
Abstract
Background
In the face of significant distress among physicians, access to counseling is critical.
Objective
An on-site wellness program for physicians-in-training and faculty was assessed by examining (a) were participants representative of those eligible for services and (b) demographic and trainee vs. faculty differences in burnout, distress, suicide risk, and presenting concerns of participants who utilized services.
Methods
From 2013–2018, 73% (N = 468; 316 residents/fellows, 152 faculty) of individuals seeking services also consented to research. At intake, participants completed a distress measure (ACORN) and two items from the Maslach Burnout Inventory (MBI), and clinicians categorized presenting concerns and suicide risk. Using Chi-square analyses, participants’ characteristics were compared to physicians eligible for treatment. The association between demographics, faculty vs. trainee status, specialty, and distress, burnout, suicide risk, and presenting concerns was evaluated with ANOVAs and logistic regressions.
Results
Women, trainees, and primary care physicians were more likely to access services. On the ACORN, 63% were in the clinical range (M =1.7, SD =0.6). On the MBI, 36% scored in the clinical range. Clinicians rated 9% of participants with suicide risk. Neither gender, racial/ethnic minority status, nor specialty were associated with distress, burnout or suicide risk. Trainees reported greater distress than faculty (F (1,447) = 8.42, P = .004,
Conclusions
Two physician groups which often report higher levels of burnout and distress when surveyed, women physicians and residents/fellows, were the most likely to get professional help in an on-site wellness program. Physician wellness programs need to be prepared to address work and personal stressors and different levels of distress and risk.
Burnout, depression and suicide risk during medical training and practice are leading to national efforts 1 to protect the well-being of physicians.2,3 Although burnout is described as an occupational hazard and best addressed with organizational level interventions, 4 responding to clinical levels of depression, anxiety and suicidal ideation requires individual resources.5,6 Significant barriers to treatment are often reported by medical trainees and physicians including concerns about confidentiality, fears of disclosure to licensing or credentialing boards, cost, limited protected time for personal health care, stigma, a culture of self-reliance, and doubts about helpfulness of counseling to address physician distress.7–9 Recognizing this unmet need, the Accreditation Council for Graduate Medical Education (ACGME) in 2017 began requiring all residency and fellowship programs to offer “accessible, affordable, comprehensive mental health treatment.” 10 Faculty well-being is critical to patient care and trainee education– highlighting the need to also offer resources to faculty.11,12 As graduate medical education and health care leaders make decisions about funding wellness services for their residents and faculty, it is important to consider what models of care are actually utilized by this population, who seeks treatment and why.13,14
Research is limited on which model of care is most likely to be accessed by medical trainees and physicians.15,16 Physician wellness programs vary by location (on-site vs. community), duration (limited sessions vs. continuity of care), funding source, clinician expertise in treating physicians, independence from a trainee evaluative role, and scope of services available.14,17,18 Residents express concern about seeking medical or mental health services in their home institution if their treating clinician could be a current or future colleague. 19 Employee Assistance Plans (EAPs) in which all employees are eligible for a limited number of sessions with a contracted counselor in the community are typically underutilized by physicians. 20 Medical trainees may have difficulty finding community providers with flexible hours to accommodate their residency schedule and are less likely to afford co-pays/deductibles. A troubling number of distressed physicians may self-medicate, ask colleagues to write prescriptions for medications, or go without professional services. 9 Lack of access to comprehensive treatment is cited as a factor in the high suicide rate among physicians.9,21
The Resident and Faculty Wellness Program (RFWP) at Oregon Health and Science University (OHSU) was established in 2004 to promote help-seeking by offering free, unlimited, confidential counseling, coaching, and psychiatric services on-site at a midsize US academic medical center (AMC). RFWP clinicians actively attempt to reduce barriers by increasing awareness about the program, providing education on our confidentiality policies (e.g., no documentation in the hospital’s electronic medical record, no reporting this treatment on licensing or credentialing applications), offering ease of scheduling, and promoting help seeking as essential to professionalism. We previously reported that RFWP is highly utilized among trainees (up to 38%) and faculty (up to 7%) and that the majority of trainees surveyed would seek services if needed.22–24
Few studies exist that examine whether physicians who receive care from on-site wellness programs such as RFWP are representative of their larger cohort or what groups might be experiencing higher level of distress or suicide risk at time of intake. 14 This type of information about level of need and treatment concerns is vital to design a comprehensive treatment model, orient mental health professionals to care for this population, and create outreach efforts that encourage all distressed physicians to seek help. Programming and messaging about wellness services may need to consider possible demographic, clinical specialty, and training status differences in presenting concerns, levels of distress and openness to seeking professional care. Burned out residents, for example, are more concerned about asking their attending to step away from service for a personal health appointment including counseling. 25
Gender, ethnicity/race, and trainee vs. faculty status may be associated with differences in accessing professional care. In community and undergraduate populations, women and white (non-Latinx) individuals are more likely to seek or be referred for counseling or psychiatric treatment.26,27 Women medical trainees report two times higher rates of depressive symptoms 28 and face unique residency stressors such as higher rates of discrimination and harassment during training.29,30 Non-white medical students are more likely to report their race negatively impacted their medical education experience and increased their sense of isolation. 31 Across a number of clinical specialties, higher levels of burnout and distress are evident among medical residents and fellows than faculty physicians5,6—suggesting potentially greater need for and utilization of supportive services by trainees. Trainees may present with different concerns than faculty and require different types of interventions.
