
Abstract
Background
The demand for complementary and integrative health (CIH) is increasing by patients who want to receive more CIH referrals, in-clinic services, and overall care delivery. To promote CIH within the context of primary care, it is critical that providers have sufficient knowledge of CIH, access to CIH-trained providers for referral purposes, and are comfortable either providing services or co-managing patients who favor a CIH approach to their healthcare.
Objective
The main objective was to gather primary care providers’ perspectives across the northwestern region of the United States on their CIH familiarity and knowledge, clinic barriers and opportunities, and education and training needs.
Methods
We conducted an online, quantitative survey through an email invitation to all primary care providers (n = 483) at 11 primary care organizations from the WWAMI (Washington, Wyoming, Alaska, Montana and Idaho) region Practice and Research Network (WPRN). The survey questions covered talking about CIH with patients, co-managing care with CIH providers, familiarity with and training in CIH modalities, clinic barriers to CIH integration, and interest in learning more about CIH modalities.
Results
218 primary care providers completed the survey (45% response rate). Familiarity with individual CIH methods ranged from 73% (chiropracty) to 8% (curanderismo). Most respondents discussed CIH with their patients (88%), and many thought that their patients could benefit from CIH (41%). The majority (89%) were willing to co-manage a patient with a CIH provider. Approximately one-third of respondents had some expertise in at least one CIH modality. Over 78% were interested in learning more about the safety and efficacy of at least one CIH modality.
Conclusion
Primary care providers in the Northwestern United States are generally familiar with CIH modalities, are interested in referring and co-managing care with CIH providers, and would like to have more learning opportunities to increase knowledge of CIH.
Introduction
The basic tenets of Integrative Medicine are that it is patient-centered with a focus on whole person health, involving collaboration between practitioners and patients to achieve optimal health and healing.1,2 There is a transdisciplinary focus to integrative health care that is typically aimed at the coordination or integration of complementary (‘alternative’ or not mainstream) and conventional (mainstream) health care approaches, also referred to as complementary and integrative health (CIH). 3 In primary care in the United States, there have been multiple efforts to increase CIH, evident in the proliferation of integrative health centers, as well as a substantial increase in opportunities for health care students and providers to learn about CIH. For example, most institutions now offer elective courses on CIH for students in nursing and medical school, and longer-term fellowships in integrative medicine are available health care providers.1,4 These efforts reflect the high consumer use of complementary health approaches. 5 In addition, these efforts reflect the need to address provider knowledge and training on complementary approaches, as it is clear from prior research that patients are seeking providers who inquire about use of CIH, have an orientation toward whole person care, have knowledge of complementary approaches and related referrals, and will collaborate with a complementary health practitioner.6,7 When asked specifically about integration of CIH integration into medical care, patients indicate that they would like to receive CIH in the primary care setting. 6 Last, these shifts in may reflect a growing interest in CIH among clinicians themselves, particularly among those who have some training or knowledge of complementary health approaches. 8
However, there are multiple potential barriers to CIH in primary care. These include patient perception that providers are not interested in CIH which can lead to non-disclosure of CIH practices by patients and can impact provider care decisions. 9 In addition, many providers remain wary of CIH, in part due to personal lack of knowledge and training on the benefits and risks of CIH approaches. 10 However, CIH offers evidence-based options for addressing common medical conditions relevant to primary care such as insomnia and anxiety, 11 chronic pain, 12 and behavioral health strategies important to a multitude of physical and mental health conditions. 13
Primary care, where 55% of all medical visits in the U.S. occur, offers an important opportunity for delivery of CIH services and patient education. 14 Thus the integration of CIH in primary care – whether that involves a team-based care approach within a clinic, CIH offerings by a dually-trained primary care provider, or referral to a CIH provider in the community – can increase patients’ access to these important services and potentially improve health outcomes. 15
To promote CIH within the context of primary care in the United States, it is critical that providers have sufficient knowledge of complementary therapies, access to CIH providers (whether in local community or within the clinic), are comfortable co-managing patient care with a CIH provider, and feel supported to move forward in this aspect of care delivery. 16 This study was designed to explore current aspects of CIH among primary care providers in a northwestern region of the U.S. where there is significant regional diversity in order to guide future next steps in these realms of education, co-management among CIH colleagues, and CIH integration into care. The study specific aims were to examine primary care provider: 1) familiarity with and perceived benefits of CIH; 2) experience referring patients for or offering CIH services within the context of primary care, 3) perceived barriers to and provider-reported availability of CIH in the clinic, and 4) interest in increasing CIH knowledge and community access.
