
Abstract
Background
Depression, generalized anxiety, fatigue, diminished physical function, reduced social participation, and pain are common for many older adults and negatively impact quality of life. The purpose of the overall trial was to compare the effects of cognitive-behavioral therapy (CBT) and yoga on late-life worry, anxiety, and sleep; and examine preference and selection effects on these outcomes.
Objective
The present analyses compared effects of the 2 interventions on additional outcomes (depressive symptoms, generalized anxiety symptoms, fatigue, pain interference/intensity, physical function, social participation); and examined whether there are preference and selection effects for these treatments.
Methods
A randomized preference trial of CBT and yoga was conducted in adults ≥60 years who scored ≥26 on the Penn State Worry Questionnaire-Abbreviated (PSWQ-A), recruited from outpatient medical clinics, mailings, and advertisements. Cognitive-behavioral therapy consisted of 10 weekly telephone sessions. Yoga consisted of 20 bi-weekly group yoga classes. Participants were randomized to(1): a randomized controlled trial (RCT) of CBT or yoga (n = 250); or (2) a preference trial in which they selected their treatment (CBT or yoga; n = 250). Outcomes were measured at baseline and post-intervention.
Results
Within the RCT, there were significant between-group differences for both pain interference and intensity. The pain interference score improved more for the CBT group compared with the yoga group [intervention effect of (mean (95% CI) = 2.5 (.5, 4.6), P = .02]. For the pain intensity score, the intervention effect also favored CBT over yoga [.7 (.2, 1.3), P < .01]. Depressive symptoms, generalized anxiety, and fatigue showed clinically meaningful within-group changes in both groups. There were no changes in or difference between physical function or social participation for either group. No preference or selection effects were found.
Conclusion
Both CBT and yoga may be useful for older adults for improving psychological symptoms and fatigue. Cognitive-behavioral therapy may offer even greater benefit than yoga for decreasing pain.
Introduction
Worry, a cognitive component of anxiety, is common in older adults.1,2 While cognitive-behavioral therapy (CBT) is the most studied non-pharmacological treatment for late-life anxiety/worry and has a strong evidence base,3-5 there is growing interest in and evidence for the use of yoga to reduce anxiety in older adults.6,7 To our knowledge, this study was the first to compare yoga and CBT for the treatment of late-life worry and a variety of related symptoms in a large sample of older adults. Findings from previously published analyses of primary and secondary outcomes showed that CBT and yoga were both effective at reducing worry and anxiety, and a greater impact was seen for CBT compared with yoga for improving sleep. 8 The focus of this investigation is on a variety of prevalent and interrelated symptoms commonly reported by older adults with substantial worry: depressive symptoms, generalized anxiety symptoms, fatigue, and pain.
Comorbid depressive symptoms are common in older adults who report anxiety/worry.9-13 High levels of worry are also associated with physical health consequences, including fatigue and pain.17,18 Fatigue becomes more prevalent with increased age. 19 Fatigue is a complex and multi-dimensional symptom and has negative implications for quality of life and physical performance (including frailty).20-23 Similarly, pain is a significant issue for older adults and has been associated with worry/anxiety symptoms in multiple studies. In older adults, chronic pain is common and is associated with substantial suffering, isolation, disability, risk of falls, and greater health care costs.24-30 Recent work highlights the relationship between greater pain and worry in older adults.31,32 In addition to treating psychological symptoms such as worry/anxiety and depression, CBT has demonstrated efficacy for managing pain symptoms in older adults.33,34
We conducted a two-stage randomized preference trial comparing CBT and yoga for treating worry in older adults. This design was chosen because it allows for a test of traditional randomized effects as well as a test of preference effects. Preference has been found to have an effect on clinical outcomes, adherence, attrition, and stratification.35-37 Preference for treatment is also a key component of shared decision-making and best practice standards. Half of participants were randomized to CBT or yoga, while the remainder were randomized to choose their treatment. As reported above, findings for the primary outcome (worry) and secondary outcomes (anxiety, sleep) have been published elsewhere. 8 In this secondary data analysis using data from the randomized arm (N = 250), we compared the effects of CBT and yoga on several exploratory outcomes: depressive symptoms, generalized anxiety symptoms, fatigue, pain interference, pain intensity, physical function, and social participation. Using data from both the randomized and preference trial arms (N = 500), we examined the effects of preference (i.e., an effect on outcome from having a choice in treatments compared with being randomized) and selection (i.e., an effect on outcomes by making a specific treatment choice) on depressive symptoms, generalized anxiety symptoms, fatigue, pain interference, pain intensity, physical function, and social participation.
