their healthcare system. Therefore, this perception of lack of access may reflect difficulty navigating the system rather than true lack of access. Similar studies21,22 have also noted easy accessibility, 24/7 availability of service in the ED, and perceived need as drivers for nonurgent use. Out of the patients who cited perceived need as their reason for attending the ED, many of them contacted their general practitioner (GP) before presenting to the ED and one quarter had been referred to the ED by their GP.
The patients’ perspective on why they visit the ED for nonurgent reasons (especially by patients who have a primary care doctor or have access to UCCs) remains unclear. This study therefore aims to close this gap by investigating: (1) the reasons for nonurgent visits to the ED; and (2) how patients who present to the ED for nonurgent visits perceive primary care centers and UCCs.
Methods
The descriptive-exploratory study allowed patients to share their reasons for visiting the ED for nonurgent reasons using a survey with predetermined choices. It took place in an urban tertiary care, academic center. Data collection took place daily from 8 am to 12 am from August 2022 to March 2024 using Epic, the electronic health record software used by the academic center. Patients were included if they were > 18 years old, triaged as ESI 4 or 5, read English or Spanish, and could verbally consent to complete the survey. Patients were excluded if they arrived with police or from jail, had altered mental status, or were otherwise unable to consent. The study was approved by the Institutional Review Board (IRB).
The ESI, a 5-level triage scale, was used to identify patients with nonurgent chief complaints. There is no universal definition of “nonurgent” ED visits, so in the absence of a standardized metric we chose to use ESI 4 and 5 as a practical surrogate to select patients who were unlikely to require immediate emergency care, aligning with the scope of our research. While ESI is a resource used to predict resource utilization rather than urgency, levels 4 and 5 are generally associated with presentations not requiring immediate medical interventions. Previous literature has used it as a proxy for nonurgent visits, 10 and we concluded that without a retrospective analysis of diagnoses these acuities can be used as a proxy to identify potentially nonurgent visits from both a clinical and research standpoint.
The survey was created based on a literature review in PubMed and observations from clinical practice, and reviewed by an expert panel of ED physicians. To locate relevant studies on the topic, a literature research was carried out in PubMed using the following search query: (((emergency medical services OR emergency care OR ER[ti] OR “emergency room"[tiab])) AND (health services misuse OR health services misuses OR non-urgent[tiab] OR health services abuse OR avoidable[tiab])) AND (patient perception OR patient perceptive OR perception OR perceptions OR awareness) AND (English[lang]). Fifty-seven articles of interest were found; however, no validated survey was found that would directly answer our questions of interest. Twenty-one of the 57 articles were deemed to be directly helpful in the creation of the survey. The specific steps taken to develop the survey included: Preliminary literature research which demonstrated a gap in the literature for patient reasoning for presenting to the ED for nonurgent complaints. Then, (1) description of the purpose, specific aims and objectives of the survey, based on the gaps in the literature review; (2) description of the primary qualitative outcomes we sought to evaluate; (3) search for existing surveys and questionnaires that are validated (of which there were none). Finally, given no previously validated surveys that could be used or adjusted for our study we (4) created a survey from core themes identified from a review of the literature. The themes included (1) convenience, (2) perceived need or urgency, and (3) negative perceptions of alternatives. These themes and appropriate subthemes were used to develop the survey items. Once the core themes were established, the subsequent steps included (1) determination of item format—open- versus closed-ended (Linkert and multiple choice); (2) determination of the length of the survey; (3) development of the questions; (4) determination of how the survey will be administered (self-administered vs by researcher); and (5) review and revision by qualified experts which included 2 ED physicians who reviewed the items to check for accuracy and relevance of each of the items and a physician who holds expertise in qualitative and quantitative research was also consulted to aid in the determination of statistically scoring and planning.
Statistical Analysis
The data analysis was performed via chi-square tests to analyze the 2-sided asymptotic significance of the correlation between the ED utilization pattern and various factors, including patient perception, care experience, accessibility, and accessibility of PCPs and UCCs. This study included and analyzed only P-values <.05 for linear-by-linear associations.
Results
Study participants included 602 ED patients with ESI scores of 4 and 5. Although all were deemed eligible and approached for this study, only 586 were enrolled and included in the data analysis, as the remaining survey entries were either missing information or incomplete. Table 1 shows the demographics of the study participants. Of those enrolled, the majority were younger, with 36.1% between the ages of 18 to 29 and 20.7% between the ages of 30 and 39. There were significant differences in employment status, with most patients (63.5%) being employed. A majority of patients also had insurance, with coverage through private insurance (28.6%), Medicare (34.5%), or Medicaid (23.2%).
Characteristics of Study Participants Classified as Nonurgent in the Emergency Department, Distinguished by Subgroup (Age, Gender, Marital Status, etc).

