
Abstract
Background
Authoritative research demonstrating efficacy of traditional dysphagia therapy for Head & Neck Cancer (HNC) patients is limited. A 2019 survey reported speech-language-pathologists (SLPs) have started using Manual Therapy (MT) to prevent or rehabilitate dysphagia in HNC patients. This application of MT is supported theoretically but no research has established efficacy. Further, specific contents of MT protocols employed in this setting remain unknown.
Objectives
In the absence of HNC dysphagia specific MT protocols, this study aimed to better understand MT protocols employed by SLPs to prevent and treat dysphagia in HNC patients during and after Radiation Therapy (RT).
Methods
An internet-based questionnaire for SLPs who use MT with HNC patients was developed and tested for face/content validity. It was sent to SLPs practicing in the USA, twice, through three national listservs (ASHA-SIG13, ASHA-SIG3, University of Iowa Voiceserv).
Results
Of 64 respondents, 44 completed the survey. Of the 44, 15(34%) provided proactive MT during RT, 37(84%) provided proactive MT after RT (to prevent dysphagia), and 44(100%) provided reactive MT after RT (to treat dysphagia). 40(91%) were trained in MT through a CE course and 25(57%) had HNC-specific MT training. The most common MT techniques were laryngeal manipulation (LM) and myofascial release (MFR). During RT, MT protocols are gentler and highly tailored, with simple home programs of mild intensity. After RT, protocols are more regimented and aggressive, but still highly customized, with more diverse home programs of at least moderate intensity.
Conclusion
MT for HNC patients lacks a standard protocol or approach, but MFR and LM, or components of those techniques, are used most frequently. Given the frequency with which MFR and LM are employed to treat dysphagia during and post-RT, and the lack of empirical evidence supporting or refuting their use, a collaboratively designed RCT is warranted to establish the safety and efficacy of MT for HNC patients.
Introduction
Each year, Head and Neck Cancer (HNC) accounts for 500 000 new cancer cases worldwide and approximately 39,000 cases in the United States.1,2 While early stage (I and II) HNC has a high curative rate via surgery or radiation alone, HNC is typically diagnosed in the late and advanced stage (III and IV) due to ambiguity of symptoms. 3 Treatment of advanced HNC is more complex, and often requires a multimodality approach including surgery, radiation therapy (RT) and/or chemotherapy (CT).2,4,5 Studies suggest that combined chemoradiation therapy (CRT) and modern improvements in RT techniques have facilitated greater local tumor control and increased survival rates for advance stage HNC patients.4,6-9 However, these advancements in treatment are often accompanied by increased acute and long-term toxicity burden for patients.6,8,10-12 Given the reported 26.1% increased incidence of late-stage HNC cancer in the US between 2004-2015, CRT related toxicities pose a significant threat to the health and quality of life of HNC survivors. 13
One such threat is impaired swallowing (dysphagia) which has been reported to occur in 30%-64% of HNC patients treated with non-surgical modalities.14-17 Dysphagia can severely impact hydration, nutrition, pulmonary function, and quality of life.15,18-20 Barring neurological or surgical deficits, Radiation-Induced Fibrosis (RIF) is believed to be the underlying cause of persistent, long-term, post-treatment dysphagia. This is because progressive worsening of fibrosis occludes the swallowing musculature, prevents adequate muscle contraction, and therefore impairs swallowing function.19,21
RIF is thought to occur due to a shift in the normal inflammatory process necessary for proper healing.19,22 It has been suggested that the recurring radiation insult not only causes recurrent inflammation, but also increases reactive oxygen species (ROS) content in tissues. 23 As a result, excessive levels of the pro-inflammatory protein, transforming growth factor-beta 1 (TGFB1) accumulate.22,24,25 This accumulation subsequently triggers the activation of pro-fibrotic mechanisms via activation of myofibroblasts – the primary fibrotic cell type – and production of Connective Tissue Growth factor (CTGF) – the primary signal for inflammation-independent fibrotic processes.19,25,26 Together, these pro-fibrotic factors result in excessive accumulation of extracellular matrix which may cause a range of organ dysfunction severities via stiffening of connective tissue and atrophy of muscles.19,22
