
Abstract
Background:
Clinicians in the Emergency Center (EC) and Urgent Care (UC) can play a vital role in preventing hospital admissions and improving outcomes of patients with newly diagnosed diabetes or pre-existing diabetes who present with hyperglycemia and the need to initiate insulin.
Methods:
This article describes a unique EC/UC discharge insulin starter kit protocol with clinician instructions via an Electronic Medical Record (EMR) order set that includes: starting doses for insulin, a prescription for glucose monitoring supplies, and an emergent referral to diabetes education at International Diabetes Center. Patients receive insulin during the EC/UC visit and are provided an insulin pen to take home. Nurses from the EC or UC review and provide educational material on how to use an insulin pen, treating hypoglycemia and healthy eating. The Certified Diabetes Care and Education Specialist (CDCES) sees patients within 24-72 hours after the referral is placed.
Results:
Within our single healthcare system’s EC and UC (multiple sites), the kit has enabled clinicians to metabolically stabilize patients and decrease the need for hospitalization without experiencing hypoglycemia. In the recent three years of use, of 42 patients given the insulin starter kit, there were only 2 patients with repeat EC/UC visits within the first six months (1 hyperglycemia and 1 hypoglycemia).
Conclusions:
An insulin starter kit and EMR-based order set initiated in the EC/UC setting is a tool that can be used to improve the quality of care for people with newly diagnosed or pre-existing diabetes experiencing significant hyperglycemia.
Introduction
There are 34.2 million people in the United States living with diabetes, accounting for approximately 10.5% of the total population. 1 Over the past decades, diabetes care has become more costly, despite worsening outcomes. Hospital admissions for diabetic ketoacidosis (DKA) and hyperglycemic crisis have both increased over 30% from 1993 to 2015, despite the per capita annual cost of diabetes care increasing 228% from 2000 to 2016. 2 Many patients with diabetes go to the Emergency Center (EC) or Urgent Care (UC) for care that could take place in an outpatient setting. Indeed, those with risk factors most strongly associated with recurrent EC visit for diabetes are patients who could have been identified and managed outside of the EC setting, including those with previous EC visits for hyperglycemia, those on insulin, and those established with a family physician. 3 According to the US Centers for Disease Control and Prevention’s National Center for Health Statistics, in 2015, about 24% of all EC visits for patients aged 45 years and older were made by those with diabetes. 4 Of these estimated 12 million visits by individuals with diabetes (a rate of 92 per 1000 persons and an increase from 2012), 28% ended in inpatient hospital admission. A higher percentage of these EC visits for patients aged 45-64 years with diabetes had Medicare as their primary expected source of payment (24%) compared with the non-diabetes EC visits (14%), while a lower percentage of the EC visits for the same age group had private insurance (32%) as their primary expected source of payment compared with non-diabetes visits (38%). There is an urgent need for hyperglycemia/DKA prevention programs to reduce morbidity and costs and improve the quality of diabetes care delivery in the EC/UC setting. 5
EC/UC clinicians may face multiple barriers in providing care for patients with diabetes, however, including lack of familiarity with diagnostic criteria for diabetes, resulting in misdiagnoses (eg, repeated presentation of urinary tract infection), lack of awareness of safe, effective and easy-to-implement standing orders for insulin initiation, and lack of knowledge about lifestyle and pharmacologic diabetes management. Inconveniencing patients also is problematic, particularly if their follow-up care requires repeated UC visits for administration of insulin doses over a weekend.
Not all patients with diabetes seen in the EC or UC are newly diagnosed with diabetes, with most of these visits (87%) occurring in patients with an established diabetes diagnosis. 3 People with diabetes who cannot afford insulin or have lost insurance coverage often stop taking it and consequently present in the EC or UC for care related to hyperglycemia. In many ECs, patients needing to start insulin are hospitalized. In UC, if on a weekend for example, treatment often requires two visits a day to receive insulin, until they are seen by Certified Diabetes Care and Education Specialist (CDCES) or primary care, or patients are just sent to the EC for evaluation and possible hospital admission.
Safe, effective, and innovative ways to triage patients with diabetes in the EC or UC without hospitalization are needed, especially for those requiring insulin initiation or resumption, to help reduce hospital admission rates and costs, as convenience of care, while also improving outcomes.
