
Abstract
The Diabetes Self-Management Education and Support (DSMES) program provides education and medical monitoring of diabetes to Veterans through the Virtual Medical Center (VMC). Qualitative interviews were conducted with 15 key stakeholders (4-DSMES VMC trainers, 5-clinical faculty, and 6-Veterans) from across Ohio urban and rural populations for up to 1h about their experiences using the program and suggestions for improvement. All the Veterans interviewed were able to access care within the DSMES VMC and reported a positive experience using the program, and improved diabetes self-management. Other stakeholders suggested more administrative and technical support for the DSMES VMC to increase awareness for VA staff and Veterans of the program to improve recruitment, and to shift to a web-based platform that is more easily accessible by clicking a link to reduce technical issues with downloading the program. These findings can inform future implementation efforts using technology to increase access to care allowing better health education for Veterans.
Introduction
The importance of self-management of chronic illnesses such as diabetes is becoming increasingly important especially in the Veteran population where approximately 1 in 4 Veterans enrolled in the Veterans Health Administration (VA) are afflicted with diabetes mellitus. 1 Diabetes Self-Management Education and Support (DSMES) was developed in the VA as a collaboration between a diabetes team and Veteran to ensure the Veteran gains knowledge and skills to successfully self-manage their diabetes. 2 This program was based on the National Diabetes Self-Management Education and Support toolkit from the Center for Disease Control and Prevention (CDC) and achieved accreditation and recognition by meeting the 10 national standards of excellence by national diabetes groups such as the American Diabetes Association. 3 DSMES participation can help improve quality of life through changes in health behaviors (eg, improved nutrition and medication adherence) and prevent diabetes complications such as heart disease and chronic kidney disease. 4
Many VA sites offer in-person diabetes shared medical appointments for groups of Veterans to meet with a multidisciplinary team for diabetic care management and learn self-management. 5 Unfortunately, few VAs provide DSMES services. Restrictions presented during the COVID-19 pandemic and travel burdens for rural Veterans halted the in-person DSMES program triggering the use of the VA Virtual Medical Center (VMC).
The VMC, developed in 2015, is a virtual environment for Veterans and their family members to access health information from home. The VMC serves as a platform that facilitates social connection for Veterans and offers virtual telehealth technologies and digital game-based learning. This approach provides Veterans with access to educational resources, diabetes management tools, staff support, and eliminating the need to travel to the nearest VA hospital. 6 In March 2020, the COVID-19 pandemic prompted the VA to shift from in-person visits to pandemic-related safety protocols requiring virtual care delivery. 7 For Veterans with diabetes the VMC can help reduce risks of comorbidities to diabetes such as heart disease, hypertension, obesity, and cancer. 8
Digital game-based learning has been applied across diverse sectors including business entities, academic science, 9 and education 10 to achieve objectives and facilitate training programs. The VMC employs gamification, a design approach that incorporates gaming engagement and motivational elements to reinforce desired healthy behaviors like dieting and exercise. 11 When health education strategies integrate gamification, they transform the participant's intrinsic motivation from completing a mandatory task into a captivating and immersive experience.12,13 Medical avatars are used within the VMC to make the virtual environment more visually compelling and adept at motivating Veterans to meet personal goals. The use of avatars resembling older participants in a 3D virtual reality intervention showed improvements to lifestyle changes such as physical activity. 14 Although the VMC offers a virtual platform for Veterans to receive DSMES remotely, this approach also has challenges related to technical aspects. Veterans who live in rural areas face significant challenges accessing healthcare due to limited technological infrastructure such as digital literacy and broadband issues that hinder their ability to utilize telemedicine services.15,16 The advanced age of many Veterans exacerbates the issue, as they may lack familiarity with modern technology, posing a barrier to effectively navigate and benefit from digital healthcare solutions.15,17
Older individuals’ willingness to accept virtual healthcare is currently being investigated. Older Veterans may not have the technological devices or knowledge of how to successfully participate in the VMC. 17 Veterans who used the DSMES VMC appreciated the chance to connect with peers who shared the same disease while they participated in interactive games such as virtual grocery shopping, virtual fitness center, and virtual cooking classes to learn about the effect of diabetes on their bodies, average blood sugar levels, and glucose metabolism. To identify factors that contribute to successful implementation and inform future implementations, a formative evaluation 18 of the VA DSMES VMC program was conducted to learn more about the users’ experiences through semistructured interviews. A formative evaluation uses methods like a summative evaluation but emphasizes a goal of identifying ways to adapt and improve the implementation of the subject of the evaluation. 19
Methods
A formative evaluation of the DSMES VMC was conducted using qualitative methods through semistructured interviews with healthcare providers and their patients. We asked providers about their experiences working in the VMC and to help manage their patients with diabetes mellitus; we asked patients about their experiences and managing their diabetes after attending DSMES VMC sessions. Our goal was to identify facilitators and barriers for improvement of the VMC to inform successful future implementation. Semistructured interview guides (see Appendix I) were created by combining the Technology/Task Fit and Unified Theory of Acceptance and Use of Technology (TTF-UTAUT) model. 20 This combined model was chosen because of the novelty of the VMC and the different types of VMC users. The interview guide assisted in providing elicit descriptions of stakeholders’ experiences with using the DSMES within the VMC, recommendations, and suggested improvements for the program. Telephone interviews were approximately 20-60 min each.
