
Abstract
Opportunities exist to improve patient experience in the emergency department for low-risk (ie, non-cardiac) chest pain patients with anxiety and panic as the underlying cause of symptoms. Referral to internet-based cognitive behavioral therapy (iCBT) with guided support is a scalable, evidence-based option that is underused, particularly among non-white patients. In collaboration with a diverse group of patient and community partners, we co-developed and tested an existing iCBT course for generalized anxiety disorder with delivery of guided support by a peer recovery specialist with concordant lived experience. We analyzed patient partner feedback from debriefing sessions during the testing phase using conventional content analysis. Results revealed overall positive experiences with both iCBT lessons and peer support calls. Key points derived from qualitative findings include: (1) iCBT lesson content resonated reasonably well with the diverse group of patient partners, (2) the peer relationship was key to individualizing application of content to various lived experiences, and (3) the guided discussion should be participant-driven and based on content that resonates most with the participant. In conclusion, iCBT with guided peer support was acceptable to patient partners involved in co-development and testing who were representative of a diverse patient population.
Introduction
There is a hidden population of patients with undiagnosed or under-treated common mental health problems including anxiety and depression who present to the emergency department (ED) for the evaluation of chest pain and related symptoms. While chest pain is the second most common reason for visits to the ED, 1 only 20% of all chest pain patients have a true cardiac cause of symptoms and approximately 40% have anxiety and panic as the underlying cause.2,3
Historically, care in the ED ends with discharge upon ruling out a cardiac or other life-threatening event leaving patients confused about the cause and management of their ongoing symptoms. 4 The missed opportunity to evaluate and treat anxiety disorders not only contributes to poor patient experience of care, but also a futile cycle of repeated ED visits of little benefit to the patient with an $1.8 billion dollar annual pricetag. 5 From the patient perspective, anxiety symptoms can be debilitating and should be taken more seriously in the ED setting. 6 Indeed, anxiety and depression are among the most disabling conditions in the US exceeding all other medical conditions in terms of years lived with disability. 7 Furthermore, communities of color are likely disproportionately represented in the low-risk (ie, non-cardiac) chest pain population with anxiety (LRCP-A) who seek care in urban EDs.8-10
Highly scalable, cost-effective, and evidence-based interventions that could be implemented in the LRCP-A population exist. Self-administered, internet-based cognitive behavioral therapy (iCBT) is an effective form of CBT,11-13 for anxiety and depression with treatment effects enhanced by guided support 14 and comparable to traditional face-to-face therapy. 15 However, iCBT is underused and particularly among non-white populations. 16
The objective for co-development and testing of an iCBT course with guided peer support for generalized anxiety disorder was to assess initial acceptability of the intervention during the research planning phase in preparation for its inclusion in a subsequent comparative effectiveness research study, the Patient-Centered Treatment of Anxiety after Low-Risk Chest Pain in the Emergency Room (PACER), that is currently being conducted. 17
Methods
Stakeholder engagement for research planning and conduct phases of the PACER Study includes a Patient and Community Advisory Committee (PAC). During the planning phase, they provided input into the selection of iCBT as one of three comparators for the study as well as the decision to use peers for delivery of the guided support component. Because the latter was a relatively new approach, a decision was made to test the coupling of guided peer support with iCBT. Six patient partners volunteered to participate in the intervention and provide feedback on their participation. In addition, community members of the PAC representing mental health advocacy organizations with expertise in peer support developed and delivered the guided peer support component during the initial testing.