The temporal development and extent of RIF is still poorly understood and can vary from person to person. It may occur months or years after RT completion and may present with progressive or spontaneous onset. Barring other medical factors, the severity and extent of the fibrotic process will determine the nature and severity of dysphagia progression.18,19,23 Due to the significant implications of Radiation Induced Dysphagia (RID), various treating clinicians have attempted to employ a range of techniques to proactively (before the onset of dysphagia symptoms) or reactively (after onset of dysphagia symptoms) manage RID. One approach has been to intervene reactively with pharmacologic anti-inflammatory and anti-oxidant factors which act by downregulating pro-inflammatory signals such as TGFB1 and ROSs, which may mitigate any ongoing inflammation contributing to fibrosis.22,27 Unfortunately, while inflammation is necessary for the induction of profibrotic factors, TGFB1-induced production of the profibrotic factor CTGF allows for the progression of fibrosis independently of inflammation.22,28 As a result, the efficacy of these agents would be limited to the pre-fibrotic process only, and they have not been shown to interrupt ongoing fibrosis or reverse established RIF.22,29
One traditional treatment for RID is early referral to Speech Language Pathologists (SLP) who attempt to maintain pre-treatment swallowing function through stretches that preserve range of motion and exercises that strengthen the swallowing musculature.30,31 Depending on institutional protocol, some patients are referred proactively to SLPs during RT in an attempt to mitigate the risk of long-term RID. Alternatively, patients are referred to SLPs reactively once they complain of dysphagia during or after completing RT. Regardless of referral pattern, SLPs typically apply traditional swallowing exercises, but evidence of their efficacy is not strong.32,33 More recently, SLPs have been employing Manual Therapy (MT) techniques as a potential treatment modality that may reduce inflammation and its downstream fibrotic sequelae.
MT has been performed for decades by SLPs administering voice therapy, but its application to dysphagia therapy in the HNC patient population is relatively new. 34 This novel and growing application of MT holds biological plausibility as a proactive or reactive treatment strategy capable of alleviating the adverse effect of RT.35,36 One study found that MT may be considered for frontline or adjuvant treatment of radiation-associated trismus by demonstrating significant improvement in maximum interincisal opening for HNC patients with post-treatment trismus. 37 Furthermore, the addition of MT to a cervical exercise program has shown statistically significant improvement in chronic neck pain patients in both the short and mid-term. 38
A recent national survey of SLPs suggested that MT could be employed during CRT in an attempt to mitigate radiation-induced toxicities without increasing adverse outcomes. 35 While SLPs have begun to employ MT techniques in the HNC population, there are no standardized protocols specific to this population, and it remains unknown what MT techniques are being employed or how they are employed for HNC patients during or after RT. As such, this current study attempted to characterize the types of MT techniques and protocols employed with HNC patients during and after RT.
Methods
Questionnaire Development
An internet-based questionnaire was developed to elucidate the types of MT techniques and the content of MT protocols employed by SLPs at three time points; during RT but before patients develop dysphagia symptoms (proactive, during RT), after RT completion but before patients develop dysphagia symptoms (proactive, post-RT), and after RT completion if patients complain of a dysphagia (reactive, post-RT). Iterative survey pilot testing, discussion, and revision established the content validity of the survey questionnaire. Consensus regarding the content, structure, and wording of the questions was reached after 7 iterations. Face validity of the survey questionnaire was tested using a group of 5 external unaffiliated SLPs. Feedback from these unaffiliated SLPs was incorporated into the survey questionnaire design. The final survey contained 30 questions, with branching logic so respondents only completed questions relevant to their practice.