To address the first research question, we examined the reasons behind why patients chose to visit the ED despite indicating a nonurgent visit. Among the patients surveyed, 76.4% provided reasons for visiting the ED that could have been addressed through alternative healthcare services, including the first 4 rows of reasons in Table 2 and “Others.” This significant proportion indicates the notion behind patients with low-acuity visits and their decision to choose the ED for reasons beyond clinical urgency. Among this population, 68.3% were currently established with their PCPs, while 31.7% recalled having previously seen a PCP. This suggests that despite existing PCP relationships, patients may still opt for the ED, raising questions about perceived accessibility and availability of primary care services.
Comparison of Reasons Behind ED Utilization Among Patients Currently Established With a PCP or Previous PCP Experience.

Abbreviations: ED, emergency department; PCP, primary care provider; UCC, urgent care center.
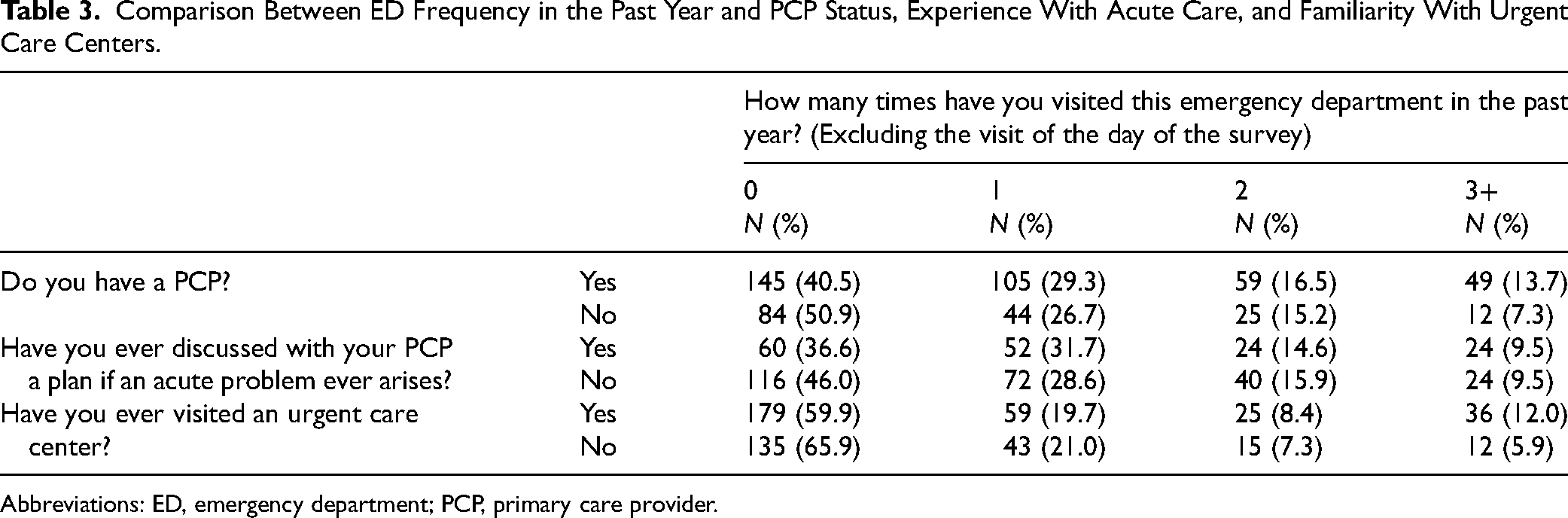
In addressing the second research question regarding patients’ perceptions of primary and UCCs, we compared ED utilization frequency to engagement with these resources. Table 3 describes the number of ED visits in the past year compared to accessibility to primary and UCCs. First-time ED visits were significantly higher among patients without a current PCP (50.9%) and those who had not previously visited a UCC (65.9%). However, higher visit frequencies were more common among patients with a current PCP and those who previously utilized UCCs. The prevalence of ED visits was most notable among first-time visitors who had never discussed an acute issue with their PCP. This implies that limited or inconsistent communication with PCPs may ultimately influence the decision to seek care in the ED.
Comparison Between ED Frequency in the Past Year and PCP Status, Experience With Acute Care, and Familiarity With Urgent Care Centers.
Abbreviations: ED, emergency department; PCP, primary care provider.
The utilization frequency of the ED was also focused based on whether or not patients had previously visited a UCC (Table 3). First-time ED visits were more common among patients who had not previously visited an UCC (65.9%) than those who had (59.9%). Patients who reported 2 or more ED visits were higher among patients who had previously utilized UCCs, at 8.4% and 12.0%, respectively. Similar to perceptions on PCPs, patients with more complex and intricate needs may be aware of alternatives like UCCs but still find the ED to be more accessible and reliable.
Table 4 represents survey responses of patients with previous UCC experience. Overall satisfaction with services provided (74.9%) is high, with the majority spending < 2 h (78.2%) at UCCs. More than half reported evening and weekend UCC availability (57.4%) and expressed that they would utilize UCCs again (69.3%). Despite generally positive perceptions, the high frequency of ED use among these patients further suggests that barriers other than satisfaction like convenience and perceived urgency may influence patient decision-making.