All members of the PAC including those who volunteered to test the intervention were recruited from the target ED population with low-risk chest pain and moderate to high symptoms of anxiety. Of the six who tested the intervention, the majority of patient partners (hereto referred to as partners) were Black Americans (5/6), male (4/6) with an even distribution of age from 19 to 34 (2/6), 35 to 49 (2/6), 50 or above (2/6) and income below (2/6), at (2/6), or above (2/6) sufficiency. Income sufficiency was self-reported in response to the question, “When you consider your household income from all sources, (today), would you say that you are comfortable, have just enough to make ends meet, or do Not have enough to make ends meet.” 18
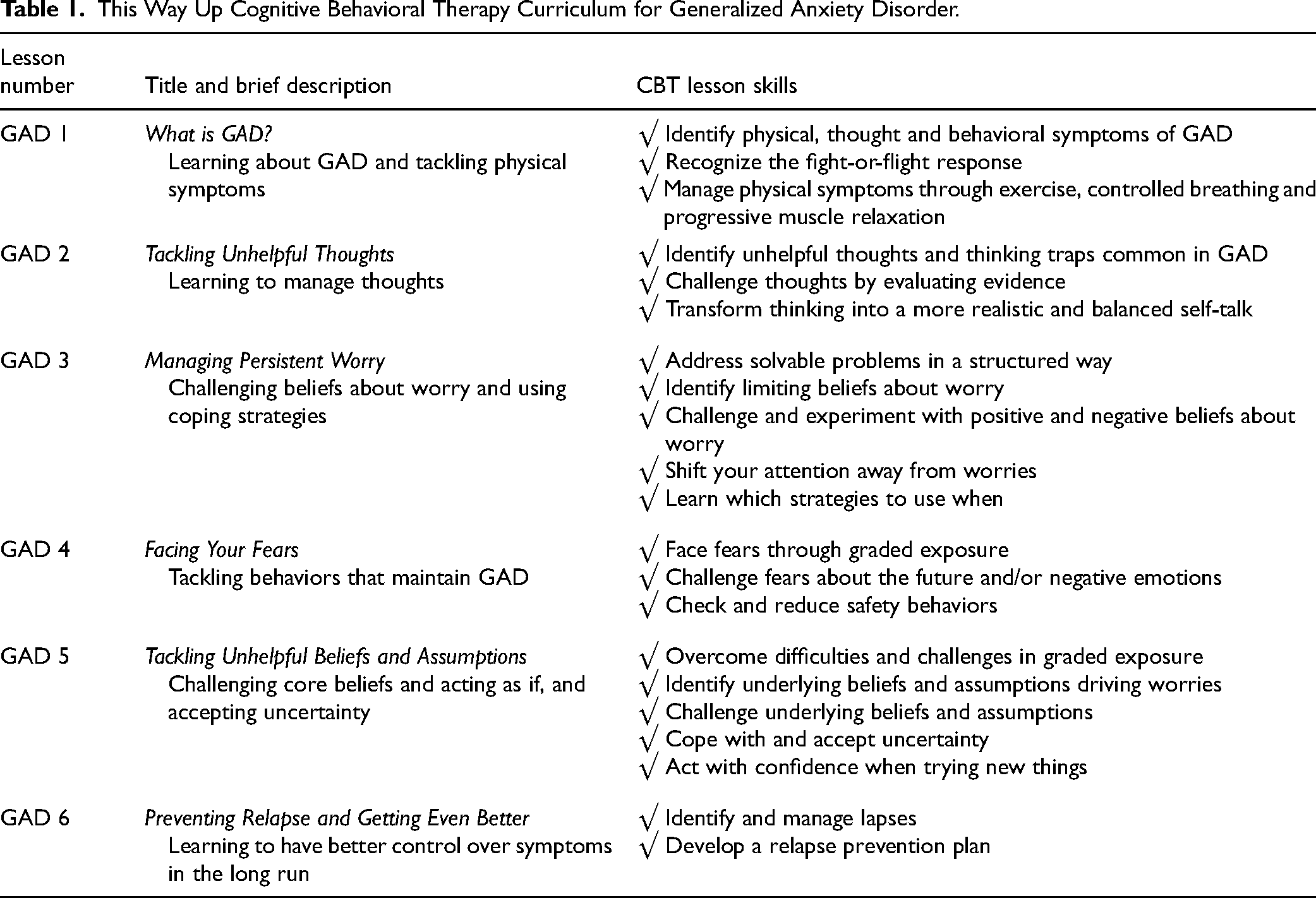
The first component of the intervention was an evidence-based online course for generalized anxiety disorder (GAD) called This Way Up (TWU) developed for use in Australia.19,20 The content of the six GAD lessons is shown in Table 1. The online content featured character stories about experiences of anxiety and its management. Users could download comprehensive PDF lesson summaries with exercises and worksheets to complete. Each lesson summary concluded with an action plan of CBT skills recommended for practice. The guided peer support component included video calls with a certified peer recovery specialist (hereto referred to as peer) with lived experience of anxiety and symptom management. The structure for guided support was based on a national peer support model and consisted of a check-in to share current experience of anxiety, discussion to apply the information learned in the lesson and closing on a positive note with encouragement to practice at least one new skill from the action plan.
This Way Up Cognitive Behavioral Therapy Curriculum for Generalized Anxiety Disorder.
During testing of the intervention, the partners joined a weekly virtual debriefing session to offer feedback on their experience with the TWU lesson and peer call. Examples of questions they were asked included, “What did you think of this lesson?,” “How was the information helpful?,” “What was the peer call like?,” and “Is there anything you would change about the lesson, peer call, or processes in general to make participation easier or more beneficial?”