Questionnaire Content
A complete list of final questions can be found in the Supplemental Material section of this manuscript. Given the lack of published HNC specific MT protocols and unknown comprehensiveness of MT training among SLPs who treat HNC patients, the questionnaire deliberately left MT techniques or protocols largely undefined. This also served to elicit responses that could potentially identify MT techniques perceived by SLPs as useful in this patient population, even if their definitions were different from more established definitions in the osteopathic or physical therapy literature. After a screener question, questions 2-8 focused on relevant respondent demographics. Question 9 asked what anatomic sites are addressed with manual therapy. Questions 10-30 inquired about the time points respondents performed MT on HNC patients; (a) proactively, during RT, (b) proactively, post-RT, and/or (c) reactively, post-RT. Respondents were asked to identify and describe the MT techniques and protocols employed at each selected time point. Techniques were listed in a check-box format with an option to specify therapies that were not listed. Listed techniques included therapies such as laryngeal manipulation, myofascial release, and muscle energy, which were discussed in the literature or anecdotally by clinicians.39-41 Protocols were assessed using both parameter-specific multiple-choice questions and an open-ended question probing the number, formality, and customization of MT techniques applied. The open-ended question was used to capture variables potentially informing the protocols, such as timing around RT, the patient’s medical condition, cancer location, tolerance, and/or patient-clinician goals of the MT intervention.
Study Design/Survey Administration
To allow for confidential and unbiased responses, the survey responses were collected anonymously. Because the research involved an anonymous survey, it was determined to be exempt under 45 CFR 46.101(b) category 2 by the lead institution’s Institutional Review Board, so informed consent was not needed.
The questionnaire was administered using SurveyMonkey® between April 20, 2021, and July 22, 2021. To maximize the response rate, it was sent 6 times over 3 months on different days, different times, and through different listservs. The list servs used included the American Speech Language Hearing Association (ASHA) Special Interest Division 13 listserv, the ASHA Special Interest Division 3 listserv, and the University of Iowa Voiceserv. Special Interest Division 13 includes SLPs with a special interest in swallowing and swallowing disorders, so it would include clinicians who treat HNC patients with MT. The Special Interest Division 3 and the University of Iowa Voiceserv listservs include members with an interest in voice and voice disorders that would include SLPs who use MT for disorders such as muscle tension dysphonia and who may also use such techniques on HNC patients. The three listservs represent a total of approximately 13,500 speech language pathologists SLPs. However, it is likely that a significant proportion of those SLPs subscribed to more than one of those listservs, so the total number of unique SLPs is unknown. As an exploratory survey of a novel and poorly described clinical intervention, the number of respondents was expected to be low, and the results were to be analyzed descriptively. Normally distributed data were calculated with means and standard deviations whereas non-normally distributed data were calculated with medians and interquartile ranges (IQRs).
Results
Of the 64 SLPS who responded to the survey, 95% (61/64) reported performing MT on HNC patients. Of the 61, 17 responses were excluded due to incomplete survey responses which resulted in a 69% (44/64) completion rate.
Respondent Demographics
Respondent Demographics for all Respondents and Across Different MT Treatment Timepoints.

aOne respondent did not answer, n = 43.
bOne respondent did not answer, n = 36.
cOne respondent did not answer, n = 43.
Ninety-one percent (91%; 40/44) reported completing MT Continuing Education (CE) training courses such as Physical Therapist instructed courses (66%), Myofascial Release training (43%), and Upledger (5%). Thirty-four percent (34%; 15/44) reported on the job training and 16% (7/44) reported receiving certification. More than half of respondents (25/44) reported receiving MT training specific to HNC patients.
MT Intervention Time Point Demographics
Of the 44 SLPs, 34% (15/44) perform MT proactively during RT, 84% (37/44) perform MT proactively post-RT, and 100% (44/44) perform MT reactively post-RT. More than half of respondents performing MT at each time point had HNC patient-specific MT training.
Sixty six percent (29/44) of respondents perform MT only post-RT. Of these clinicians, 79% (23/29) use MT both proactively post-RT and reactively post-RT. The remaining 21% (6/29) of this group only perform MT reactively post-RT, once a patient reports dysphagia.