In the present study, we examine five years of RFWP intake sessions to (a) assess whether participants were representative of all physicians eligible for services, (b) identify demographic, trainee vs. faculty, and clinical specialty differences in levels of burnout, distress and suicide risk of participants who utilized services, and (c) explore demographic and trainee vs. faculty differences in the types of presenting concerns at intake. In addition, given higher rates of suicide among trainees nationally during the months of July-September and January-March, 21 program utilization was assessed for seasonal differences by trainees and faculty.
Methods
In 2013, the RFWP launched a program evaluation with Oregon Health and Science University IRB approval. From 2013-2018, 637 individuals (445 residents/fellows and 192 faculty) accessed treatment in the RFWP and 73% (n = 468, comprised of 316 residents/fellows and 152 faculty) of individuals consented to participation in research. Results of logistic regressions indicated individuals who agreed to participate in the research did not differ significantly from the nonparticipants by gender, age, race/ethnicity, referral source, being clinically distressed on ACORN, burnout items, or clinician ratings of suicide risk. Trainees were slightly less likely to participate in research than faculty (OR = 0.645, 95%CI = .430–.966) and the reason for this difference is unknown but anecdotally trainees expressed more confidentiality concerns. De-identified institutional data on descriptive statistics of all faculty and trainees for each of these five academic years was obtained. Due to the anonymous nature of the institutional data, we were unable to collapse the full AMC population data across years and any examination of these data had to be done for each year separately. The average AMC population across the five years was 2443 physicians.
Categorization of Descriptive Variables
We examined four descriptive factors: gender, race/ethnicity, faculty vs. trainee status, and clinical specialty. Gender was assessed as a dichotomous measure (male/female). Due to low rates of multiple racial/ethnic groups, race/ethnicity was measured as white/non-Hispanic vs. other. Status at the institution was dichotomized as faculty vs. trainee. Five broad categories were created based on clinical specialty: hospital-based (e.g., anesthesia, radiology, pathology, psychiatry, emergency medicine), medical/pediatric specialties, primary care (pediatrics, internal medicine, and family medicine), surgical, and other/PhD. These broad categories were intended to prevent identification of individuals in smaller training programs and group them in a way that captured similarities in the setting and/or scope of their work.
Measures of Distress, Burnout, Suicide Risk
At initial intake, participants reported on various psychological symptoms over a two-week period on a scale of 0 (“rarely”) to 4 (“very often”) using the well-validated A Collaborative Outcome Resource Network Adult Version 11 (ACORN). 32 A summary score of ten items, the Global Distress Scale (GDS), is generated; the three substance use items are intended to be screening items for substance abuse and are evaluated separately. A mean GDS score of 1.5 or greater is in the clinical range. 32 For the present study, the ACORN demonstrated good internal reliability, α = .846.
Participants also rated their levels of Emotional Exhaustion (EE) and Depersonalization (DP) as measured by two Maslach Burnout Inventory (MBI) items found to be predictive of the overall scale. 33 MBI scores were dichotomized such that participants were considered in the clinical range for burnout if they scored 5 or higher on either scale. 33
Clinician rating of suicide and other risk (any indications of impairment, domestic violence, violence towards others) was also obtained during the intake interview, along with source of referral to the RFWP (self-referred vs. other). Clinicians based their ratings of suicide risk and other risk on participants’ responses in the clinical interview and on related items on the ACORN (e.g., “thoughts of harming myself”).