The Role of EC and UC in Insulin Initiation
Patients presenting in the EC or UC with hyperglycemia needing insulin are not necessarily newly diagnosed with diabetes. Some patients with diabetes using EC or UC visits for their diabetes care may never have followed up with diabetes education or been to their primary care clinic for some time. Some may have stopped taking non-insulin diabetes medication or insulin previously prescribed. Unaffordability of diabetes medications or loss of or no insurance may also contribute to patients seeking care in the EC or UC, as diabetes medications are the second most costly therapy class of drugs. 2
Although the epidemic numbers of people living with diabetes has garnered national and worldwide attention, in a review of the clinical literature we did not identify any articles discussing the initiation of insulin in the EC or UC because of hyperglycemia without hospital admission.
In a study by Álvarez-Rodríguez et al 6 in Madrid, Spain, hyperglycemia is a common finding at hospital ECs in patients with diabetes, but little data are available on its frequency, management and subsequent impact based on the assessment made in the EC. The study found the prevalence of patients with diabetes admitted to the hospital from the EC to be very high. Additionally, there was a high trend of underestimating its significance, with hyperglycemia rarely reported as a diagnosis in the EC discharge report, whereas in standard hospitalization, the diagnosis was more common.
Bernard et al 7 examined the impact of an aspart insulin protocol for treatment of hyperglycemia in the EC, but the study investigated the impact when the protocol was coupled with rapid initiation of a detemir-aspart insulin protocol at the patients’ hospital admission. Palermo et al 8 did a single-center study of an EC rapid-referral program to a diabetes clinic but referrals were for patients with no evidence of hyperglycemic crisis and no other condition requiring hospitalization. Patients were started on insulin therapy during the diabetes clinic visit.
Rubin 9 promotes further study of transitioning patients with diabetes out of ECs to confirm efficacy and replicability of interventions that target high-risk patients to improve outcomes and lower costs. Echouffo-Tcheugui and Garg 10 note that evidence suggests that better management of hyperglycemia in the EC with proper follow-up improves clinical outcomes and prevents readmission. They also call for more clinical trial data on the outcomes and cost-effectiveness of various management strategies or protocols to optimize hyperglycemia management in the EC.
In a national survey by the Canadian Diabetes Association (CDA), 11 now Diabetes Canada, of attitudes and practice related to the awareness and use of CDA’s 2013 Clinical Practice Guidelines for the Prevention and Management of Diabetes in Canada among 500 randomly selected members of the Canadian Association of Emergency Physicians, the majority of respondents reported the guidelines to be useful (83.6%); more than half were familiar with the guidelines and more than half claimed to use them in clinical practice. The most frequently reported barrier to guideline implementation was a lack of education (56%). The results suggest the need to improve knowledge-translation strategies across ECs to standardize management strategies applicable in the EC for DKA and hyperosmolar hyperglycemic states.
The EC/UC Discharge Insulin Starter Kit protocol described in this article provides a model for how EC and UC healthcare providers, supported with minimal skills training and regular communication with diabetes specialists, can help patients presenting with hyperglycemia avoid hospitalization.
Methods
The IDC Park Nicollet EC/UC Discharge Insulin Starter Kit
The International Diabetes Center (IDC) at Park Nicollet is a research, education, and publication center, which is part of HealthPartners/Park Nicollet clinics and hospitals, a large integrated healthcare organization. IDC has created a “kit” to provide the education and guidelines for initiating insulin in one hospital EC and eight UC sites within the care system.
At Park Nicollet EC/UC sites, clinic staff compile the “Discharge Insulin Starter Kits” with clinician instructions, insulin supplies, and patient education handouts (Figure 1, Table 1). In the EC, kits are clearly labeled and stored in a bin. When the kit is used, the insulin pen must be ordered through the onsite automated medication dispensing system (in our case, we use Humalog 75/25 pre-mixed insulin pens [Eli Lilly, Indianapolis, IN, United States]). In the UC, kits are stored in a refrigerator including the insulin pen sample. In addition to differences between how the kit is maintained in Park Nicollet’s ECs and UCs, care can vary slightly. Often UC clinicians send patients to the EC, since the UC can only give patients up to 1 L of fluids and may not have full access to quick laboratory results that would impact management. The IDC education manager follows up with the EC/UC medical director if the order set is not implemented, when indicated. Trusted communication provides EC/UC clinicians ongoing feedback for improving this workflow.
