
Abstract
Delays in cancer treatment are detrimental across nearly every disease site in oncology including head and neck cancer. This study aimed to evaluate the impact of same-day access for patients with newly diagnosed head and neck cancer referred for radiation therapy consultation. From March 2021 to March 2023, a total of 50 consecutive patients who completed curative treatment were matched to a control subject who did not use the same-day initiative based on age, gender, histology, performance status, primary tumor site, stage, p16 status, treatment, and smoking history. With a median follow up of 30 months, there were no differences in 3-year overall survival, progression-free survival, or local-regional control between the 2 cohorts (P > .05, for all). However, the same-day access initiative was associated with significant reductions in time from diagnosis to first day of radiation (49 days vs 71 days, P < .001); time from diagnosis to completion of diagnostic work-up (32 days vs 43 days, P = .01); and time from diagnosis to completion of all treatment (91 days vs 111 days, P < .001).The same-day access initiative was associated with significant reductions in time from diagnosis to first day of radiation (49 days vs 71 days, P < .001); time from diagnosis to completion of diagnostic work-up (32 days vs 43 days, P = .01); and time from diagnosis to completion of all treatment (91 days vs 111 days, P < .001). The same-day access initiative thus enhanced multidisciplinary coordination and expedited treatment for patients with head and neck cancer.
Introduction
While the reasons underlying delays in cancer care are multifaceted and influenced by a slew of patient- and system-related factors, the downstream ramifications can be profoundly detrimental.1-3 A recently published analysis that reviewed 34 different studies including over 1 million patients demonstrated that every 4 weeks delay in cancer treatment can increase the risk of death by 10%. 3 Notably, the effects of delay are thought to be particularly pronounced in patients with rapidly dividing tumors. For patients with newly diagnosed head and neck cancer, the importance of both beginning and completing treatment in a timely fashion has been well established.4-6 Among those requiring radiation therapy, the emphasis on expediency is particularly germane because from a radiobiological standpoint, treatment is most likely to be successful with a smaller burden of tumor since with each passing day, the ability of cancer cells to not only divide but to develop resistant phenotypes increases. 7 The likelihood of distant metastasis also increases as the tumor size grows. 8 Huang et al 9 reviewed 46 studies to study the relationship between delays in initiating radiation and outcomes and showed that local control was significantly compromised for patients receiving radiation for head and neck cancers when delays were prolonged. Additionally, patients who wait longer for treatment experience more psychosocial distress and suffer from disproportionately higher rates of depression and anxiety. 10
However, the management of head and neck cancer is heavily dependent on multidisciplinary coordination and well-known for its logistical complexities in treatment decision making. Given the operational barriers potentially involved in scheduling and maintaining appointments, same-day visits have been proposed as a means of improving access. 11 However, the data on its impact on its feasibility have largely been limited to anecdotal experiences and case reports. This study compares the outcomes, specifically those related to system-based quality metrics related to access and workflow, of patients with head and neck cancer opting for same-day consultation to those who were seen in the traditional, episodic manner in the outpatient setting.
Methods and Materials
Patient Population
This study was approved by the Institutional Review Board at the University of California, Irvine (#2589) prior to the retrospective collection of all patient information. From March 2021 to March 2023, a pilot initiative was conducted such that all new patients referred to a tertiary care-based radiation oncology department affiliated with a National Cancer Institute-designated Comprehensive Cancer Center were deliberately offered the ability to be seen as a same-day consultation. The only pre-requisite was successful obtainment of prior insurance authorization. During this time period, a total of 57 consecutive patients among all 379 (15%) with cancer originating from the head and neck region were seen via same-day consultation. Among these, the 50 patients with head and neck cancer who completed curative treatment for local-regional disease formed the primary patient population of this analysis.
A flow diagram illustrating the pathway after initial patient contact is shown in Figure 1. Each morning before 8:00am, all pre-authorized referrals collected from the prior overnight hours were compiled at a daily huddle at which time a designated intake team contacted patients for scheduling. Schedulers were instructed to use the following verbiage to be as explicit and consistent as possible with patients: “Would you like to be seen by one of our radiation oncology specialists today?” Clinic slots were available in 1h increments from 1pm to 5pm, with last typically offered at 4:30, but in some cases 5:00. Referrals that arrived subsequently throughout the day, whether from the electronic health record system or via direct contract from referring physicians or patients were scheduled similarly. The general rule was that a same-day appointment was offered as long as initial contact was made before 11:00am. This time cut-off was selected to ensure sufficient time for logistical coordination. All patients who satisfied this criterion were offered a same-day appointment without exception. Inpatient referrals as well as patients seen in the Emergency Department were excluded.

Flowchart demonstrating the process of offering same-day access appointments.