Of the 15 SLPs who perform MT proactively during-RT, 93% (14/15) perform MT both proactively post-RT and reactively post-RT. This demonstrates that almost a third (14/44) of the respondents perform MT on HNC patients regardless of RT timing or onset of RID (Figure 1). Timing of MT application.
The majority of respondents reported having more than 10 years of clinical experience, but less than 5 years of experience employing MT (Figure 2). This trend was consistent across all three time points. All SLPs who perform MT proactively during RT reported having 5 or more years of general clinical experience. Years of general clinical and MT experience reported by SLPs who perform MT by treatment timepoint.
Demographics between SLPs who perform MT at all time points (n = 14) vs only reactively post-RT (n = 6) was also assessed, but no appreciable differences were seen.
Demographics of SLPs Who Perform the Least vs Most MT Sessions per Month
Demographics of the 5 respondents who perform MT the least (≤2 sessions per month) were compared with those of the 5 respondents who perform MT the most (≥25 sessions per month) (see Appendix A). SLPs who conduct the most MT sessions per month were more likely to be employed at an Academic or Specialized Hospital, have had HNC patient specific MT training, and have greater HNC clinical caseloads. Interestingly, neither group appeared more or less likely to perform MT proactively during RT, proactively post-RT, or reactively post-RT (see Appendix A).
Manual Therapy Techniques Employed
Laryngeal manipulation, myofascial release, and massage therapy were the techniques reportedly used by most survey respondents across all three time points (Figure 3). Distribution of MT Techniques used by SLPs by Treatment Time Point.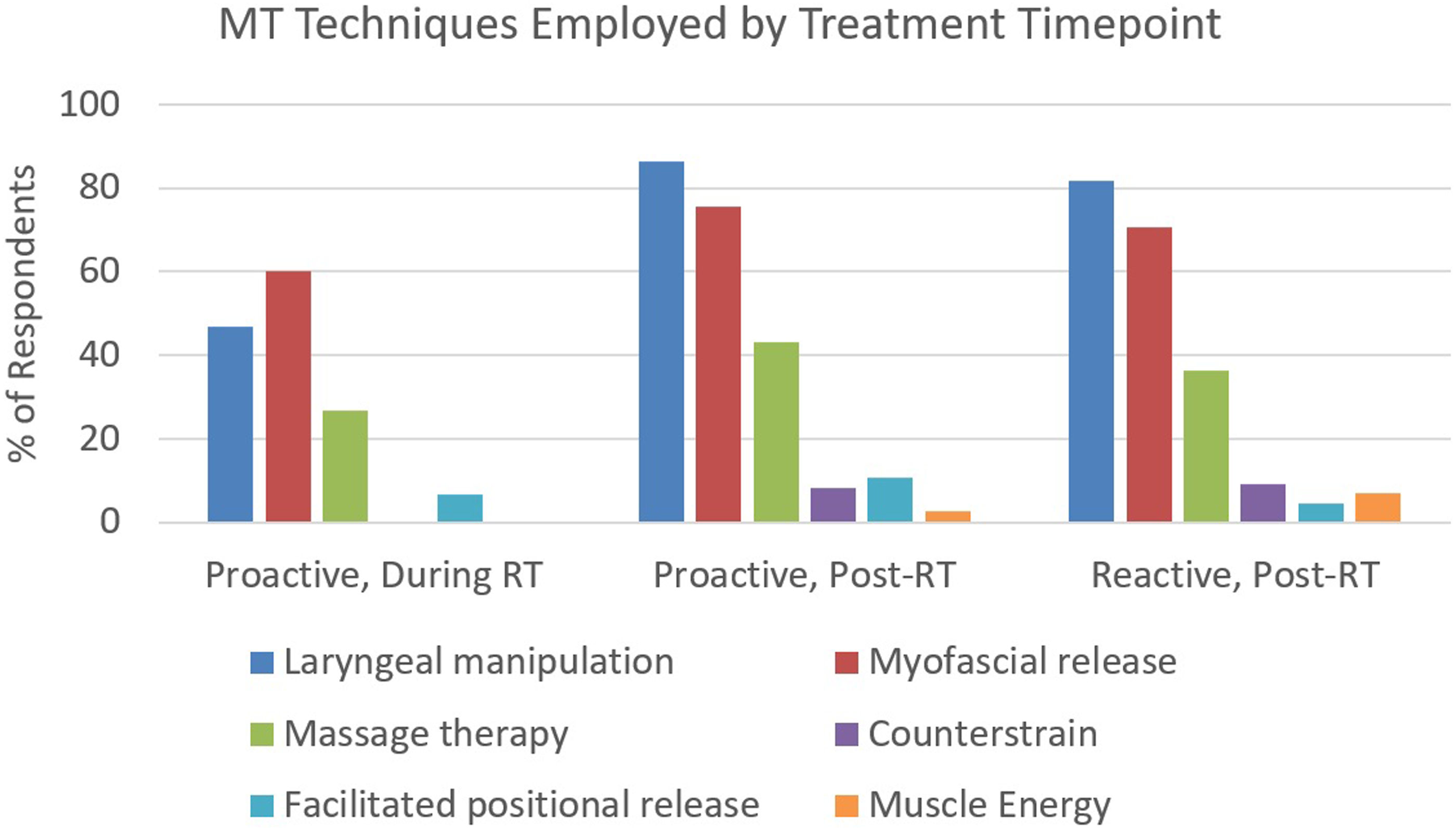
During RT, myofascial release was the technique used by the greatest number of SLPs (60%), followed by laryngeal manipulation (47%). This trend was reversed in the post-RT setting, with laryngeal manipulation becoming the dominant therapeutic technique, followed by myofascial release. SLPs were twice as likely to employ laryngeal manipulation techniques post-RT as compared to during RT (82%-87% vs 47%).
Massage therapy was consistently the third most reported MT technique employed across all time points. While Facilitated Positional Release was employed by a limited number of SLPs across all three time points, Counterstrain and Muscle Energy techniques were only employed in post-RT time points, and only by a few SLPs.