Coding of Presenting Concerns
Qualitative data of participants’ presenting concerns reported in the intake interview were coded by two of the study authors using an iterative qualitative review. First, the authors created categories of presenting concerns based on their clinical experience with the RFWP participants. They then pilot coded 50 sets of intake notes, resolved areas of disagreement, and modified the coding categories, arriving at 9 categories of presenting concerns hierarchical grouped into work-related and nonwork-related topics (Table 3). At this point, the authors each coded half of the intake notes; for each category, coders indicated if it was a presenting concern for the individual (0 = no, 1 = yes), thus providing quantitative data as well. Forty sets of intake notes were randomly selected for double-coding to examine interrater reliability. Using the thresholds suggested by Landis and Koch, 34 levels of agreement for all categories were fair or better (Cohen’s κ range = .343-.688, all but one value fell in the moderate to substantial agreement ranges). Due to concerns of prevalence issues, which can unduly influence κ values, we also examined percent agreement, which ranged from 75–100%. Interrater agreement for the summed superordinate work- and nonwork-related concerns was also in the acceptable range (single-measures absolute-agreement ICCs = .56–.58). 35
Data Analysis
Analyses were conducted using SPSS Statistics for Windows Version 25.0 (IBM Corp, Armonk, NY). To examine the representativeness of the RFWP participants to all physicians eligible for services, we used Pearson’s chi-square tests to compare annual institutional descriptive data on the entire cohort of medical trainees and faculty to that of the RFWP participants in each specific academic year. Due to confidentiality of and likely redundancy across the five academic years of the institutional cohort and RFWP participants, we were unable to run one comparison that combined five years of data for each group. Separate analyses were conducted for each of the four descriptive factors (e.g., gender, race/ethnicity, trainee vs. faculty and clinical specialty). For the only non-dichotomous variable, clinical specialty, Bonferroni-corrected post hoc comparisons were planned and significant omnibus tests performed.
Means, standard deviations on the ACORN and MBI, frequencies in the clinical range on the ACORN and clinician ratings of suicide or other risk were conducted. Independent samples t-tests were conducted to compare endorsement of individual ACORN items between faculty and trainees. Based on the differences noted between this AMC population and the RFWP sample, we tested the relationship between distress and four individual characteristics including gender, ethnic/racial identity, faculty vs. trainee status, and clinical specialty. Each relationship was tested using a univariate ANOVA with GDS score from the ACORN as the dependent variable. Logistic regression was used to test whether any of the descriptive factors were significantly associated with the dichotomous outcomes of clinical levels of burnout or suicide risk. Frequencies of presenting concerns were provided and logistic regression was used to test whether any of the descriptive factors were significantly associated with each of the specific presenting concerns, as well as overall number of work- and nonwork-related concerns. Finally, RFWP utilization by time of academic year was examined using Pearson’s chi-square tests to examine if rates of intake sessions differed based on time of year (divided into quarters).
Results
Representativeness of RFWP Participants to AMC Population
Compared to all eligible physicians, individuals engaging with the RFWP were more likely to be female (results were consistent across the five years, ranging from χ6+(1)s = 4.12–12.08, Ps = .042–.001, specific findings by year available in Supplemental Materials). The RFWP sample was not significantly different in terms of race/ethnicity for any year (χ2(1)s = .10–1.50, Ps = .221–.751). The RFWP sample was on average 33.9% less likely to be faculty (vs. trainee) than the AMC population and this difference was significant for all years (χ2(1)s = 33.26–80.74, Ps < .001). Significant differences in RFWP utilization were observed based on clinical specialty at each year (ps < .001). Bonferroni-corrected post hoc comparisons indicated that for all years, compared to the AMC physician population, RFWP participants were significantly more likely to be primary care physicians and less likely to be from the other/PhD. Comparisons between hospital-based, medical/pediatric or surgical specialties were not significant.
Distress, Burnout, and Suicide Risk in RFWP Participants
Table 1 provides descriptive statistics on the participants and their responses to measures of distress, burnout and suicide/other risk. Of note, 63.1% physicians seeking treatment reported clinical levels of distress, 35.9% endorsed clinical levels of burnout, and 9.4% and 3.5% were evaluated by their clinicians to have suicide risk and other risk, respectively, at time of intake. Due to the small number of participants with “other risk,” this variable was not included in subsequent analyses of sample differences.