Methods
This study received approval from the Wake Forest School of Medicine Institutional Review Board. Participants were adults aged ≥ 60 years with elevated self-reported worry scores (≥26) on a standardized measure [Penn State Worry Questionnaire-Abbreviated (PSWQ-A)].38,39 Exclusion criteria included the following: current psychotherapy, current yoga practice, current alcohol or substance abuse, dementia diagnosis, cognitive impairment (based on the Telephone Interview of Cognitive Status-Modified), 40 current psychotic symptoms, active suicidal ideation with plan and intent, change in psychotropic medications in the last 4 weeks, and hearing loss that would prevent participation in study interventions. In a two-step screening process, participants provided verbal informed consent for a brief initial screen and written informed consent for the full screen.
Procedure
Study procedures have been described in detail previously. 41 Participants were recruited through outpatient clinics, flyers, mailings, and newspaper advertisements. Eligible participants were randomized to one of the following 3 conditions: randomized controlled trial (RCT) CBT, RCT yoga, or preference trial. Randomization was electronically linked to eligibility based on entry of the baseline forms, and the sequence of random assignments was only available to the statisticians who generated the randomization list and the programmers who implemented the randomization process. Individuals assigned to the randomized trial were then further randomized into CBT or yoga, stratified by whether they used psychotropic medication. Randomization was completed using a permuted block algorithm with random block lengths over a secure web-based data management system.
Assessment
All self-reported study assessments (described in detail elsewhere (41)) were completed by telephone, in person, or by mail. The current study presents analyses of exploratory outcomes collected at baseline (Week 0) and following intervention completion (Week 11). As exploratory analyses, nominal P-values are presented and significance for each outcome set at .05.
Outcomes
PROMIS-29
Constructs from the PROMIS-29 measure included in these analyses were: depressive symptoms (8 items), fatigue (4 items), pain interference (4 items), physical function (11 items), ability to participate in social roles and activities (4 items), and pain intensity (1 item).
Generalized anxiety disorder screener (GAD-7)
The GAD-7 is a self-report measure of DSM-IV generalized anxiety symptoms that has been validated for use in the general population.42,43
Interventions
Cognitive-behavioral therapy participants completed up to 10 weekly 50-minute telephone-based psychotherapy sessions using a standardized workbook (with homework/daily practice). Each session focused on an assigned workbook chapter with standard CBT topics (e.g., relaxation techniques, cognitive restructuring) to manage worry and anxiety. 41 Cognitive-behavioral therapy sessions were conducted by 2 Licensed Clinical Social Workers who received weekly supervision from the senior author (GAB).
Yoga participants completed up to 20 biweekly 75-minute yoga classes based on the Relax into Yoga for Seniors gentle Hatha yoga program. 44 Classes included centering and breathing, a gentle physical posture practice, and meditation/relaxation. Yoga was provided by 7 yoga instructors with at least RYT 200 certification.
Fidelity
All sessions were audio- or video-recorded; 10% were selected randomly for rating by CBT or yoga experts for protocol adherence and intervention delivery competence. On a 9-point scale, mean therapist ratings were >6 on adherence and competence items.3,45,46 Mean yoga instructor ratings were >6 on adherence and competence items for all but 1 instructor (who stopped teaching study classes prior to retraining).
Statistical Analyses
Our general approach to analysis of this study has been previously described. 8 Baseline descriptive statistics by intervention group and within both the randomized and preference trials were calculated, and t-tests and chi-square tests were used to compare the CBT and yoga preference groups on baseline characteristics.