Each of the 50 patients who opted for same-day access was subsequently matched to 1 patient with control head and neck cancer who did not opt for same-day consultation during the same time period. Matching was based on age (±5 years), gender, histology, Eastern Cooperative Oncology Group (ECOG) Performance Status, primary tumor site, 2016 American Joint Committee on Cancer (AJCC) disease stage (stage I/II vs stage III/IV), p16 status, primary treatment (surgery and postoperative radiation therapy vs radiation therapy alone), smoking history, and use of chemotherapy. Although every attempt was made to match precisely based on each of the above variables, this was only successful in 47 of the 50 never-smoker cases. However, in the 3 incidences where a perfectly matched control subject was unavailable, priority was given toward the following factors: gender, primary tumor site, histology, AJCC disease stage, and primary treatment. Using these prioritized factors, all patients seen as same-day consultations were successfully matched with an eligible control patient for the purpose of this matched-pair analysis.
Statistical Analysis
Clinical, disease-specific outcomes between the same-day access patients and their respective controls were initially compared using the Kaplan-Meier method with respect to the endpoints of overall survival, progression-free survival, and local-regional control. 12 Local-regional control was judged to have been attained if there was no evidence of tumor growth at the primary site or regional lymph nodes based on clinical and radiographic findings at follow up. All disease recurrences were biopsy proven. Comparisons among groups were performed with 2-sided log-rank tests with events measured from the first day of radiation therapy. Statistical analyses were performed using SAS version 9.4. Tests analyzing the difference between the distribution of characteristics and the proportions in each cohort were performed using either a χ2 statistic, or the Fisher exact test when more than 2 categorical variables were used. All tests were 2-tailed, with P < .05 considered statistically significant. Quality-related, system-based benchmarks related to treatment timeliness which were analyzed included time to first day of radiation; time to completion of diagnostic work-up (including all imaging studies); time to completion of all treatment; and time to acquisition of insurance authorization. These operational metrics were selected based on their practical significance as commonly assessed guide points for patients and providers in the delivering expedient care.
Results
Demographics
Patient and disease characteristics of the 2 groups are listed in Table 1. As expected, no significant differences existed between the 2 groups with respect to the matching variables (P > .05, for all). The patients ranged in age from 39 to 80 years, with a median of 55 in the same-day access group and 57 in the control group. The most common primary sites among the same-day access group were the oropharynx (20 patients), oral cavity (12 patients), followed by the skin (7 patients), salivary glands (5 patients), and larynx/hypopharynx (3 patients). Thirty-five patients (70%) were treated with definitive radiation; and 15 patients (30%) were treated with surgery and postoperative radiation. Concurrent cisplatin chemotherapy was administered to 23 patients (46%). Forty patients (80%) had an ECOG Performance Status of 0 or 1. Follow-up time ranged from 9 to 50 months with a median duration of 30 months for all patients. The follow-up time did not differ significantly between the 2 groups and was 30 months for the same-day access patients and 33 months for the non-same-day access patients (P = .77).