SLPs who perform the greatest number of MT sessions per month were more likely to perform Myofascial Release and Counterstrain techniques as compared to SLPs who perform the lowest number of MT sessions per month. There were no other appreciable differences in the types of MT techniques provided between these two groups.
Manual Therapy Protocols Employed
The majority (66%) of SLPs who perform MT proactively during RT reported seeing patients for MT sessions less than once per week (once or twice per month). In the post-RT setting, 78% of SLPs reported conducting treatment sessions 1-2 times per week (Figure 4). Typical frequency of MT sessions provided to HNC patients (A) and recommended frequency of self-administered MT (B) by treatment timepoint.
Overall, no consistent MT protocols was identified across timepoints. The way in which SLPs incorporated different MT techniques into MT protocols varied between treatment timepoints, between clinicians, and between patients. This is exemplified by Respondent 47 who reported performing a “combination of MFR/manual therapy and laryngeal manipulation — [focusing on] where the patient feels the tightness/stiffness, [without a] set protocol” (Appendix B, Respondent 47). The complete set of protocol descriptions by time point can be found in Appendix B.
Some themes in MT application were identified within intervention time points. SLPs who perform MT proactively during RT provided a noticeably gentler approach that was highly customized to patients when compared to the other time points. However, this customization made it difficult to identify a standard MT protocol used proactively during RT. At this timepoint, SLPs often employ laryngeal manipulation and myofascial release, but do so in a limited, light touch, and patient centered way. The SLPs also reported performing very light stretching and massage therapy. Collectively, the goal was to relieve patient-reported symptoms, release tension/stiffness, and maintain muscle integrity. A good example of this is from respondent #30, who stated… “It depends on the patient’s reaction to radiation. In the first 4 weeks, I do myofascial release on laryngeal, head and neck and shoulder areas to release tension and improve laryngeal movement. After week 4 of radiation, I will teach the patient to do head and neck easy range of motion” (Appendix B).