The VA Northeast Ohio Healthcare System's Research and Development Committee review and determination of the evaluation plan 21 and deemed it nonresearch and quality improvement activity designed for internal VA purposes on August 30, 2020 (VHA Handbook 1200.21). The interview guide was approved by employee unions before administering. A DSMES program lead provided names of Veterans who participated in DSMES classes within the VMC, clinical faculty who conducted the courses and met with their patients within the VMC, and trainers involved in training the faculty to provide this education within the VMC. Clinical faculty were invited to participate in a 1h telephone interview by VA email. Veterans were invited through letters outlining the interview's purpose for program improvements, requirement for verbal consent, recording of information, and assurance of name removal for publication. Veterans were asked to respond to the letter if interested in participating in interview by calling the evaluation team for further clarifications. Invitations for participation were emailed to 17 clinical faculty and 6 trainers. Letters were mailed to 13 Veterans. Once the evaluation team received consent, an appointment was scheduled, and participant ID created.
Interviews were led by a team of interviewers with over 20 years of combined experience in qualitative data collection and analysis. The interviewers were trained in health services research and quality improvement implementation to inform, advise, and evaluate strategies designed to improve access to primary and specialty care. Training is completed when team members are onboarded. Interviewers followed a standard script explaining the interview process including the confidentiality and voluntary nature of the interview. Interviewers also adhered to the open-ended questions in semistructured interview guide adding only grounded probe questions (Appendix I) using the respondent's words throughout the interview. 22 During the interview each participant consented to being audio-recorded. The data were anonymized, stored on a VHA secure server, transcribed verbatim, and quality checked by a member of the analysis team. To analyze the qualitative data a rapid matrix analysis23,24 was completed using a priori neutral domains derived from the UTAUT model to code data from transcripts of interviews with Veterans (Appendix II) and clinical staff and trainers (Appendix III); adding inductive domains as identified. The matrixes were populated with data from each transcript by members of the qualitative analysis team. For each populated domain, analysts sought to identify barriers and facilitators to program implementation and identified targeted actionable steps to improve the program. Analysts met weekly to discuss and build consensus in team meetings where any coding discrepancies were identified and resolved often by refining code definitions to develop consistent coding of data within the matrix. Analysis was ongoing and iterative; analysts referred back to interview transcripts to ensure that the identification and assignment of codes were grounded in the data. The completed matrix was discussed by the entire team to validate results. 25 Results from this study could inform adaptation of healthcare delivery when a virtual modality is preferred or necessary.
Results
Fifteen (n = 15) key stakeholders (4 VMC trainers, 5 clinical faculty, and 6 Veterans) across Ohio urban and rural populations agreed to participate and were interviewed. Data collection was completed between February 2021 and June 2021. The focus was to gain knowledge of the experiences with training providers on how to use the VMC to provide care and receiving or providing virtual DSMES care within the VMC. Perceived facilitators and barriers of the VMC were also explored. Most trainers reported about their experiences using the program, providing care, and suggestions for improvement, while clinical faculty reported challenges with downloading the application. Despite these issues, Veterans who were able to access care within the VMC reported a positive experience using the program, better self-management, and easier access to diabetes care. Stakeholder's quotes can be found in Table 1.