RFWP Sample Descriptives and Distress Variables.

Note: n = 468 unless otherwise noted due to missing data. ACORN clinical distress is defined as a score of 1.5 or higher. MBI burnout is defined as a score of 5 or higher on either the Maslach Burnout Inventory (MBI) Emotional Exhaustion (EE) or MBI Depersonalization (DP) scales. RFWP = Resident and Faculty Wellness Program, ACORN = A Collaborative Outcome Resource Network Adult Version 11. Suicide and other risk (impairment, domestic violence, threat of aggression towards others) are based on clinician report and coded as any vs. none.
When demographic (gender, race/ethnic status) and programmatic (trainee/faculty status, specialty type) were considered in relation to distress, burnout and suicide risk variables, only a few differences were found. Independently, neither gender (F(1,449) = 0.35, P =.553,
Endorsement and Comparison of Individual ACORN Items by Trainee and Faculty Status.

Note: Items 1–10 are used to calculate the Global Distress Score (GDS). Items 11-13 are intended to be screening items for substance abuse. 0 = never, 1 = hardly ever, 2 = sometimes, 3 = often, 4 = very often in past 2 weeks. Bolded areas show significant differences between trainee and faculty ratings of severity.
*Significant Levene’s test for homogeneity of variances, so adjusted t reported.
Differences in Presenting Concerns
Coding of the presenting concerns yielded categories in work and personal areas (see Table 3). Participants most often endorsed seeking treatment due to multiple concerns (Total Issues
RFWP Participants’ Presenting Concerns.
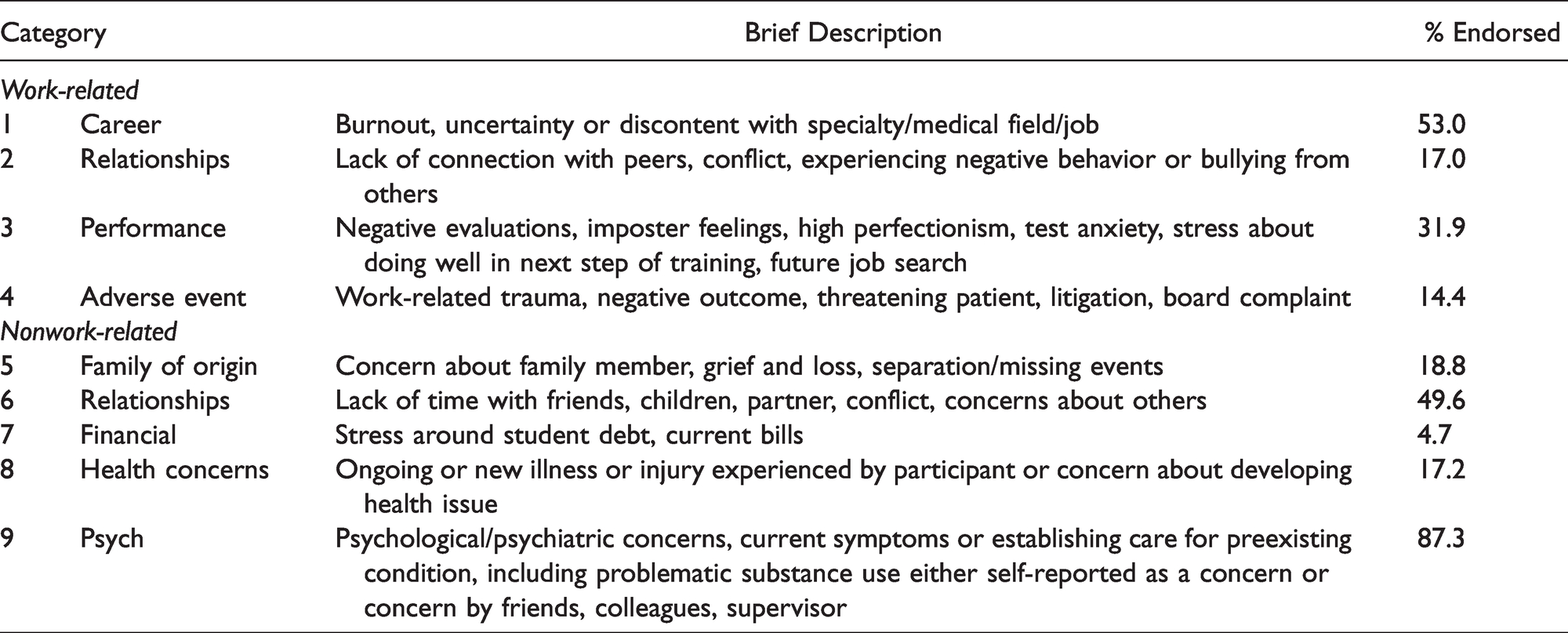
One-way ANOVAs comparing summary scores of work-related vs. nonwork-related issues by gender, race/ethnicity, and status (faculty vs. trainee) found only one significant difference. Faculty reported significantly more work issues, F(1, 462) = 5.78, P = .017,
Gender, Race/ethnicity, and Faculty/Trainee Status as Predictors of Presenting Concerns.