Although SLPs who perform MT both proactively post-RT and reactively post-RT also reported variation in individual MT protocols, a theme of practice emerged entailed higher frequency, rigor, and pressure with noticeably less customization. During the proactive post-RT time point, treatment sessions consist of a combination of techniques including laryngeal manipulation, myofascial release, stretching, and massage therapy. When MT is applied reactively post-RT, SLPs were more likely to report employing MT techniques that are performed in a manner consistent with formal MT programs, although such application was still often customized and patient-specific. The focus at this point seemed was less about modifying the technique to avoid potential pain, and more about maximizing the effectiveness of each technique. These MT treatment sessions also incorporated traditional dysphagia therapy techniques such as stretches, range of motion maneuvers, and strengthening exercises. Quotes from respondents 34 and 64 are examples of reactive post-RT protocols (Appendix B).
Respondent #34: “When tissue or scar is more stiff or I suspect adhesions, I will be more aggressive – implementing more forceful techniques and other modalities such as kinesiotaping.”
Respondent #64: [I employ a] “custom protocol: combination of laryngeal manipulation, myofascial release, and fascial manipulation. My patients usually have surgery + RT. Usually start with gentle stretches and myofascial release along surgical scar then progress to fascial manipulation.”
Additionally, the majority of SLPs taught patients MT techniques to perform at home. For patients receiving MT proactively during RT, 10/15 SLPs (66%) recommend practicing MT at home at least once per week, with 6 SLPs (42%) recommending practicing MT at home five or more times per week (Figure 4).
For patients receiving MT proactively post-RT, 35/37 SLPs (95%) recommended practicing MT at least once per week at home, and for patients receiving MT proactively post-RT, 41/44 SLPs (93%) recommend the same. Across time points, SLPs generally recommended a high rate of self-administering MT at home (>5 times per week).
The MT techniques taught to patients to perform at home varied in complexity depending on the time of intervention. Patients who are actively undergoing RT are taught simple, gentle techniques such as stretches, manipulation, and/or self-massage techniques to prevent fibrosis and tissue stiffness. The intensity and complexity of techniques taught to patients are greater at the post-RT timepoints. SLPs reported a hands over hands approach to train patients and/or significant others how to perform stretches, massage therapies, or myofascial release techniques. During the reactive, post-RT time point, techniques taught, including laryngeal manipulation and swallowing exercises, were more technical compared to the techniques taught at other time points.
Discussion
A previous study reported that MT is used during and after RT to proactively prevent and reactively treat RID in HNC patients, with similar reported rates of adverse effects between HNC patients and non-HNC patients receiving MT. 35 However, it remained unknown what techniques and protocols are used on HNC patients during or after RT. This current study revealed that SLPs often employ a combination of MT techniques, specifically laryngeal manipulation, myofascial release, and massage therapy. Additional techniques were used, albeit less frequently and often post-RT, including facilitated positional release, counterstrain, and muscle energy. When comparing the during RT and post-RT treatment timepoints, there were differences in treatment session frequency, home program recommendation, and self-administered MT patient education. The choice of when to perform MT on HNC patients did not vary by SLP demographics such as experience or training, suggesting that this choice is likely a function of professional opinion or institutional culture.
The SLPs who completed this survey were mostly experienced; 70% had 10 or more years of experience. However, approximately half of the SLPs reported having less than 5 years of experience performing MT. This finding suggests that experienced SLPs who perform MT on HNC patients incorporate MT later in their careers, possibly to add another therapeutic option to treat RIF and dysphagia. One reason for this may be that traditional therapy for dysphagia in HNC patients has limited efficacy.30-32 In this scenario, it would make sense that SLPs who have been practicing for many years, and who have experienced the limitations with current standard therapy, would seek new and promising therapeutic approaches to help their patients. Interestingly, almost half of SLPs who perform MT on HNC patients were employed at academic teaching hospitals. However, this finding may be superficially elevated due to the volume of HNC patients at academic hospitals. Our study found that 63% of SLPs who perform >9 MT sessions per month (n = 19) were from academic hospitals as opposed to the 28% of SLPs who perform <9 MT sessions per month (n = 25). A larger HNC population may dictate the need to try something as novel as MT.