Stakeholder Quotations.

The table above lists supporting quotations for results.
Veteran Experience: Facilitators and Use of Avatars
All the Veterans interviewed had previous diabetes education in-person with providers, but they agreed that they learned how to better manage their diabetes and implement healthy lifestyle changes through the VMC. The VMC gave Veterans the opportunity to join the program anonymously through the patient avatars instead of using a camera for live video feed. This virtual learning environment was preferred by some of the Veterans because of its accessibility with no requirement to travel to the VA and the materials available for diabetes management. One Veteran shared how it took some time to get use maneuvering the avatars around the virtual platform but “once you get the hang of it” it was like a game. One Veteran highlighted how the VMC was targeted for everything he wanted to learn whereas other resources like Google “you have to keep looking further into something.” All the Veterans reported that they enjoyed learning about their disease, hoped it continued, and would recommend the VMC to others.
Clinical Faculty Experience: Facilitators and Perspectives
The clinical faculty described many benefits of the VMC. For example, one clinical faculty shared that the VMC provided more health information for Veterans than a single in-person appointment. Another explained how the VMC helped the participating Veterans meet their personal goals, as well as better health outcomes such as improvements in blood pressure, diet, and blood sugar control. One clinical faculty also described how the Veterans connected with each other and had the option to create small groups in the VMC.
Barriers and Challenges of DSMES Within the VMC
Technical issues relating to downloading and initial set-up on personal home computer, long patient instructions, and duplicate avatars were barriers reported by most of the stakeholders interviewed and may account for the low number of VMC users. A Veteran mentioned how the number of avatar options was limited so multiple faculty in one class looked the same. Most Veterans reported satisfaction with the technical support given to use the VMC. One Veteran reported an easy log-in experience when using mailed instructional materials and receiving assistance from the help desk. A clinical faculty recognized the need for the VMC to be more user friendly. Sometimes teaching Veterans to use the program required an extensive time commitment. Another clinical faculty suggested making the VMC more user friendly with easier movements like a video game using a joystick. One clinical faculty reported on how Veterans struggled to load the desktop application due to the size of the program. While VA Office of Information Technology (IT) could assist Veterans with technology issues, faculty also needed computer support during and prior to DSMES sessions. A clinical faculty reported difficulties getting Veterans referred to use the VMC due to the lack of awareness about VMC. They also stated that there was a need for administrative and technical support to help Veterans explore the VMC. The clinical faculty needed other providers to refer Veterans to the classes offered through the VMC.
Trainer Experience: Involvement and Suggestions
One of the trainers interviewed explained how they became involved with the VMC because of the increase of access it provides Veterans and that they would recommend the VMC to others. Another trainer recognized the technical issues that some Veterans had while trying to access the VMC and suggested shifting to a web-based platform that is more easily accessible by clicking a link to reduce issues with downloading the program.
Differing Points of View
The clinical faculty and trainers expressed concerns about the VMC that were not uniformly shared by Veterans. All the clinical faculty conveyed concerns about technical barriers in the VMC, expressing apprehension that older Veterans might be deterred or lack the required equipment for active participation. Additionally, clinical faculty reported that the VMC lacked user-friendliness. To mitigate the technical issues associated with downloading the program it was suggested that the VMC needs to transition into a web-based platform to enhance accessibility. Some clinical faculty believed there was a low attendance of Veterans in VMC due to insufficient awareness and inadequate support for the program. However, most of the Veterans interviewed in this evaluation reported not having issues with the VMC. Veterans highlighted how they asked the clinical faculty or used the help category for assistance from VA Internet Technicians when needed in the VMC. A few Veterans explained that technical support was excellent and that once they received the instructions on how to access the VMC it was easy to do and “like a game.” The Veterans unanimously gave positive feedback about their experience with VMC, even remarking how they would recommend the program to others. One Veteran stated a preference for utilizing the VMC for all appointments to avoid the need to travel to the VA. Another finding from the Veteran interviews was the desire for increased attendance of Veterans for more interactions. If more Veterans participated in VMC there would be opportunities for Veterans to share experiences related to diabetes and medications. Overall, the Veterans found the program and platform relatively easy and enjoyable to access and use; the clinical faculty and trainers believed a few changes could make the virtual platform better.