Patient Characteristics.
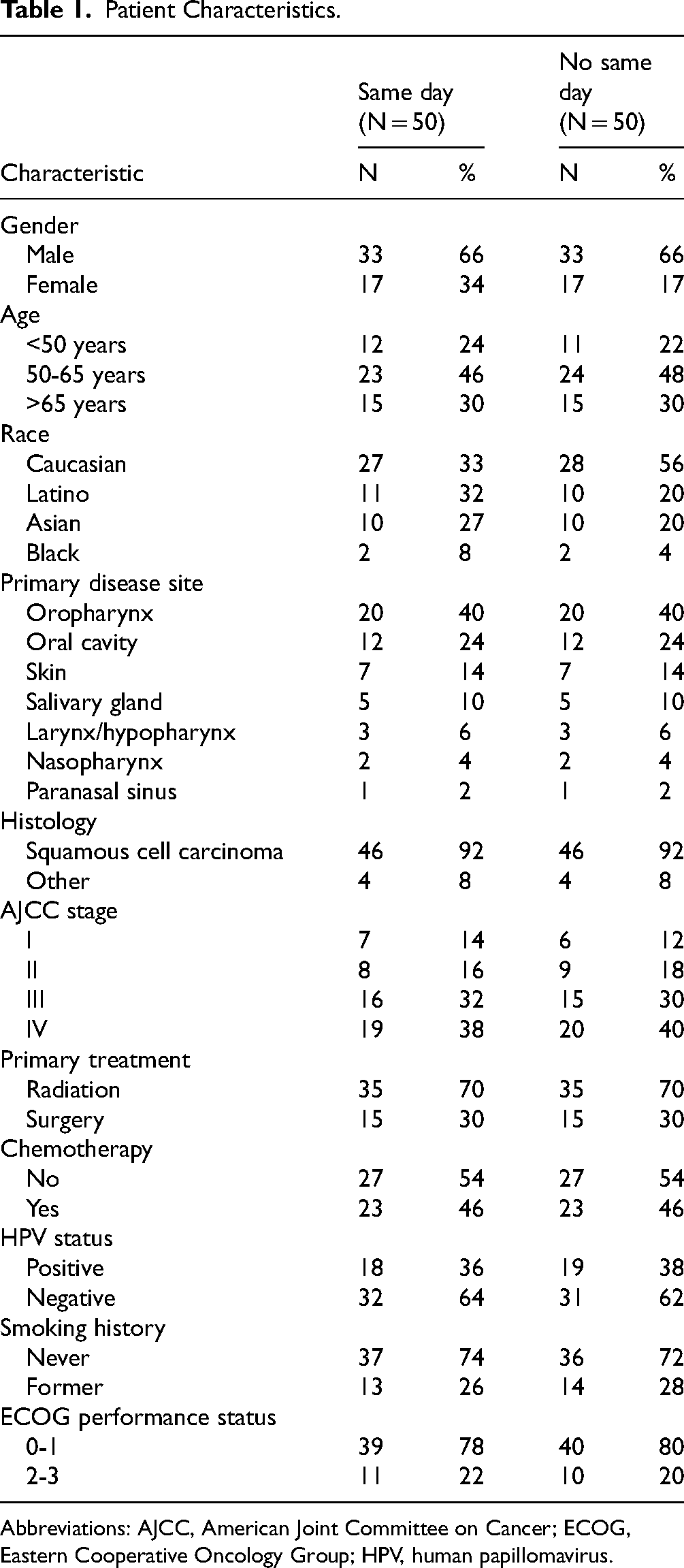
Abbreviations: AJCC, American Joint Committee on Cancer; ECOG, Eastern Cooperative Oncology Group; HPV, human papillomavirus.
Outcome Analysis
Figure 2 illustrates overall survival for the same-day access patients compared with the non-same-day access control group. The 3-year actuarial estimates of overall survival were 79% and 75%, respectively (P = .59). Fifteen of the 50 (30%) same-day access patients experienced disease recurrence (first site of relapse: 8 local-regional, 7 distant) compared with 18 of the 50 (36%) control patients (first site of relapse: 10 local-regional, 8 distant). As illustrated in Figure 3, the corresponding 3-year rates of progression-free survival were 69% and 62%, respectively (P = .35). The 3-year rates of local-regional control were 80% and 77% among same-day access and non-same-day access patients, respectively (P = .32).

Overall survival based on utilization of same-day access consultation (yes or no).

Progression-free survival based on utilization of same-day access consultation (yes or no).
Operational Analysis
Table 2 illustrates access-related benchmarks related to treatment between the 2 cohorts. Same-day access patients with head and neck cancer had significantly expedited duration with respect to all metrics including time from diagnosis to first day of radiation (49 days vs 71 days, P < .001); time from referral to first day of radiation (23 days vs 37 days, P = .01); time from diagnosis to completion of diagnostic work-up (32 days vs 43 days, P = .01); time from referral to completion of diagnostic work-up (7 days vs 21 days, P < .001); time from diagnosis to completion of all treatment (91 days vs 111 days, P < .001); and time from referral to completion of all treatment (72 days vs 94 days, P < .001). Additionally, the time from diagnosis to acquisition of insurance authorization for treatment was significantly reduced with the same-day access initiative (10 days vs 17 days, P = .02).
Effect of Same-Day Access Initiative on Treatment-Related Quality Benchmarks.

Abbreviation: RT, radiation therapy.
Discussion
The management of head and neck cancer is heavily dependent on multidisciplinary input and well-known for its complexities in treatment decision making. Due to challenges with respect to logistical coordination, patients often experience fragmented care that can compromise quality of care. 13 Not only can delays in care adversely affect clinical outcomes, barriers to accessing the cancer care continuum can also contribute to psychosocial distress and decreased treatment compliance for patients. 10
Given the potential effects of head and neck cancer on basic human functions such as speaking, eating, swallowing, and breathing, the need for streamlined flow in care coordination is imperative. This is particularly the case since patients frequently see multiple specialists and ancillary services across a diverse range of settings prior to starting and during treatment.
The findings from the present study showing the effect of a same-day access initiative in expediting care for patients with head and neck cancer are thus striking. Although the relatively small sample size likely precluded the demonstration of any benefit with respect to the clinical endpoints of survival or disease control, it is nonetheless noteworthy that operational metric related to the timeliness of care were all improved. In other words, the same-day access initiative tangibly improved clinical efficiency using a variety of objective and longitudinal performance-based metrics for patients with head and neck cancer.