Within RCT analyses
Constrained, repeated measures analysis of covariance, with an unstructured covariance matrix to account for multiple measurements (Weeks 0 and 11) not being independent, was used to estimate the intervention effect on the exploratory outcomes.47,48 The intervention effect was estimated by comparing mean scores between CBT and yoga groups in the RCT.47,48 Pre-specified effects for baseline psychotropic medication use, sex, and race (both related to depression; race dichotomized) and intervention effects specific to each measurement time were contained in this model. A contrast was used to test for intervention effects at Week 11 using a two-sided .05 significance level. Analyses were performed consistent with an “intent to treat” philosophy (i.e., all randomized participants were included in their allocated groups). Participants who achieved a clinically meaningful change in outcomes from baseline to Week 11 were identified based on thresholds from published literature. Marginal standardization [46] of results from logistic regression (adjusted for baseline psychotropic medication use, sex, and race) was used to estimate the proportion of participants achieving minimally important differences (MIDs) in each intervention group (and risk differences between groups); 95% confidence intervals were calculated using a bootstrap confidence intervals with 1000 replications.
Estimation of preference and selection effects using both the RCT and preference study data
Preference and selection effects were estimated for each outcome using a mixed-model repeated measures framework and data collected in both randomized and preference trials. 49 Dummy variables were used to represent membership in the randomized and preference groups, intervention assignment in the randomized group, and intervention preference in the preference group. The fitted model was used to estimate the adjusted means and variance-covariance matrix needed to compute these effects and their standard errors. The standard errors associated with the preference and selection effects were derived using formulas provided by Walter and colleagues. 50 Statistical significance was assessed at the two-sided, .05 level in these secondary analyses.
Results
Baseline Characteristics of Study Participants.

aValues are N (%) unless otherwise specified.
Baseline Scores on Outcome Measures.

Exploratory Outcomes for the RCT
Week 11 Results from the Randomized Trial (Exploratory Outcomes) a .

aAll models are adjusted for sex, race, and baseline psychotropic medication use.
Participants in both the CBT and yoga groups experienced improvements in depressive symptoms, fatigue, generalized anxiety symptoms, and social participation upon completing the intervention. However, there were no significant differences in the amount of improvement between the CBT and yoga groups. Minimal changes were seen for physical function for either intervention group.
Meaningful Change
Minimally Important Differences (MID) for Exploratory Outcomes: Logistic Regression Results Modelling the Probability of Reaching the MID 1 .

1Adjusted for baseline psychotropic medication use, sex, and race.
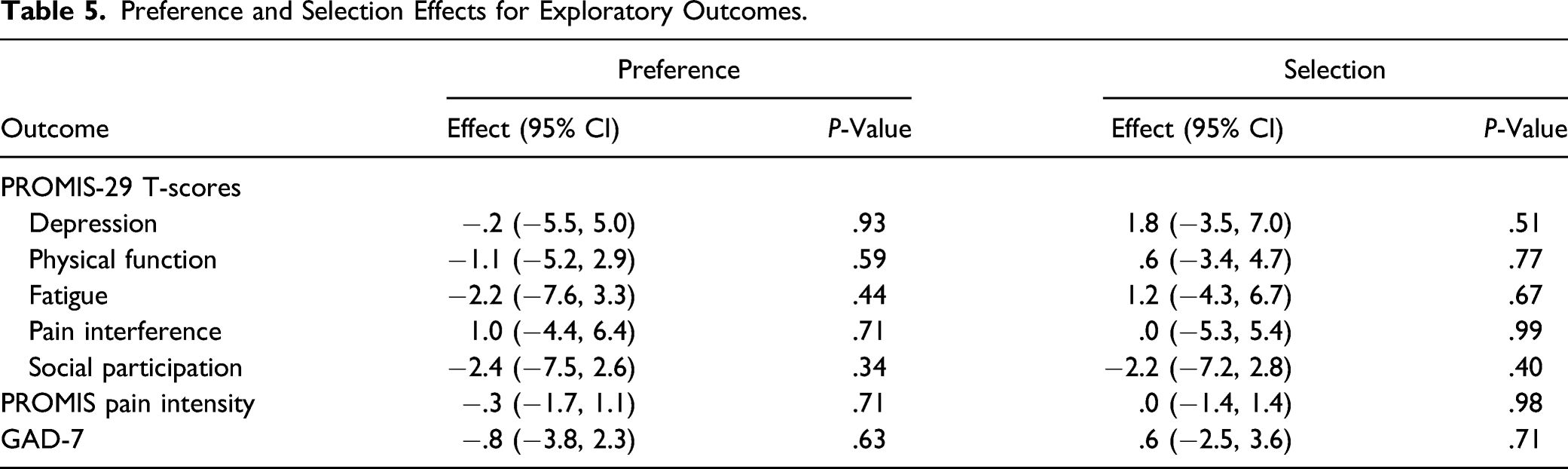
Preference and Selection Effects
Preference and Selection Effects for Exploratory Outcomes.