Discussion
The purpose of this evaluation was to explore the experiences of VA staff involved with training others to provide diabetic education, VA providers involved with facilitating this education, and Veterans with diabetes who received DSMES within the VMC. Veterans who accessed DSMES within the VMC had positive experiences using the program reporting better self-management and easier access to diabetes education. VA clinical faculty and trainers reported advantages of the program for Veterans and VA staff, as well as the challenges in getting more technical support and Veteran referrals for the program. Our findings highlight the facilitators and barriers of utilizing the VMC via avatars and preferred virtual accessibility and suggests this is an important option for many Veterans, to improve health behaviors.
Virtual technology has been shown to increase access for preventive health and to resources that improve health such as recipes, exercise, stress and anxiety management. 26 The Veterans interviewed in this evaluation described the benefits of virtual learning from DSMES within the VMC, their ability to access it, and adopt healthy lifestyle changes. Studies have shown that technology can assist in helping Veterans shift to healthier habits. 14 The Veterans interviewed were satisfied with the remote access to diabetes care, preferring to utilize the VMC rather than traveling to an in-person meeting. The VMC allowed Veterans to learn at their own pace in their home environment to reach personal health goals. Avatars within the VMC promoted an interactive experience. Previous studies have described the effectiveness of medical avatars for patient learning and health outcomes. One study reported how avatars with digital characteristics can serve as health coaches to foster health promotion and lifestyle changes in Veterans. 14 Another provided evidence that showed psychosocial improvement for patients who used avatars in virtual healthcare environments. 26 Some Veterans referred to DSMES VMC as it being “like a game.” Gamification adds gaming elements such as rewards for participation or task completion and promotes motivation, engagement, and improvement for users. 27
One of the clinical faculty noted how older Veterans did not understand the technology for using the VMC. In previous studies, technology is known to offer abundant resources, but the absence in ease of use can become a barrier for elderly users. 27 Although the Veterans reported having technical issues, they also reported positive experiences receiving assistance which was “excellent” or “real easy.”
Clinical faculty stated that there was a lack of awareness for Veterans to know about what was offered in DSMES VMC. Enhancing administrative and technical support for the DSMES VMC could potentially improve Veteran referrals, thereby expanding program participation. A clinical faculty reported that more support was also needed to help the Veterans with exploring the VMC. Studies have suggested that elderly patients need support with virtual technology due to cognitive or physical abilities. 27 Participant barriers could be addressed by offering support to Veterans as they begin the program so that the clinical faculty have more time to focus on the DSMES education and less time teaching the programing basics (eg, walking, sitting, asking questions, etc). Based on our findings, future implementation of the VMC should consider packaging the platform into an application that is easy to download and install with technical support available for using the application.
Limitations
Our findings and recommendations are based on a small sample size due to the relatively low and limited number of VA providers, staff, and Veterans involved in the DSMES VMC at the time of this evaluation. Most respondents had not regularly used the VMC in a long time and in general said that they had “not a lot of experience” and that it “needs to be updated to meet Veteran needs, in order to be used.” Future studies that use mixed methods with a larger sample could offer further understanding of the faculty and Veteran satisfaction with DSMES sessions using the VMC platform.
Conclusion
Although the stakeholders interviewed noted some challenges in using the VMC DSMES platform, overall, respondents felt that the program increased access to resources on diabetes self-management. Veterans who were able to access care within the VMC reported a positive experience using the program reporting better self-management and easier access to diabetes education. VA clinical faculty and trainers reported the advantages of the program for Veterans and VA staff as well as the challenges and offer some suggestion for improvement. The VMC provided a virtual opportunity for Veterans to share experiences and learn to live a healthier lifestyle, especially during the COVID-19 pandemic when there was a disruption in care.
Footnotes
Acknowledgments
We are grateful to the Veterans Health Administration staff and Veterans who generously gave their time and shared their experiences with our team. We would like to acknowledge Michael Heh from the Employee Education Service department of Veterans Affairs.
Declaration of Conflicting Interests
The authors declared that there are no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This evaluation was reviewed and declared to be nonresearch by the VA Northeast Ohio Healthcare System Research and Development Committee and did not require Institutional Review Board oversight.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Memorandum of Understanding with the Dayton VA Medical Center through the DOD/VA Joint Incentive Fund (JIF) National Defense Authorization Act 2003 Section 721, amended Section 8111 of Title 38 of the United States Code.