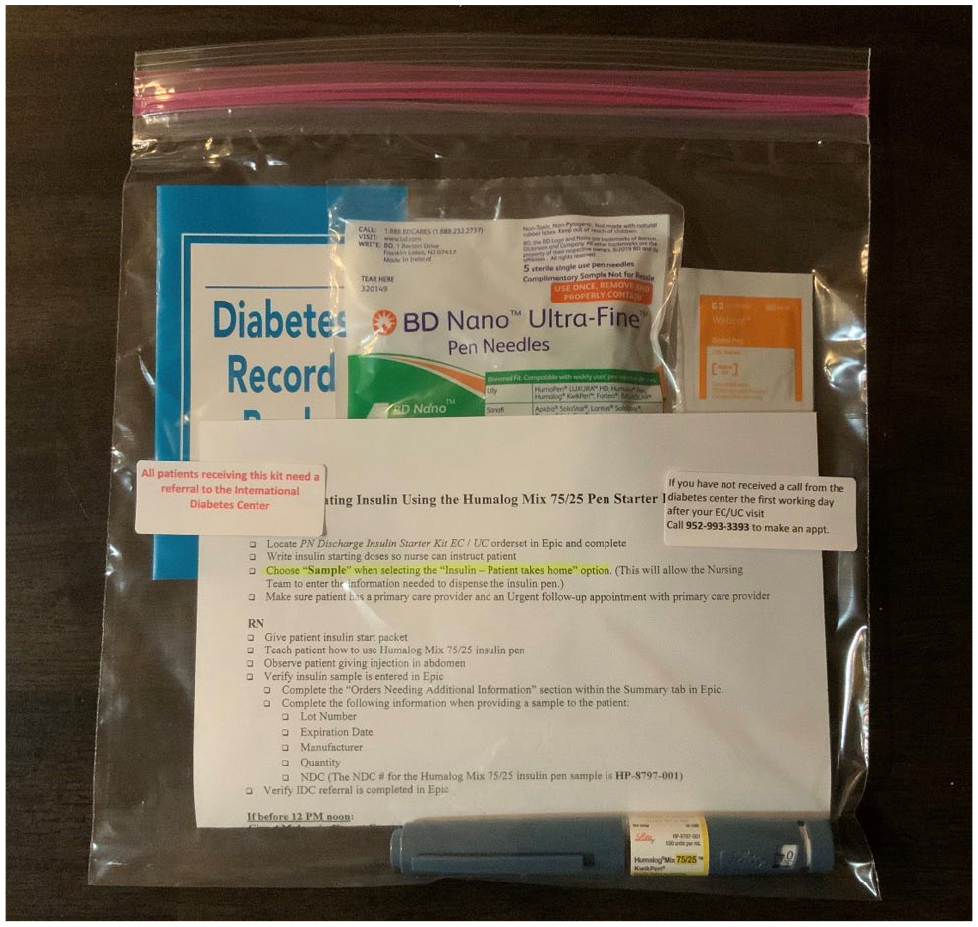
The Insulin Starter Kit. This kit contains instructions for both the EC/UC clinic staff, patient information about testing glucose and diabetes self-management, insulin pen needles, alcohol pads, and a glucose log book. The insulin pen opened during the patient’s EC/UC visit is also sent home with them in the kit.
Components of the EC/UC Insulin Starter Kit Program.

Abbreviations: CDCES, Certified Diabetes Care and Education Specialist; EC, Emergency Center; EMR, Electronic Medical Record; UC, Urgent Care.