Patient Care Experience and Availability of Urgent Care Centers.

Discussion
Our findings demonstrate several factors contributing to the high number of nonurgent ED visits. The most frequently reported reasons include perceived ED accessibility, the belief that emergency physicians are better qualified, and the need for diagnostic testing. These align with prior research,8,23-25 reinforcing that patients often prefer EDs for comprehensive services, ones similar to those offered at alternative care options. This highlights the need for enhanced patient education on what PCPs and UCCs offer while emphasizing the importance of reserving ED resources for immediate care. However, reducing low-acuity visits alone will not resolve ED overcrowding as it is also driven by inpatient boarding and high-acuity patients. 26 Nonetheless, redirecting nonurgent patients and improving resource education can help reduce high ED volumes and should be attributed as one component of a broader strategy.
Over half of participants reported having Medicare or Medicaid as their primary health insurance, reflecting similar trends in California.27,28 These patients may be unaware of comparable resources located elsewhere at significantly lower costs. 29 Beyond affecting ED operational flow3,30 this trend also emphasizes the continued need for patient education on healthcare resource allocation as a result of perceptions on PCPs including limited availability. Patients most prevalently cited PCP or UCC referrals, recent ED complications, or limited PCP availability as reasons for visiting the ED, many of which categorized as nonurgent, despite our findings revealing access to PCPs with barriers like limited clinic hours or inability to make a prompt appointment.8,31 The contrast suggests that access to PCPs alone fails to recognize timeliness, convenience and perceived availability, all of which influence whether patients choose to utilize their PCPs. In addition to pointing towards more interventions to enhance PCP relationships, these findings pose a need for more effective access through implementations such as telemedicine visitations or postclinic care.
UCCs, with extended hours, help reduce strain on EDs by optimizing patient flow and managing nonurgent cases. 6 Although slightly fewer patients in our study had UCC experience, brief interventions like education on available services may increase their utilization. For most UCC users, patients reported high satisfaction, shorter wait times, evening/weekend availability, and were typically found to spend under 2 h at UCCs, less than California's median ED wait time. 28 Despite these benefits, higher ED use was found among previous UCC users, showing a positive correlation between use of both services when patients are familiar with UCCs. While UCCs hold great promise as a key strategy to mitigate the rising rates of nonurgent ED visits, it is essential to shift our focus toward improving patient education. Simplifying medical information about alternative healthcare options, combined with follow-up interventions via phone and mail, has shown relative success in enhancing patient education. 32 However, other studies also suggest that increasing the time availability and expanding the hours of walk-in clinics and UCCs could be another factor in reducing ED utilization. 28 Although most UCC users reported benefits like evening and weekend access, UCC operating hours vary and expanding them should still be considered to reduce overutilization of the ED for nonurgent cases.
About 12.7% of participants selected “Other” as the reason for visiting the ED, suggesting reasons beyond the scope of our research. Previous research that conducted structured interviews on this topic found 3 main themes: lack of PCPs, financial difficulties, and lack of comprehensive care outside of the ED. 21 Interestingly, most respondents reported having a PCP and insurance, 20 indicating that perceived access issues may drive ED visits rather than actual provider availability and may encompass those selecting “Other.”
Limitations
Our study has several limitations which could impact the results. For one, convenience sampling limited the ability to evaluate overnight patients. We used a structured survey to collect data, limiting the potential for patients to give extended answers. This is especially apparent, with 12.7% of patients stating their reason for their ED visit was “other.” We specified the nonurgent cohort using acuity scores of 4 and 5, but as stated above, it is unclear if this triage score is an ideal surrogate marker for “nonurgent”’ visits. Despite these limitations, the findings of this study have important policy and practice implications that support previous research and identify potential future research or educational interventions.
Conclusion
This study aimed to identify reasons for nonurgent ED visits and assess how patients who present to the ED for nonurgent visits perceive primary care centers and UCCs. Contrary to popular presumption, many patients who present to the ED for nonurgent complaints do have access to their PCP and UCCs but identify other reasons for coming to the ED like accessibility, the belief that emergency physicians are better qualified to handle their medical concerns, and the need for further diagnostic testing. These results suggest that interventions to decrease nonurgent ED visits will need to be multifactorial likely with education toward patients about the comprehensive care available at PCPs and UCCs, such as same-day or next-day appointments and phlebotomy and radiology services and possibly the addition of incentives for using primary care.
Footnotes
Acknowledgments
Not applicable.
Declaration of Conflicting Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and publication of this article.
Ethical Approval
This study was approved by the University of California, Irvine's Institutional Review Board (ID: 20195532).
Data Availability Statement
The datasets used and analyzed during the current study are not publicly available to protect participant anonymity and privacy.
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with UC Irvine's Institutional Review Board approved protocols (ID: 20195532).
Statement of Informed Consent
Verbal informed consent was obtained from the patients for their anonymized responses to be published in this article.