Appendix I. Semistructured Interview Guides.
Grounded probes/prompts: Grounded prompts are used to elicit detailed responses and should be used verbatim.
What do you mean by ____________? Tell me more about___________. Give me an example of ____________. Tell me about a time when ____________. Who ____________? Where ____________? What, if anything, was helpful about ________________? What, if anything, was not helpful about ________________? What, if anything, made ________________ difficult? What, if anything, made ________________ easier?
Tell me about your experiences using the DMSES within the VMC.
How often to you access the system?
How did you find out about the system?
How did you decide to use the system?
Effort and Facilitating: Ease of use.
Tell me about times you used the system.
Probe: What components, if any, did you find helpful?
Probe: What components, if any, did you unhelpful?
Tell me about other on-line resources, if any, you have used to help you manage your health.
Performance: Results
What, if any, are your goals in using this system?
Have you met your goals?
Probes
To what extent, if at all, has your ability to manage your health changed?
Performance: Behavior change
Have you made any changes to your lifestyle since participating in this platform or using these resources?
Motivation
Under what circumstances do you expect to access the system again?
Would you recommend this system to another Veteran?
What would you tell Veterans about it?
Social Support
What, if anything, about this system have you discussed with your VA providers?
What, if anything, about this system have you discussed with your family, friends, and/or caregiver(s)?
What, if anything, could have improved your experience?
Is there anything else you would like us to know?
Grounded probes/prompts: Grounded prompts are used to elicit detailed responses and should be used verbatim.
What do you mean by ____________? Tell me more about___________. Give me an example of ____________. Tell me about a time when ____________. Who ____________? Where ____________? What, if anything, was helpful about ________________? What, if anything, was not helpful about ________________? What, if anything, made ________________ difficult? What, if anything, made ________________ easier? What was the impact of ________________?
Tell me about your role at the VA.
Tell me about how you first learned about using the VMC.
Tell me about how you decided to use the VMC.
Tell me about your experience using the VMC.
How often to you access the VMC?
Tell me about any user training you may have provided to Veterans (For Faculty/CDEs/trainees) OR To Faculty/CDEs (For Trainers) Tell me about the training you participated in to learn how to use the VMC. (For Faculty/CDEs/trainee) [probes]
Walk me through how you use the VMC.
Probes: What components, if any, did you find helpful? (Trainees/Faculty)
What components, if any, did you find unhelpful?
What are your goals in using the VMC? (Trainers and Faculty/Trainees)
Have you met your goals?
Tell me about managing your Veterans using the VMC. (Trainees/faculty)
What are your goals in training others to use the VMC?
Have you met your goals? Tell me about your expectations for use of the VMC as part of Veteran management. In what ways, if any, has using the VMC influenced how you interact with your Veterans? (trainees/Faculty) What changes, if any, have you noticed in your Veterans who have been using the VMC? (trainees)
Under what circumstances do you expect to use the VMC? (Faculty)
At this point, would you recommend the VMC to a VA colleague or co-worker? (Faculty)
What would you tell them about it?
What, if anything, could have improved your learning/training experience? (Trainers and Faculty)
Under what circumstances do you expect to use the VMC again? (Faculty/trainees)
Would you recommend the VMC to a VA colleague or co-worker? (Faculty/trainees)
What would you tell them about it?
What, if anything, could have improved your experience? (Trainers and Faculty)
Tell me about other online resources, if any, you have used to help you manage your Veterans’ health. (Trainers and Faculty).
How long have you worked at the VA?
Appendix III. Domain Matrix for Clinical Faculty and Trainers.