Methods
Design
This study involved a cross-sectional one-group study design. The UW Osher Center for Integrative Medicine partnered with the WWAMI (Washington, Wyoming, Alaska, Montana and Idaho) region Practice and Research Network (WPRN) Coordinating Center, based at the University of Washington (UW) Institute of Translational Health Sciences (ITHS) and a small group of research champions from WPRN clinical sites to develop and conduct this study of primary care providers’ perspectives on CIH. The study protocol was reviewed and approved by the institutional review board at the UW and a waiver of written consent was obtained in order to preserve anonymity of survey responses.
Setting
The study was conducted in the WPRN, a collaborative group of over 80 primary care practices across 33 healthcare organizations in the Washington, Wyoming, Alaska, Montana and Idaho region. All WPRN member organizations (n = 33) were invited to participate in the study. Consistent with standard practices in the WPRN, staff and faculty held webinars with WPRN clinic representatives to orient them to the study protocol and secure leadership approval. Eleven WPRN sites (33% of invited organizations) across Washington, Wyoming, and Idaho agreed to administer the survey to their providers. Seven were hospital-associated outpatient clinics; four were community health centers. Across participating clinics, the proportion of patients who are uninsured or receiving Medicaid or Medicare ranged from 30% to 80%. A research champion at each clinic site had the opportunity to provide feedback on the survey design and facilitated administration of the survey.
Measure
Survey questions were drafted based on items from questionnaires used in prior published CIH survey studies.17–20 The 19 survey questions covered the following topics: practice of and familiarity with CIH methods, support for and practice of CIH at the clinic, education and training in CIH, and respondent demographics. Specifically, the survey asked primary care providers if they had ever talked about CIH with their patients, if they would be willing to co-manage a patient with CIH providers, whether they would recommend CIH for specific health conditions, about their how familiar they were with different CIH methods (unfamiliar, familiar, tried/used approach in their own healthcare), about barriers to the integration of CIH modalities in their patient care, about their clinic’s level of support for providing CIH, whether their clinic has providers who can offer different CIH methods, if they have ever personally received any training in CIH, and about their level of interest in learning more about or in providing different CIH modalities. They were also asked about demographics such as age, gender, race, ethnicity, provider type, and training status.
The survey was pilot tested with three primary care providers to ensure comprehension and ease of response. The 19 survey questions covered the following topics: practice of and familiarity with CIH methods, support for and practice of CIH at the clinic, education and training in CIH, and respondent demographics. The survey was programmed into REDCap, a web-based software designed for data collection and storage. 21 A copy of the survey can be requested from the corresponding author.
Procedures
The online survey was sent via email to all eligible providers (n = 483) at each participating organization (n = 11) in November 2019, followed by three weekly reminders. The number of eligible participants per site ranged from 9–95. Participants were asked to complete the survey within one month of the initial request. Eligible providers were all primary care (Medical Doctor (MD), Doctor of Osteopathy (DO), Physician Assistant (PA) and Nurse Practitioner (NP) providers, including any resident/trainee providers, at the participating clinics.
Analysis
Responses were summarized descriptively as frequencies and percentages. Providers for each clinical practice were categorized as working at either an urban or rural-serving site based on the 2013 Rural-Urban Continuum Codes (RUCC). 22 Results were then stratified by urban/rural-serving practice location (rural-serving = a 3 or greater on the RUCC code) and by whether or not respondents were trainees, to compare differences in personal attitudes about and availability of CIH. Associations were analyzed using contingency table analyses (Chi-square, Fisher exact test) and by multivariate logistic regression. Stata v14.1 was used for all analyses. 23
Results
Respondent Demographics and Past CIH Training
There were 218 survey respondents, which represented a 45.1% response rate. The majority of respondents were under 40 years old (61.8%), female (57.2%), non-Hispanic/Latino (94.0%), and white (83.8%). Respondents were primarily physicians (91.5%) who worked in an urban healthcare setting (81.2%). About half were residents. Approximately half had taken a class on CIH (could be single or multi-day), although only one respondent had formal training via an integrative medicine fellowship. Less than 10% reported being dually trained in a CIH modality (Table 1).