Clinician Instructions
The first component of the kit provides EC/UC clinicians and registered nurses (RNs) with instructions for locating and completing the order set in the Electronic Medical Record (EMR) (Epic, Verona, WI, United States). The order set then prompts the ordering clinician to order the insulin (using pre-populated weight-based dosing), lab tests including hemoglobin A1c (HbA1c) and metabolic panel, an emergent referral to IDC Education (to be seen within 24-72 hours), and a statement of acknowledgment from the order provider that they are allowing for one visit to the IDC educators, so that the CDCESs can follow standing orders prior to obtaining a renewal referral from the patient’s primary care provider (Figure 2).
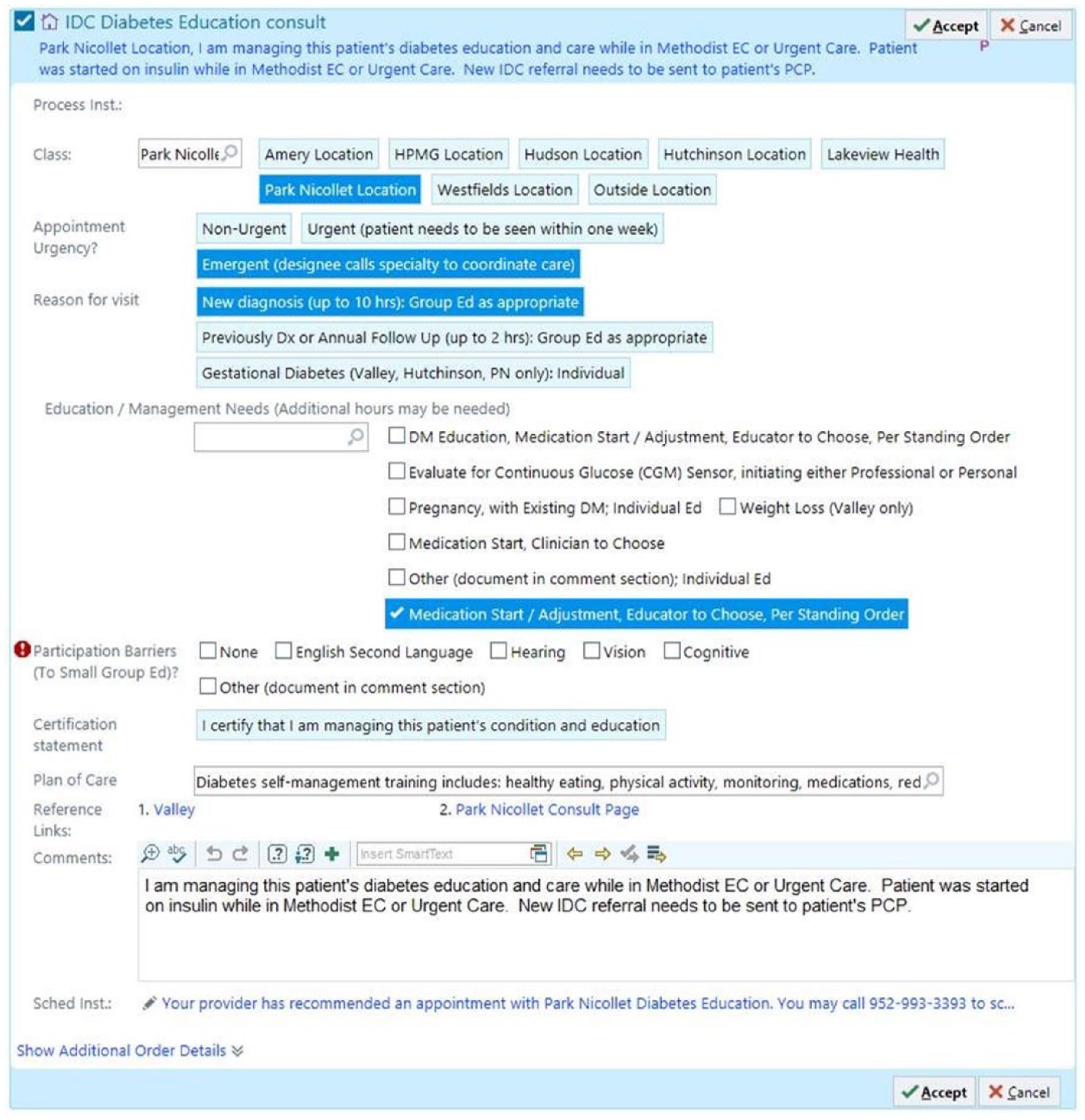
Screenshot of the actual order set in the EMR for diabetes education from the EC/UC setting. © 2020 Epic Systems Corporation.