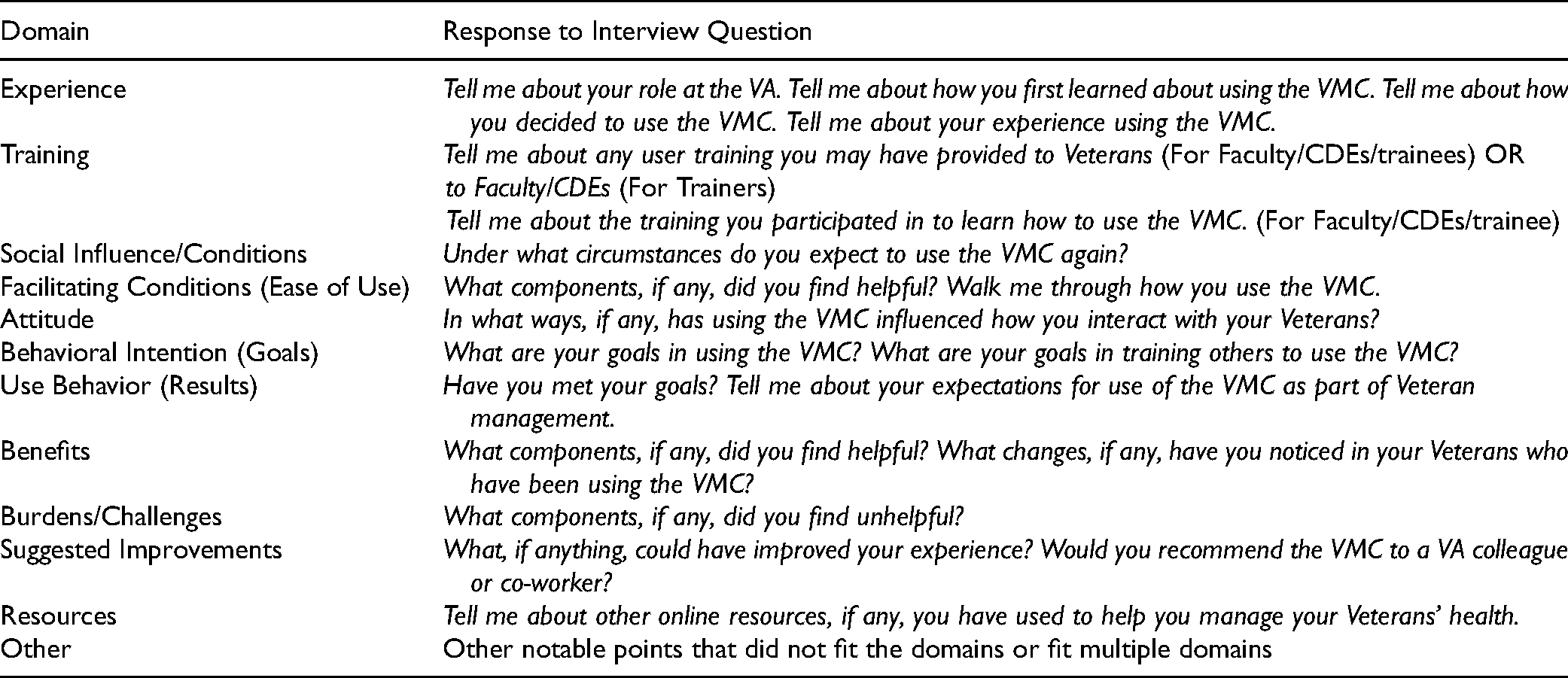
| Domain | Response to Interview Question |
|---|---|
| Experience | Tell me about your role at the VA. Tell me about how you first learned about using the VMC. Tell me about how you decided to use the VMC. Tell me about your experience using the VMC. |
| Training | Tell me about any user training you may have provided to Veterans (For Faculty/CDEs/trainees) OR to Faculty/CDEs (For Trainers) Tell me about the training you participated in to learn how to use the VMC. (For Faculty/CDEs/trainee) |
| Social Influence/Conditions | Under what circumstances do you expect to use the VMC again? |
| Facilitating Conditions (Ease of Use) | What components, if any, did you find helpful? Walk me through how you use the VMC. |
| Attitude | In what ways, if any, has using the VMC influenced how you interact with your Veterans? |
| Behavioral Intention (Goals) | What are your goals in using the VMC? What are your goals in training others to use the VMC? |
| Use Behavior (Results) | Have you met your goals? Tell me about your expectations for use of the VMC as part of Veteran management. |
| Benefits | What components, if any, did you find helpful? What changes, if any, have you noticed in your Veterans who have been using the VMC? |
| Burdens/Challenges | What components, if any, did you find unhelpful? |
| Suggested Improvements | What, if anything, could have improved your experience? Would you recommend the VMC to a VA colleague or co-worker? |
| Resources | Tell me about other online resources, if any, you have used to help you manage your Veterans’ health. |
| Other | Other notable points that did not fit the domains or fit multiple domains |