Demographics (N = 218).
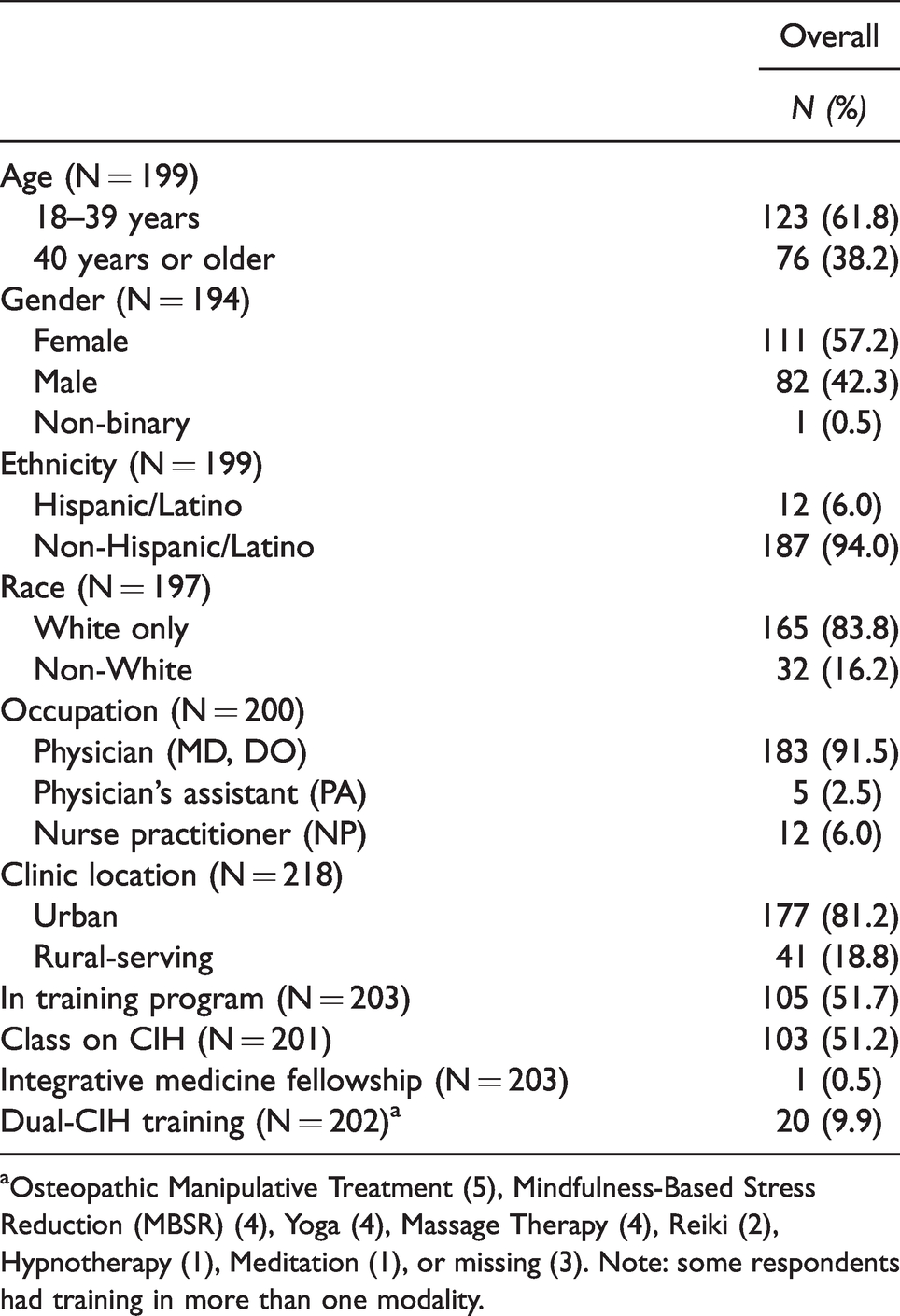
aOsteopathic Manipulative Treatment (5), Mindfulness-Based Stress Reduction (MBSR) (4), Yoga (4), Massage Therapy (4), Reiki (2), Hypnotherapy (1), Meditation (1), or missing (3). Note: some respondents had training in more than one modality.