Instructions take into account timing of first insulin dose given in the EC/UC. Tables (and an example) are provided to the EC/UC staff for determining insulin doses to direct adult patients to take at the EC/UC and at home. Dosing is weight-based according to the patient’s symptomology, glucose level, ketone level, and HbA1c (Figure 3). Guidelines also are provided for UC clinicians for sending the patient to EC.
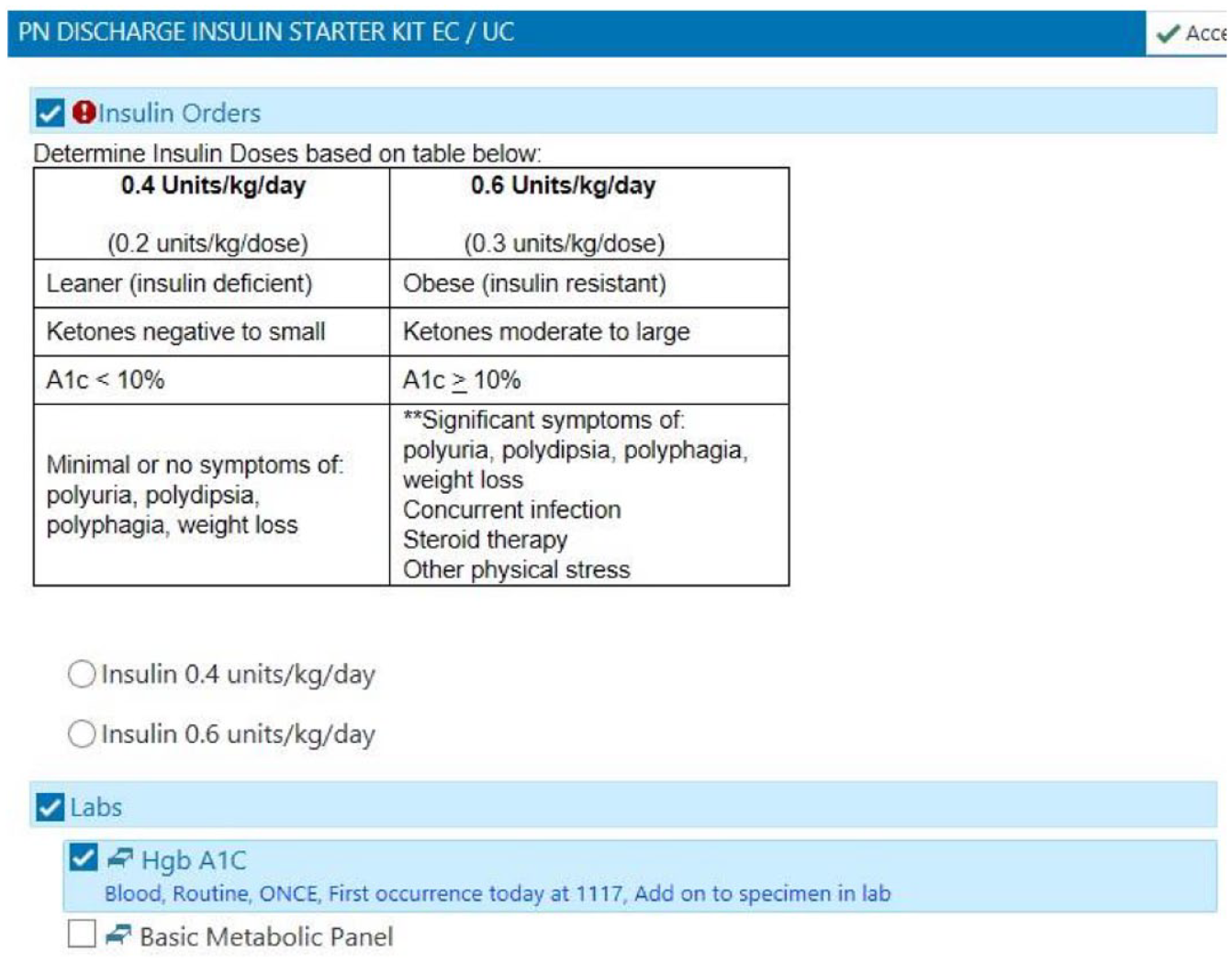
Screenshot of the weight-based insulin dosing calculator instructions to the EC/UC clinicians to simplify insulin dosing decisions and accompanying laboratory orders. © 2020 Epic Systems Corporation.