Discussion
We examined the effects of CBT and yoga on depressive symptoms, generalized anxiety symptoms, fatigue, pain (interference and intensity), physical function, and social participation in a sample of community-dwelling older adults who reported significant levels of worry. Findings from these analyses showed that depressive symptoms, generalized anxiety symptoms, fatigue, and social participation were improved in both intervention groups upon completion of the intervention with no statistically significant between-group differences. Results showed greater reductions in pain (both interference and intensity) favoring participants randomized to CBT vs yoga. Little change was noted in physical function for either intervention group. Our findings support the use of both CBT and yoga for improving depressive symptoms, generalized anxiety symptoms, fatigue, and social participation in older adults. For those reporting issues with pain, significantly greater declines in both pain interference and pain intensity were seen for those in the CBT intervention group (compared with yoga).
There are strong data to show that CBT benefits the outcomes of interest examined here, and our results are consistent with prior findings.3,59,60 Yoga has demonstrated efficacy for anxiety reduction; however, little yoga research has focused specifically on older adults, especially those with high levels of worry.61-69 To our knowledge, there have been no other comparative effectiveness studies of CBT and yoga for improving worry and related outcomes in older adults. Our findings demonstrate that yoga is effective in reducing some of the additional symptoms associated with worry. This finding is important because older adults prefer nonpharmacological treatments (primarily psychotherapy) over medication for anxiety and depression.70,71 Prior to this study, no one examined relative preference for yoga for the treatment of anxiety. Analyses of data from the current study suggest that older adults do not differ in their preference for psychotherapy or yoga. 72 This finding in conjunction with those reported in the current study suggest that yoga is an efficacious and well-liked intervention for late-life worry and associated symptoms.
Interestingly, when the randomized and preference trial data were combined, no preference or selection effects were seen for any of the outcomes in these analyses. These findings were surprising as one would expect that being given a choice of interventions rather than being randomized (preference) would have a beneficial effect on study outcomes. It had no effect. One might also expect that choosing one’s preferred intervention (selection) would impact study outcomes. It did not. We can conclude from these findings that the opportunity to select CBT or yoga and which of those behavioral interventions is selected will not impact the effect of the intervention on depressive symptoms, generalized anxiety symptoms, fatigue, physical function, social participation, and pain. Older adults and their health care providers can confidently recommend either CBT or yoga, as they have shown similar efficacy whether chosen or prescribed.
Perhaps the most relevant question is whether the change observed in these outcomes is at a level that is meaningful to participants. Beyond statistical significance, were the changes we observed in the various exploratory outcomes in the randomized trial enough to make a difference in their daily lives? As we compared average improvements in exploratory outcomes with published data on MIDs, we found meaningful levels of change for the majority of participants in both intervention groups for depressive symptoms, fatigue, and generalized anxiety symptoms. While the average changes from baseline were less than the MID for physical function, pain interference, and pain intensity for either intervention group, some participants did achieve meaningful change in these areas as well. It is notable that while participants were not recruited into this study based on level of pain at baseline, we saw meaningful levels of change for pain interference for a substantial minority of RCT participants, and to a somewhat lesser extent for pain intensity.