CIH Familiarity and Perceived Benefits
Of the CIH modalities, chriopracty was the modality that the largest proportion of primary care providers were familiar (72.6%), followed by spirituality/prayer (66.9%), and supplements (66.2%). For each of the other modalities, at least 55% of providers were familiar with each modality except for curanderismo (8.0%), Ayurveda (23.3%), and therapeutic touch/Reiki (47.6%) (Table 2). In addition, many respondents reported they had personally tried or used meditation/mindfulness (56.1%), yoga (55.5%), and/or relaxation techniques (53.9%) for themselves, and a majority also reported having asked their patients about their use of meditation/mindfulness (61.7%), relaxation techniques (59.4%), and/or yoga (58.3%). On average, the respondents estimated that close to 50% of their patients would benefit from CIH, and 86% indicated that CIH would increase patient satisfaction with their care (data not shown in Tables).
Primary Care Providers’ Report on Specific CIH Modalitiesa (N = 218).

aParticipants were asked to select all that apply, so row percentages will not add up to 100%.
Attention to CIH Within Clinical Care
Most respondents (88.4%) said they talked to their patients about the possible benefits of or recommended the use of CIH modalities at least some of the time. While 62.2% had provided a referral for massage, less than 40% had provided referrals for any other CIH modality (Table 2). Most participants (89.4%) said they would be willing to co-manage a patient with a CIH practitioner, however only 41.5% had ever co-managed a patient with a CIH practitioner.
Integrative Care Within Clinics: Available Modalities and Barriers
All respondents reported that at least one CIH modality was available at their clinic (Table 2). The most commonly reported modalities provided within clinic were relaxation techniques (70.9%) and meditation/mindfulness (64.0%) (Table 2). Nearly two-thirds of respondents thought financial concerns were a significant barrier to integration of CIH, such as patients not being able to afford out-of-pocket costs (71.9%) or lack of insurance coverage of CIH modalities (65.8%). Not knowing who to refer to for CIH services was considered a significant barrier by 45% of respondents. In addition, other notable barriers to integration of CIH in primary care, included a lack of personal knowledge of the evidence (54% rated as somewhat significant), lack of trust in evidence (54% rated as somewhat significant), or a personal lack of familiarity (57.6% rated as somewhat significant). Lack of clinic leadership support for CIH was not considered a significant barrier (Table 3). Resident physicians were significantly more likely, compared to non-resident providers, to perceive their lack of knowledge of CIH efficacy as a barrier to CIH integration (44.2% vs. 27.4%, p-value = 0.047). Similarly, resident physicians were less likely to know local CIH providers for referrals (51.9% vs. 37.9%, p-value = 0.044).
Perceived Barriers to Integrating CIH into Primary Care Practice (N = 204).

Promoting Integrative Care: Increasing Knowledge, Referral Base, and Providing Services
The majority of respondents were interested in learning about the safety and efficacy of at least one CIH modality (78.4%). The modalities for which large proportions of respondents were interested included biofeedback (56.7%), supplements (51.8%), hypnosis (50.5%) and acupuncture (50%). Providers were most interested in knowing about local providers who they could provide referrals to for massage (72.9%), acupuncture (72.2%), yoga (69.9%), meditation/mindfulness (69.0%), and relaxation techniques (65.7%). Providers indicated little overall interest in providing integrative modalities themselves, with the exception of relaxation techniques (41.4%) and meditation/mindfulness (39.1%).
There were no differences in rates of interest in learning about CIH safety or efficacy between providers in urban vs. rural-serving practices. Resident physicians were significantly more likely to be interested in knowing about the safety and efficacy of at least one CIH modality compared to non-resident providers (89.5% vs. 77.6%, p = 0.021).There were no differences between residents and non-resident providers in their desire to know about which providers to refer patients to for services, or in their interest in providing CIH modalities themselves (Tables 4 and 5).
Training Interest by Clinic Location and Training Status (N = 218).

Note: *p < .05.
Training Interest by CIH Modalitya (N = 202).

aParticipants were asked to select all that apply, so row percentages will not add up to 100%.
bOsteopathic Manipulative Treatment.