Other instructions direct the RN specifically through education steps to teach the patient. This includes giving the patient an insulin pen, explaining how and when to use it (observes patient giving first injection dose in the abdomen), as well as how to store it. Additional instructions guide the RN in discussing supplies needed for checking glucose to pick up at the pharmacy, and how to record glucose results in the record book provided.
The checklist of instructions also addresses verifying that the insulin pen sample is documented in the EMR as well as ensuring the emergent education referral to IDC has been placed (IDC will call the patient to schedule an appointment within 24-72 hours with a CDCES).
Lastly the instructions direct the RN to point out the patient education handouts in the kit and instruct the patient to drink water to stay hydrated. Should any questions arise before the patient’s education visit, they are to call their primary care clinician.
Insulin Pen and Supplies
A second component of the kit includes a pre-mixed insulin pen, ten pen needles and alcohol prep pads. A generic prescription for glucose testing supplies and a glucose meter are sent to the patient’s pharmacy, and dispensed per that patient’s insurance formulary preference or lowest cost meter system for patients lacking insurance.
Patient Education Materials
The third component of the kit includes four education handouts to promote immediate diabetes management or modification. These are all written at the fifth grade level, and are available only in English. For those newly diagnosed with diabetes, a general piece provides an overview of what diabetes is, how the body uses glucose, causes and types of diabetes, risk factors for diabetes, symptoms, and diagnosis and treatment of diabetes.
Another handout focuses on high and low glucose, with an emphasis on the importance of understanding the causes, symptoms, and treatment of both high and low glucose. The patient is instructed in the prevention, recognition, and management of high and low glucose.
A third handout provides step-by-step instructions for measuring and injecting insulin using an insulin pen. This piece helps reinforce what the RN taught during the EC/UC visit. Information on where to inject insulin includes an illustration.
A fourth handout introduces meal planning using the plate method and dismisses some misconceptions about carbohydrates and foods with sugar. Tips help patients gain an understanding of how what they eat, how much they eat, and when they eat can affect their glucose level. Example meals compare healthier foods with less healthy foods.
Data regarding the HbA1c at presentation and between one month and six months afterwards, prior insulin use, attendance to their emergent diabetes education appointment, race, and type of diabetes were also collected.
Results
EC and UC clinicians following the order set helped patients decrease their acute glucose with no occurrences of hypoglycemia or DKA during their initial EC/UC visit. EMR data regarding the insulin starter kit have been tracked since early 2017.
Patients requiring insulin initiation or resumption are seen in Park Nicollet’s EC or UC any day of the week, as well as on weekends. In earlier years of using the kit, patients were more typically seen or hospitalized over the weekend. However, with the increased costs of insulin and loss of or lack of insurance, patients are more often seeking care in the EC or UC on any day of the week.
From January 1, 2017 through December 31, 2019, there were 42 patients who used the insulin starter kit protocol in the EC/UC (Table 2). Over the same time period, there were 90 patients seen in the EC/UC who had an emergent referral to diabetes education placed who were not enrolled in the insulin starter kit protocol. Within the first six months following the initiation of the insulin starter kit, only one patient had a subsequent admission for DKA, and only one patient had subsequent EC visit for hypoglycemia. The patient with DKA did not schedule follow-up with our CDCES and ran out of insulin; the patient with hypoglycemia was a patient with newly diagnosed type 1 diabetes. For those not starting on the insulin starter kit protocol, there was no severe hypoglycemia, and only one episode of DKA in the subsequent six months, which occurred outside of our system and no details were available. Of note, all 42 patients started on the kit were insulin naïve, whereas 22 patients (24%) with an emergent referral to diabetes education but not using the kit were previously on an insulin-based regimen. The most commonly identified reason for the group not placed on the protocol being seen in the EC/UC was for running out of or discontinuation of their insulin or other diabetes medications.