While the majority of SLPs reported performing MT post- RT (proactively (89%), and reactively (100%), it is notable that a third of respondents reported performing MT proactively during RT. This seems significant given that this practice is not well established. Application of MT during RT suggests that a considerable proportion of SLPs feel that MT has the potential to mitigate the pro-inflammatory and pro-fibrotic effects of RT, and that this therapy can be applied safely at this time point. In contrast, 13% of surveyed SLPs reported only performing MT post-RT in reaction to the onset of dysphagia symptoms, suggesting that most SLPs may view MT as most effective when applied proactively. These findings cumulatively suggest that some SLPs (or their institutions) may acknowledge the benefit of proactive MT while remaining uncertain of its safety during RT. The lack of formal phase 2/3 clinical trials for proactive MT’s safety and efficacy during RT, combined with SLPs’ varied adherence to protocols — from “No adherence to protocol,” (Appendix B, Respondent #2), to “[Performing] only the techniques [they were] taught,” (Appendix B, Respondent #11) — highlights a lack of standardization. This absence of standardization, along with insufficient safety and efficacy data, necessitates the development and testing of a standardized MT protocol for HNC patients via an RCT to ensure safety and universal therapeutic benefit.
The assessment of demographics between the SLPs who perform MT on HNC patients proactively during RT, proactively post-RT, and reactively post-RT yielded no appreciable differences. Similar proportions of SLPs received HNC-specific MT training irrespective of the time point the SLPs chose to implement MT in clinical practice. The HNC clinical caseloads, SLP experience (both clinically and with provision of MT), and the number of MT sessions performed per month were also similar across SLPs performing MT at different timepoints. Since no differences were observed between clinicians who perform MT at different timepoints, the decision to perform MT at a specific time point is likely not a matter of experience or training, but a matter of opinion or institutional allowance to perform the intervention.
There were notable differences in the application of MT techniques and protocols between different timepoints SLPs providing MT proactively during RT focused on relieving patient-reported symptoms, releasing tension/stiffness, and maintaining muscle integrity amidst a reported absence of established MT protocols. Currently, the frequency and intensity of MT necessary to appreciably mitigate the inflammatory factors leading to fibrosis is unknown. This lack of an evidence-based consensus is highlighted in the home program responses (Figure 3). During RT, SLPs seem to be split between providing no home program and an aggressive 6-7 day per week program. It is possible that some SLPs are worried about “over doing it” while others feel that patients need to perform MT almost every day to affect inflammation and downstream fibrosis.
SLPs providing MT at post-RT timepoints also reported varied protocol application, but were less concerned about pain and more concerned about maximizing the effects of the MT intervention. While laryngeal manipulation, myofascial release, and massage therapy were the main modalities used across all time points, the frequency and intensity of application was higher post-RT. If the goal of MT application is to prevent a switch from a normal to abnormal wound healing process through reduction in peak inflammation, then it is possible that any post-RT MT performed on dysphagic patients who are already fibrotic is largely ineffective. Reactive MT may, however, release adhesions and loosen connective tissues, which, if applied consistently, may improve swallow function even if it does not reverse fibrosis or the autocrine fibroproliferative process. One study is currently testing safety and preliminary efficacy of a post-RT MT program on a cohort of 24 patients who are at least 2 years post-RT and present with moderate RID. The results of this study are highly anticipated. 36
This study is not without limitations. While an interdisciplinary team of researchers, students, ENTs, and SLPs aided in the design of the survey, they are not an expert panel of MT practitioners. An expert panel of SLPs and PTs who provide MT to dysphagic patients may have altered the composition or content of the survey. Accordingly, interpretation of MT techniques and protocols may be limited by language that may not perfectly align with language from osteopathic and PT disciplines. The survey did not evaluate patient demand or SLPs availability as they relate to frequency of MT provision, so it remains unknown if low frequency MT providers were constrained by clinical environment or patient need. Additionally, open-ended questions about protocols could have required a minimum word count from respondents to encourage SLPs to provide more in-depth descriptions, although this may have increased the risk of respondent drop-out.