Note: Significant results presented in bold. OR = odds ratio, CI = confidence interval, LL = lower limit, UL = upper limit. Gender < 1 is female; Race/Ethnic < 1 is white/nonLatinx; Faculty vs. Trainee Status < 1 is faculty.
Utilization Differences During Academic Year
Overall utilization of the RFWP was relatively consistent across the year. Results suggested the proportion of individuals engaging with RFWP who are trainees was greater between July-September than faculty (χ2(3) = 11.12, P = .011).
Discussion
Seventeen years ago we launched an on-site physician wellness program designed to reduce known barriers and promote access to individual counseling, coaching and psychiatric treatment. Prior investigation demonstrated positive attitudes about the program and high utilization.22–24 In this investigation, we sought to evaluate whether the cohort seeking services was representative of all physicians eligible for services to determine if our program is seen as accessible to diverse groups of physicians. It is encouraging that participants in the RFWP were representative of all physicians eligible for services in terms of racial/ethnic identity. A model of care that is seen as welcoming and supportive of diverse medical learners and faculty is part of creating a more inclusive and supportive learning and work environment.
The finding that women are more likely to seek clinical services through the RFWP is consistent with findings in the general population 36 and at University of Washington’s on-site wellness program for residents and fellows. 14 In a meta-analysis on male attitudes about seeking treatment for depression, men responded positively to educational outreach about the symptoms of depression, if offered active problem-solving types of therapy such as coaching or cognitive behavioral therapy and if messaging framed “fighting depression” as a sign of strength. 37 Similar types of messaging and therapeutic services may encourage male physicians to be more willing to self-refer when distressed. Although women physicians at our institution were more likely to seek treatment, nationally women physicians may not access care as readily as their non-physician female colleagues—in spite of higher levels of distress, burnout, and family needs.30,38 In a 2016 online survey, almost 50% of women physicians reported barriers to receiving comprehensive mental health treatment in their community. 39
Residents and fellows were more likely to be seen through the RFWP than faculty and two possible explanations seem likely. First, visibility of the RFWP may be higher among trainees as each year RFWP clinicians meet incoming trainees during orientation and provide workshops for chief residents and program directors about how they can assist and refer distressed trainees. Second, the need for psychological services may be greater among trainees given the documented higher rates of burnout and distress during training.28,40,41 This explanation is consistent with our finding that trainees seen at RFWP reported higher levels of clinical distress than faculty. Not surprisingly, trainees more commonly than faculty endorsed in their clinical interview that they wanted to establish care for new or worsening psychological/psychiatric symptoms. Of note, during the higher risk times for distress and suicide (first quarter of the academic year), 21 trainees comprised an even larger proportion of those seeking services. The other high-risk time, January-March, had a similar proportion of trainees seeking help as seen at other times in the year.
On a measure of distress, the ACORN, trainees also reported experiencing more frequent symptoms of anxiety, loneliness, fatigue, attentional and productivity difficulties than faculty seen at RFWP. Similarly, imposter feelings, perfectionism, anxiety about performing well on rotations/exams were more commonly identified by trainees in the intake interview. These types of concerns may guide residency/fellowship program leaders to develop more preventive efforts for trainees. For example, rotations in critical care settings which often elicit a great deal of performance anxiety in trainees may be designed with more in-depth orientation and buddy systems to support learners when they rotate onto these units. Trainees often share how performance anxiety on new rotations and loneliness decrease as their medical skills improve, they become more connected with peers and faculty, and they feel valued by their program.