Audio recordings from debriefing sessions were transcribed and analyzed using conventional content analysis. 21 Remarks about the partners' experiences with the two components of the intervention and their recommendations for changes were coded with the phrase that captured the essence of the remark. Each transcript was coded independently by a team member and verified for accuracy by a second team member. Codes were organized in a data display table according to experiences with the TWU lessons and the peer support calls. Similar codes were grouped into categories by team member dyads and finalized by team consensus.
Results
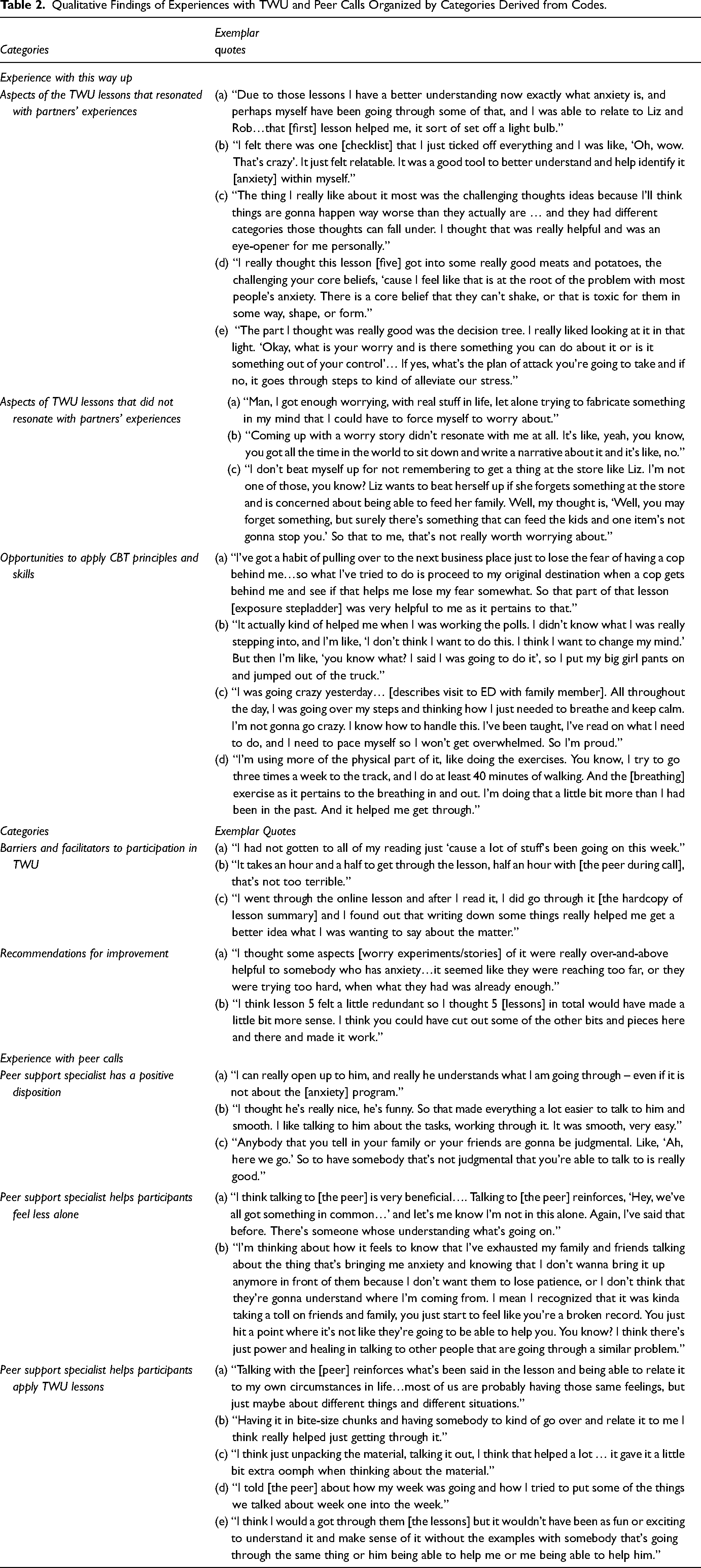
Overall, the partners described positive experiences with both TWU lessons and the peer support calls. Their discussions of TWU lessons focused on (a) aspects of the lesson that did or did not resonate, (b) how CBT principles and skills were applied, (c) barriers and facilitators to participating in the lessons, and (d) recommendations for improvement. During their discussion of the peer support calls, partners described (a) the peer's positive disposition, (b) how he helped them feel less alone, and (c) how he helped them apply the TWU lessons. Table 2 highlights narrative summaries and exemplar quotes for each category.
Qualitative Findings of Experiences with TWU and Peer Calls Organized by Categories Derived from Codes.