Another limitation is the unknown response rate. Despite the survey being distributed through multiple subscription listservs specifically targeting SLPs, the presence of overlapping membership among these services hinders an accurate estimation of the true number of SLPs reached. Furthermore, because this is a novel application of MT that lacks standardized training and documentation of service delivery, the true population of SLPs who employ this technique, or where they work, is unknown. As a result, sampling bias, non-response bias, and limited representation of the true population are possible limitations of this study.
Future directions should include at least two critical tasks. The first is to establish common language and terminology for MT techniques and protocols. Flock & King attempted to do this for MT techniques used in voice therapy, but their results were limited by studies published by teams with their own MT language. 42 Future research should include qualitative interviews and/or application of Delphi methodology with a diverse group of clinician and trainer stakeholders. These stakeholders, who should be experts and who should broadly represent both MT providers and MT trainers, should come to consensus regarding terminology used to describe MT techniques and to propose mutually agreed upon protocols. This would establish a baseline language that can be employed across future studies and between MT practitioners. The second critical task, after completion of the first, would be to develop and execute a phase 2/3 RCT that measures the potential efficacy of MT in the HNC patient population, ideally at each of the 3 possible treatment timepoints.
Conclusion
Laryngeal manipulation, myofascial release, massage therapy, facilitated positional release, counterstrain, and muscle energy techniques were used to treat dysphagia in HNC patients. While MT was typically applied gently during RT and more aggressively post-RT, the application of these techniques was not standardized and was highly customized to the patient. Customization is important when considering patient variables such as patient tolerance/feedback, cancer location, timing of cancer treatment, and type of cancer treatment. However, the complete lack of standardization can also be detrimental in that different clinicians could treat identical patients in very different ways, which would hinder consistent and optimal therapeutic effect across patients. It also makes measuring treatment efficacy exceptionally difficult. Given the prevalence of RID and its impact on the HNC patient livelihood, the novel utilization of MT as a proactive and reactive technique to prevent and/or alleviate RID is understandably one of clinical interest. A semi-standardized protocol that allows for patient customization should be collaboratively developed and tested with a properly designed and powered phase 2/3 clinical trial.
Supplemental Material
Supplemental Material - A Survey of Manual Therapy Techniques and Protocols Used to Prevent or Treat Dysphagia in Head and Neck Cancer Patients During and after Radiation Therapy
Supplemental Material for A Survey of Manual Therapy Techniques and Protocols Used to Prevent or Treat Dysphagia in Head and Neck Cancer Patients During and after Radiation Therapy by Kadesh Daniels, Anindita Chanda, Lucas Berry, Arpita Edke, Parth Patel, Andy Wun, and Gintas P. Krisciunas in Global Advances in Integrative Medicine and Health.
Supplemental Material
Supplemental Material - A Survey of Manual Therapy Techniques and Protocols Used to Prevent or Treat Dysphagia in Head and Neck Cancer Patients During and after Radiation Therapy
Supplemental Material for A Survey of Manual Therapy Techniques and Protocols Used to Prevent or Treat Dysphagia in Head and Neck Cancer Patients During and after Radiation Therapy by Kadesh Daniels, Anindita Chanda, Lucas Berry, Arpita Edke, Parth Patel, Andy Wun, and Gintas P. Krisciunas in Global Advances in Integrative Medicine and Health.
Supplemental Material
Supplemental Material - A Survey of Manual Therapy Techniques and Protocols Used to Prevent or Treat Dysphagia in Head and Neck Cancer Patients During and after Radiation Therapy
Supplemental Material for A Survey of Manual Therapy Techniques and Protocols Used to Prevent or Treat Dysphagia in Head and Neck Cancer Patients During and after Radiation Therapy by Kadesh Daniels, Anindita Chanda, Lucas Berry, Arpita Edke, Parth Patel, Andy Wun, and Gintas P. Krisciunas in Global Advances in Integrative Medicine and Health.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.