The importance of timely treatment, as measured by a variety of different metrics, has been well established in head and neck cancer.4-6 From a practical standpoint, the barriers to starting treatment are likely related to the sheer complexity of coordination encompassing the entire gamut of care from diagnostic evaluation to multidisciplinary care. The experience of the Danish Head and Neck fast-track program is particularly instructive, as it showed that immediate referral for evaluation once symptoms were confirmed accelerates the pathway toward treatment, particularly with the summoning of resources. 14
Others have shown that dedicated multidisciplinary clinics are useful for the management of head and neck cancer in expediting care.15-17 This is important because studies have shown that decision can often be changed as patients move from one provider to another. 17 For instance, investigators from the University Medical Center Groningen in the Netherlands reported on how the development of a “multidisciplinary first-day consultation” clinic impacted access and optimization of care. 18 Similar to the results of the present series, they showed significant reductions in the time to primary treatment as well as time to diagnostic procedures. Additionally, the percentage of new patients treated within the Dutch standard of 30 calendar-days after intake increased from 52% to 83%. Toustrup et al also compared the outcomes of 446 patients with head and neck cancer enrolled on a “fast track” program over the course of a year to those presenting in the preceding year. They demonstrated that the time from referral to treatment and until initiation of treatment was reduced from a median of 26 to 15 days. As importantly, the initiative also reduced overall treatment time from a median of 57 to 29 days. 19
The most impressive finding of the present initiative was the dramatic reduction in the wait times for patients as measured from the time of referral to their actual start of treatment. The fact that only a small percentage of the patients who were seen as same-day access consultations ended up seeking treatment elsewhere suggests that retention and compliance could also possibly be enhanced with this practice. These observations demonstrate the potential of same-day access in helping the oncology community transition to value-based care models, particularly for higher acuity patients such as those with head and neck cancer.
It is arguable that one of the primary appeals of same-day access was its effect on decreasing potential barriers to travel. Head and neck cancer is notorious as one where the demands of having to see multiple providers (head and neck surgery, medical oncology, radiation oncology, radiology, etc) over a short period of time to complete work-up and staging can be overwhelming. Moreover, the subsequent preparation and coordination of treatment often requires multiple modalities and visits for ancillary services (speech and swallow, audiology, gastroenterology, and dental, to name a few) which can not only add to anxiety but also contribute to additional delays. Thus, patient-centric initiatives to alleviate any potential “bottlenecks” should be embraced. Given that traditional multi-appointment clinics that are episodic and geographically distant can result in delays in initiation of care as patients travel to see the individual specialists on different days, the inherent benefits of same-day access are obvious.
However, the influence of selection bias in the interpretation of these findings must be acknowledged. For instance, patient preference is a potentially unmeasured confounder that could have contributed to some of the differences in observed outcome between the groups. Since those opting for the same-day access initiative possibly could have been more motivated to pursue treatment and thus be more compliant with care, it is possible that the operational improvements were driven by patient-related rather than system-related processes.
Others have proposed interventions to shorten wait times for patients diagnosed with head and neck cancer once consultation has already been completed.20-22 For instance, Duggar et al 20 showed that the implementation of 2 interventions (upgrade of the treatment planning system and development of an automated patient management and accountability system) could strategically improve radiation therapy workflow resulting in quicker turn-around time to initiation of treatment. Patient navigation has also been proposed as a potentially robust means of enhancing the timeliness of care. 21 Graboyes et al 22 showed that intervention utilizing patient education, travel support, standardized processes for discussion, and organization re-structuring, among others, could all contribute to more efficient workflow. Notably, investigators from Australia, Canada, and New Zealand have all demonstrated the feasibility of same-day simulation and treatment for patients requiring radiation, albeit in the palliative setting.23-25
Future avenues for research will focus on the integration of artificial intelligence and machine learning algorithms into the same-day access paradigm to optimize workflow. The use of more sophisticated analytical techniques to track patient waits in real time also have the potential to refine this delivery model. Methods to address social determinants that might impede timely care including those related to transportation, employment, education, and/or housing, among other considerations, will also need to be considered to make access improvement scalable across all segments of the population.
In conclusion, an increasing amount of data now exists showing that patients desire an individualized approach to care with a focus on expediency. Due to the complexities of care traditionally involved in head and neck cancer, the development of value-based programs such as same-day access to promote patient empowerment are particularly important. Given the dramatic improvement in the operational metrics used to assess quality of care observed among patients opting for same-day consultations, continued efforts focusing on patient-centric access seem warranted.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
This research was approved by the UCI Institutional Review Board (Approval #5283) on June 14, 2024.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
A waiver of consent was obtained for this retrospective research.
Statement of Human and Animal Rights
This study was approved by the local institutional review board.