Demographics and Outcomes from January 1, 2017 through December 31, 2019 for Patients with Emergent Diabetes Education Referral from the EC/UC (Column A) Given the Insulin Starter Kit Protocol and (Column B) for Patients Not Given the Insulin Starter Kit Protocol.

Abbreviations: DKA, diabetic ketoacidosis; EC, Emergency Center; UC, Urgent Care.
A reduction in HbA1c was seen for both those started on the starter kit protocol and those who were not (Table 3). The patients given the insulin starter kit protocol saw their mean HbA1c decrease from 11.7% at presentation to 7.8% HbA1c (delta HbA1c, −3.9%) in the one-month to six month time period following the intervention. Of these 42 patients, 9 (21.4%) no-showed for their emergent CDCES appointment. The patients with an emergent referral to education who did not start on the starter kit (n = 90) saw their mean HbA1c decrease from 11.0% to 8.7% (delta HbA1c, −2.3%) during the same time period. Of these 90 patients, 32 patients (35.6%) no-showed to their emergent CDCES appointment. While complete data are lacking for all of the 132 patients, the percent of patients at presentation and at the one-month to six month post-EC/UC visit periods with an HbA1c <8% increased from 0% to 42.6% for those initiated on the insulin starter kit protocol, compared with an increase from 7.8% to 25.6% for those not started on the protocol.
HbA1c Outcomes in Patients with Hyperglycemia and an Emergent Referral to Diabetes Education Who Were Given or Not Given an Insulin Starter Kit.
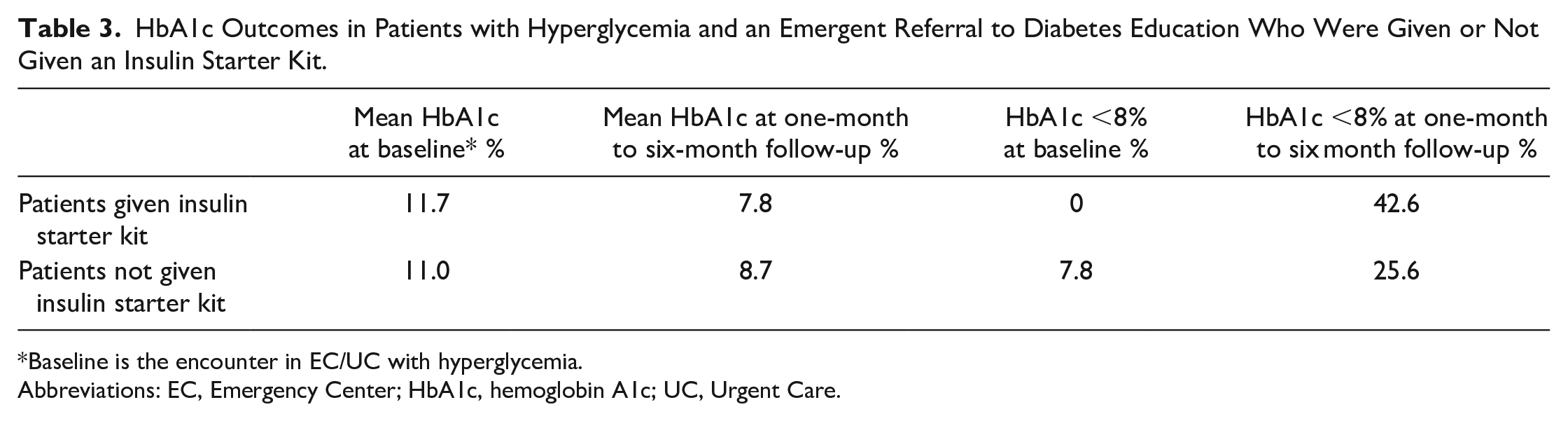
Baseline is the encounter in EC/UC with hyperglycemia.
Abbreviations: EC, Emergency Center; HbA1c, hemoglobin A1c; UC, Urgent Care.