Discussion
The results of this study of primary care providers across 11 clinics in three states highlight high rates of overall familiarity of primary care providers with CIH. The findings also indicate that providers have high levels of interest in referring to or co-managing care with a CIH practitioner. The results suggest that higher levels of provider personal experience with a specific CIH modality, and/or the availability of specific CIH modalities in the clinic, may positively influence providers’ asking patients about their use of that specific CIH modality. Likewise, higher levels of provider personal experience with a specific CIH modality may positively influence levels of interest in referring patients for these services. Similarly, a low level of provider personal experience with a specific CIH modality may negatively influence providers’ asking about patient use of that CIH modality. As might be expected, there was more familiarity and personal experience with mainstreamed CIH approaches (e.g. Mindfulness, Massage, and Yoga) and little familiarity or personal experience with approaches that are less so and likely used most by people from certain cultural backgrounds (e.g. Curanderismo, Ayurveda, Tai Chi). This finding may also reflect the racial/cultural background of the study sample which was predominantly non-Hispanic White, as are the majority (approximately 72.5%) of primary care physicians in the United States. 24 These findings highlight the potential impact of provider personal experience with CIH, and thus the critical importance of experiential learning in CIH education for providers, as shown in an initial longitudinal study of CIH in undergraduate medical education. 25
Providers indicated interest in learning more about the safety and efficacy of at least one CIH modality, particularly among medical residents who made up about 52% of the sample. These results indicate that increasing opportunities for residents to receive education and training about providing CIH and/or coordinating CIH care with community providers, would be acceptable. Importantly, increased educational opportunities could also address potentially significant barriers to wider recommendation of CIH by primary care providers, such as lack of familiarity, trust, and knowledge.
The recognition that approximately half of their patients would benefit from CIH approaches and that CIH approaches could increase patient satisfaction with care, suggests that primary care providers are looking to expand their ability to meet patients’ healthcare needs as well as an awareness of consumer demand for CIH. This is not surprising given the shift toward including CIH as a recommended treatment for some conditions common in primary care, for example in the treatment of chronic pain conditions (e.g. low back pain, arthritis, fibromyalgia), and irritable bowel syndrome.12,26–29 Even so, in this study only 40% had even once co-managed care with a CIH provider. Primary care providers noted lack of access to CIH providers to whom to make referrals as a significant barrier to integrating CIH into primary care practice, highlighting the need for more transdisciplinary contact and networking. These findings are aligned with findings from prior studies pointing to the critical importance of referral networks 15 and positive interprofessional communication15,30 between conventional and complementary providers as key themes for the success of CIH integration in primary care.
These study results showed that providers perceived a lack of financial coverage as the primary barrier to CIH. As providers are likely aware, insurance coverage for CIH providers varies by state, as well as within states. 31 Likewise federal funding through Medicare and Medicaid for CIH is minimal to non-existent, highlighting the lack of access to CIH for low income and underserved populations. This overwhelming recognition of the financial barriers to CIH from providers in this study supports the need for systemic policy changes to address patient financial barriers to accessing CIH modalities. 32
Study limitations that reduce generalizability of these findings include the lack of diversity in primary care provider types (i.e., vast majority were physicians), lack of diversity in age and race (majority were under 40 years of age and Caucasian), and greater participation by clinicians at urban vs. rural-serving clinics. It is also possible that clinicians who are more interested in CIH were more likely to complete the survey. However, the response rate of 45% is consistent the typical response rate for clinician surveys. Despite these limitations, there are distinct strengths of this study. Unlike many prior CIH studies that focus on a single clinic, this study was administered across multiple clinics in three northwest states, represents a regionally diverse (i.e. urban and rural) group of primary care providers, and included trainees (medical residents) and established primary care providers.
Conclusion
Primary care providers in the Northwestern region of the United States are generally familiar with many CIH modalities, believe their patients would benefit from CIH, are interested in referring to and co-managing care with CIH providers, and would like to have more learning opportunities to increase knowledge of the safety and efficacy of CIH. The results highlight several actionable areas to guide future efforts to increase patient access to CIH in primary care. These include creating opportunities for providers to network with local CIH practitioners in order to increase referral sources, increasing CIH services offered within clinics, increasing CIH education within medical training programs, and more continuing education opportunities for experienced clinicians. Longer term efforts for increased integration with primary care should address systemic issues of access, such as the need for private and public insurance coverage for CIH services. Likewise, this study points to the need for further and future study to better understand what actions are most helpful in CIH promotion, in what contexts, and among which types of providers.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was largely funded by the UW Osher Center for Integrative Medicine. This project was supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under Award Number UL1 TR002319. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.