While no prior work has compared CBT and yoga to look specifically at worry, prior studies have compared CBT and mindfulness-based intervention approaches (of which yoga is one) for pain. In the present study, we saw a significant between-groups difference for both pain interference and pain intensity favoring the CBT group. This finding is in contrast to a relatively recent RCT conducted with adults (aged 20-70 years) with chronic low back pain comparing treatment with mindfulness-based stress reduction (MBSR), CBT, and usual care. 74 They found that both MBSR and CBT participants demonstrated a greater improvement in pain and functional limitations related to pain than the usual care group, and no significant differences were seen between MBSR and CBT. (To our knowledge, no comparable study has been conducted with a sample of older adults.) There are data that suggest potential neural mechanisms for mindfulness-based interventions to impact pain. Specifically, recent experimental findings suggest that people reporting higher levels of mindfulness report less pain intensity and unpleasantness (i.e., feel less pain) and show greater deactivation of the posterior cingulate cortex (brain region involved in sensory, cognitive, and affective appraisals of pain). 75 These data suggest that both CBT and yoga remain viable options that warrant investigation in older adults, particularly for a study focused on pain-related outcomes.
There are several limitations of this study. First, despite substantial efforts to recruit a diverse sample in terms of gender and race/ethnicity, the ultimate sample consisted of White women which may somewhat limit the generalizability of our findings. Second, as a randomized preference trial, all potential participants had to be willing to be randomized to either an RCT or a preference trial, meaning that they needed to agree in advance to either be randomized or select their intervention. Potential participants not willing to agree to this type of randomization may have dropped out earlier in the recruitment process, thereby decreasing generalizability of study findings. Third, given that multiple comparisons were conducted, it is possible that findings are due to Type 1 error. Finally, there was no objective performance measure of physical function as we relied on a brief self-report measure for this key variable.
These points notwithstanding, this study has a number of substantial strengths. Clearly, the two-stage randomized design allowed us to examine preference and selection effects in addition to the more traditional RCT findings, and inclusion of multiple exploratory measures allowed us to examine impact of both CBT and yoga interventions on depression, generalized anxiety symptoms, fatigue, pain, and social participation – all important constructs that contribute to quality of life in older adults.
Conclusions
These findings suggest that both CBT and yoga may be useful approaches for depressive symptoms, generalized anxiety symptoms, fatigue, and social participation in community-dwelling older adults who report high levels of worry. CBT may show greater benefit for improving pain-related outcomes. Finally, recommending an intervention or allowing a person to choose an intervention had no effect on outcomes.
Footnotes
Authors Contributions
Data Access, Responsibility, and Analysis: Suzanne C. Danhauer, PhD and Gretchen A. Brenes, PhD had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Andrea Anderson, M.S., Jasmin Divers, PhD, and Michael E. Miller, PhD conducted the analyses. Study conception and design: Brenes, Danhauer, Divers, Miller. Acquisition, Analysis, or Interpretation of Data: Anderson, Brenes, Danhauer, Divers, Hargis, Miller. Drafting of the Manuscript: Anderson, Brenes, Danhauer, Divers, Hargis, Miller. Critical Revision of the Manuscript for Important Intellectual Content: Anderson, Brenes, Danhauer, Divers, Hargis, Miller. Obtaining Funding: Brenes, Danhauer, Divers, Miller. Administrative, Technical, or Material Support: Anderson, Brenes, Danhauer, Divers, Hargis, Miller. Supervision: Brenes, Danhauer, Divers, Miller
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported through a Patient-Centered Outcomes Research Institute (PCORI) Program Award (CER-1511-33007; MPIs Brenes and Danhauer) and by the Office of the Dean at Wake Forest School of Medicine. PCORI was not involved in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Disclaimer
All statements in this report, including its findings and conclusions, are solely those of the authors and do not necessarily represent the views of the Patient-Centered Outcomes Research Institute (PCORI), its Board of Governors or Methodology Committee.