TWU Lessons
The partners' narratives revealed that the majority of lesson content was helpful and described as easy to understand or relatable and therefore resonated with their own experiences of anxiety. However, at least one partner stated that some character scenarios did not relate to their own experience of anxiety and several partners identified a few topics that were less easy to understand or apply. For example, while content related to thought challenging was helpful to most partners, topics related to imaginative exposure, including writing worry stories and conducting worry experiments, was not.
The partners reported applying CBT principles and skills to a variety of real-life experiences. They described how they applied skills to lessen anxiety when driving, working at election polls, confronting health issues, and addressing other chaotic or stressful life events.
Most of the barriers were related to their own situations that could potentially decrease participation including feeling burdened by life events, being tired from work, procrastination, and low motivation. Facilitators were related to ways they found to engage productively with the course materials and included having a hard copy of lesson materials, taking notes, pacing participation, and reviewing the materials between lessons to retain more information.
Partners were satisfied with the TWU course and had only a few recommendations for improvement that included omitting content that did not resonate with all or most partners, reducing the number of total lessons, and being able to watch rather than read character scenarios on their phone.
Peer Support Calls
Partners indicated they appreciated the approachable disposition of the peer. They described the peer as “nice,” “understanding,” and “non-judgmental.” They felt because he had experienced similar struggles, he “truly” understood their experiences of anxiety and made them feel less alone. As a result, the partners felt he was easy to talk to and comforting.
All partners indicated the peer helped them apply the lessons from TWU to their own personal experiences. The peer helped them “unpack” the material, talk it through, and apply it. Furthermore, all partners agreed that they would not likely have completed the TWU lessons without the guidance of the peer.
Discussion
Overall, the content provided in the TWU lessons resonated reasonably well with this diverse group of patient partners and was applicable to a variety of lived experiences with anxiety. The peer relationship was key in individualizing application of TWU content to diverse partners' experiences. This may be of particular importance among individuals with a history of poor experiences of care and/or mistrust in healthcare delivery systems. Finally, there was some variation in aspects of the TWU lessons that resonated among partners. Hence, the guided discussion should be participant-driven and based on content that resonates most with the participant rather than peer-driven or a comprehensive review of all lesson content.
Findings from co-development and testing of the iCBT with guided peer support intervention was focused on developing a novel intervention for the PACER study and is aligned with emerging research. 22 The PACER study is currently being conducted to test the effectiveness of integrating the intervention into the ED workflow. 17 It is anticipated that results of the PACER study will be used to both inform clinical guidelines and practice improvement for low-risk chest pain patients with anxiety in the ED setting and population.
Limitations
Our findings are limited by a small sample of patient partners participating in the co-development and testing of the intervention during the research planning phase. The sample size did not allow for data saturation and thus the findings do not yield an exhaustive description of patient partner experiences with the intervention. Moreover, findings may not be generalized to LRCP-A populations more broadly. Nonetheless, the patient partners provided ample information on the acceptability of the intervention to justify its inclusion in a subsequent trial.
In addition, we did not include a control or comparison group in the initial testing. We also relied solely on self-reported qualitative data during initial testing. While the volunteer nature of patient partners may have skewed the results toward more positive findings, the research team felt the partners were invested in the testing process and provided feedback that was candid. However, increased sample sizes, use of comparison groups, more robust quantitative measures for clinical symptoms of anxiety, and randomization of research participants are being used in the larger PACER trial currently testing the intervention. 17
Conclusion
Internet-based cognitive behavioral therapy with guided support delivered by peers was acceptable to patient partners involved in co-development and testing who were representative of a diverse patient population.
Footnotes
Acknowledgments
We acknowledge the contributions of all patient partners who participated in the planning phase of research, and in particular members of the Patient and Community Advisory Committee who participated in preliminary testing of the iCBT with guided peer support intervention including Latoya Snorten, Andrew Butler, Veronika Clay, Alex Prittie, and Marshall Conley.
Authors’ Contributions
JNC, NK, EM, JH, MM, KK, and PM made substantial contributions to the conception and design of the work. JNC and PM were awarded funding to support the work. JNC, KP, CD, and JE contributed to the analysis of data and JNC, KP, CD, JE, and CM contributed to the interpretation of data for the work. All authors contributed to drafting the work, providing critical revisions for important intellectual content, and assume accountability for accuracy and integrity for the work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
A determination of not human subjects research was made by the Indiana University Institutional Review Board on 09-22-2020, IRB#2009857215.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the Indiana University's Racial Justice Research Fund.
Informed Consent Statement
Informed consent to participate in providing feedback as an engagement activity was not obtained because of the non-human subjects research determination. Verbal consent for publication was obtained from all patient partners to share de-identified exemplar quotes to accompany aggregate feedback.