By contrast, faculty seeking treatment more commonly described concerns about work load, career direction, problematic work relationships, financial pressures and adverse professional events (e.g., adverse or tragic patient outcomes). These types of issues match closely with national discussions about causes distress and interventions for health care professionals.11,12 Faculty physicians may respond best to a menu of psychological supports including referrals to a peer supporter following an adverse event and confidential coaching on career and professional relationship challenges. Through annual presentations to faculty groups and informal consultation with faculty leaders, our clinicians promote our coaching and counseling services as a way for faculty physicians to be more effective in addressing personal and professional challenges.
Gender, clinical specialty, and racial/ethnicity status were unrelated to levels of distress, burnout, and suicidal ideation as opposed to findings typically cited in surveys of physicians. 28,38,42 This discrepancy could be related to the possibility that those seeking professional treatment are different than physicians participating in anonymous surveys or our broad categories of individual characteristics lack sensitivity to detect differences among specialty groups or ethnic/minority groups of physicians.
Consistent with previous findings on the cumulative impact of stress on well-being, 43 physicians who sought professional care in the RFWP reported on average three or more presenting concerns—similar to “the perfect storm.” The majority were in the clinical range on a standard measure of psychological distress and 9% were rated by the RFWP clinician as having suicide risk at the time of intake. This level of distress, suicide risk, and high number of presenting concerns suggest that physician wellness programs need to be prepared to offer a wide range of interventions that vary in intensity and duration to meet the multiple needs of trainees and faculty presenting for treatment.
There are limitations to this study. These findings present one wellness program in a midsize academic medical center that may not generalize to other academic medical centers. Health systems with more ethnic and racial diversity in their trainee and faculty cohorts might be able to evaluate whether there are differences in help-seeking and levels of distress among underrepresented minority physicians. For example, Asian-American participants made up the majority of our nonwhite/non-Hispanic sample. Additionally, due to small numbers of some specific specialties, we had to combine some groups (e.g., lumped medical and pediatric specialties into a single category), limiting our ability to look at presentations of some programs individually. The descriptive, cross-sectional design of this study also does not allow us to infer that participants sought help due to the specific model of care offered. In addition, the categorization of presenting concerns is based upon clinician ratings and may not reflect how clients would have described their main reason for seeking care. Additionally, while the interrater agreement of the quantitative coding data on presenting concerns was generally acceptable, some estimates were on the lower end (i.e. κ = .343 for psychological/psychiatric concerns), and should be interpreted with caution. We have subsequently added to our intake process a self-report measure of presenting concerns. Future research is needed to more closely evaluate what models of care, types of treatment, and dose (number of sessions) lead to significant decreases in burnout, anxiety, depression and suicide risk during medical training and in subsequent years of medical practice.5,12,13
Conclusion
Recent education campaigns to reduce the stigma about physicians seeking mental health treatment and to encourage peers to reach out to distressed colleagues may be having a positive impact on medical culture. 5 Personal stories of physicians who have benefitted from treatment are now being publicly shared and may influence others to seek timely treatment upstream before the onset of severe burnout or depressive symptoms.44,45 Faculty physicians and men may be more motivated to access treatment focused on enhancing career satisfaction and professional development. 37 We are encouraged that two physician groups which often report high levels of burnout and distress, women physicians and residents/fellows, were the most likely to seek professional help in our on-site wellness program.
Supplemental Material
sj-pdf-1-gam-10.1177_21649561211017471 - Supplemental material for Seeking Help in the “Perfect Storm”: Why Residents and Faculty Access an On-Site Wellness Program
Supplemental material, sj-pdf-1-gam-10.1177_21649561211017471 for Seeking Help in the “Perfect Storm”: Why Residents and Faculty Access an On-Site Wellness Program by Sydney Ey, PhD, Benjamin Ladd, PhD, Marie Soller, MD and Mary Moffit, PhD in Global Advances in Health and Medicine
Footnotes
Acknowledgments
The authors would like to thank J Mark Kinzie, MD, PhD, Program Director, Department of Psychiatry, George Keepers, MD, Chair, Department of Psychiatry, and Nathan Naruponjirakul, Graduate Medical Education. Special thanks to Kris R Henning, PhD, Professor, Department of Criminology, Portland State University for his significant assistance on classification and analysis of presenting concerns. Finally, the authors wish to acknowledge the willingness of OHSU residents, fellows, and faculty to share their stories.
Compliance
Human Subjects approval by Oregon Health and Sciences University IRB #9003
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.