Discussion
The IDC Park Nicollet EC/UC Discharge Insulin Starter Kit provides a safe, clinically effective and potentially cost-saving strategy for initiating insulin to patients who have hyperglycemia without having to admit them to the hospital for treatment. The kit enables EC/UC clinicians easy-to-implement, EMR-based standard orders and instructions for teaching patients how to inject insulin doses before following up with further diabetes education and management within 24-72 hours. The kit also provides several handouts to help patients learn about diabetes, measuring and injecting insulin using an insulin pen, recognizing and managing high and low glucoses, and following a healthy eating plan.
A good working relationship between the EC/UC and IDC/endocrinology clinicians is also critical. Skills training is provided annually to UC nurses, which helps keep the UC clinical staff familiar with the use of glucose testing devices and insulin administration. For instance, review with a saline pen is a focus of the annual skills training. The use of our EMR and ongoing review of workflow processes as well as the auto referrals to diabetes education at IDC assures that clinicians are entering the appropriate referral. It is also worth noting that the patients offered the insulin starter kit were more likely to show for their emergent education visit within 72 hours supports that perhaps the insulin sent home with the patient or the educational materials offered helped engage these patients in their care. Indeed, in Minnesota clinics and healthcare systems, the threshold for meeting statewide quality of care targets is an HbA1c <8%. It is notable that the insulin starter kit protocol increased the number of patients meeting this by 42.6%, compared with just 17.8% for the patients who did not use the protocol.
There are several limits to our quality improvement project. First, it is not certain that such an insulin starter kit program would be easily implemented in other EC/UC systems that may not have as direct of a connection to a comprehensive diabetes education program, or systems that may be more decentralized. Further, additional evaluations are needed to see if this program would be successful in areas where EC/UC is not integrated at all with a diabetes education program/endocrinology clinic. Indeed, we did observe a decrease in HbA1c levels in both groups who were emergently referred to diabetes education, though the HbA1c decrease was numerically higher with those started on the insulin starter kit protocol. The number of patients included in our analysis and the very low number of events of hypoglycemia/DKA in both groups does make it difficult to show improvements based on those metrics, however the larger decrease in HbA1c and lower no-show rate to education appointments for the insulin starter group suggests at least some aspect of this program may improve patient engagement. Although additional investigation is needed to evaluate the protocol’s effectiveness on outcomes and cost effectiveness, we believe it provides a step forward to improve clinician awareness and confidence in starting patients with hyperglycemia on insulin without hospitalization, along with immediate follow-up diabetes education for these high-risk patients.
Conclusions
An EMR-based order set initiated in the EC/UC setting, utilizing an insulin starter kit and very close follow-up with diabetes education, may be a tool that can be used to improve the quality of care for people with diabetes.
Footnotes
Acknowledgements
The authors thank the clinicians within the EC, UC, endocrinology and CDCESs for their collaboration on this ongoing project.
Abbreviations
CDA, Canadian Diabetes Association; CDCES, Certified Diabetes Care and Education Specialist; DKA, diabetic ketoacidosis; EC, Emergency Center; EMR, electronic medical record; RN, registered nurse; UC, Urgent Care.
Author Contributions
JLD, JAC and RMB developed the IDC Park Nicollet EC/UC Discharge Insulin Starter Kit standing orders, order set and kit; JAC conducted patient chart evaluation; JLD and RT primarily wrote the paper, RMB and ALC provided analysis, interpretation of data, and all authors read and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: ALC has received research support and/or provided consultation for Medtronic, Abbott, Sanofi, Dexcom, Insulet, Eli Lilly, Novo Nordisk, and UnitedHealthcare. RMB has received research support, consulted, or has been on a scientific advisory board for Abbott Diabetes Care, Ascensia, CeCur Corporation, DexCom, Hygieia, Insulet, Johnson & Johnson, Lilly, Medtronic, Novo Nordisk, Onduo, Roche, Sanofi, and United Healthcare. His technology research is funded in part by NIH/NIDDK. ALC’s and RMB’s employer, non-profit HealthPartners Institute, contracts for their services and no personal income goes to ALC or RMB. JLD, JAC, RT have no relevant disclosures.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.