
Abstract

With the arrival of the COVID-19 pandemic, the Centers for Medicare & Medicaid Services (CMS) expanded its coverage for telehealth services to broaden access to patients while maintaining social distancing efforts. At our institution, one of the challenges involved incorporating telehealth into our inpatient consult service. Different attending physicians rotating on the service had varying understanding of CMS rules, different comfort levels with video visits, and different workflows for rounding. As a result, rounds were often inefficient. Fellows and other learners were frustrated due to inconsistent expectations and guidance from the attending. As a remedy, we developed a standard workflow incorporating telehealth services into our daily inpatient rounds. Our goal was to offer guidance to learners and faculty for navigating a variety of telehealth consults, while continuing to deliver excellent patient care and maintain a culture of learning for learners. This commentary shares a pictorial representation of our workflow with explanations, so that other institutions may benefit from our standardized workflow.
Figure 1 depicts the workflow for the inpatient consult service. The path begins at the upper left corner. The first decision point is whether a face-to-face consult is indicated or desired by the patient or clinician. The indications we used are in the lower right-hand corner. Patients with COVID-19 were managed safely without physically examining the patient when there was a safety issue or a shortage of personal protective equipment. For all patients with a continuous glucose monitor, we used remote monitoring to augment their care.
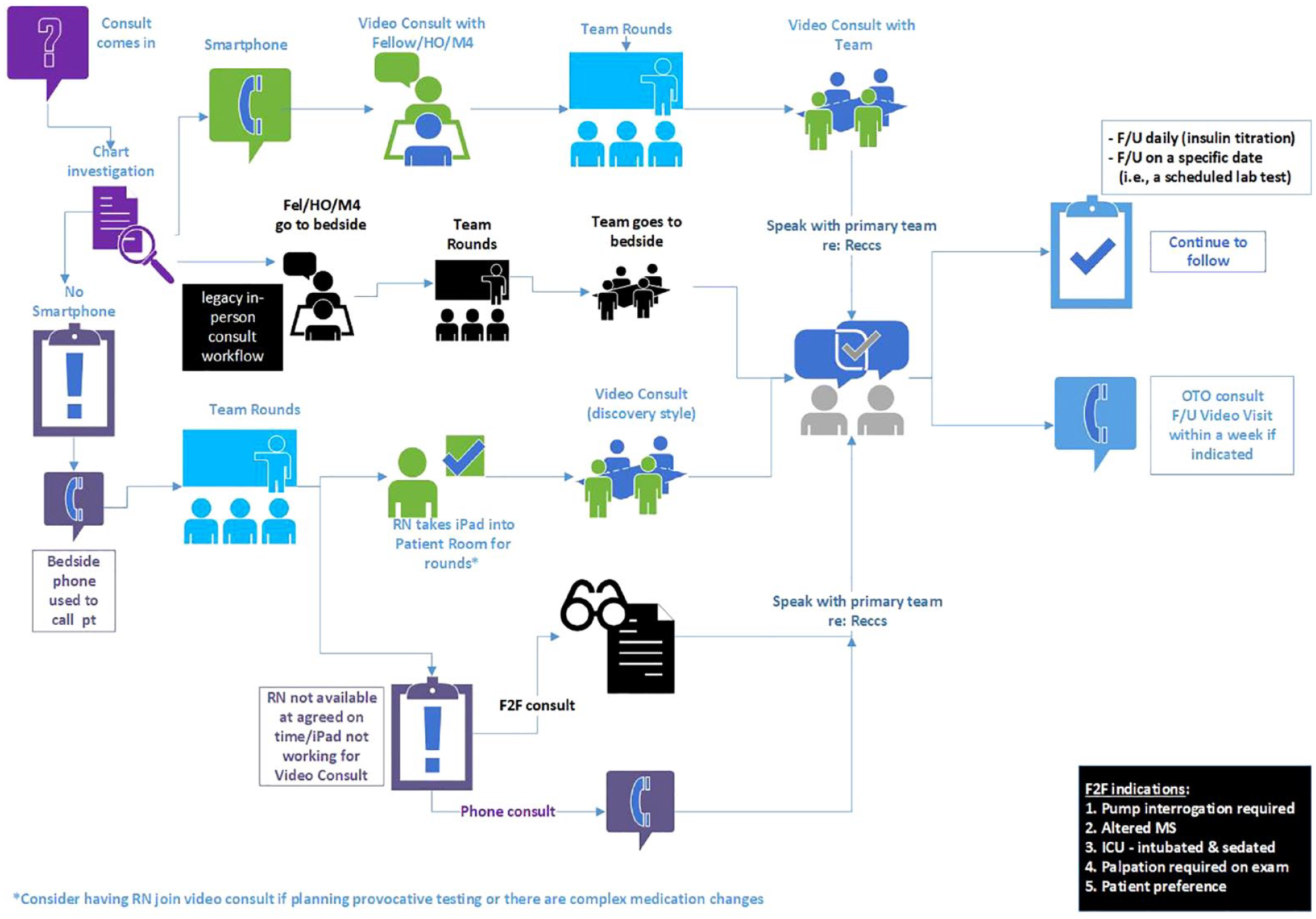
Workflow for inpatient consult service. Abbreviations: HO, house officer; M4, fourth-year medical student; OTO, one time only; CPE, clinical phone encounter.
If a telehealth consult is appropriate, the next step is determining whether the patient has a video-capable smartphone and is willing/able to do a video consultation. If so, the learner does an initial video consult to obtain the history and perform a pertinent virtual physical examination. The full team then meets for in-person rounds and then a second video call is made with the team and attending present.
If the patient does not have a smartphone, there are two options: the patient uses a hospital device with video capability (the ward’s laptop or tablet) or if none is available, an audio-only phone consult is done. If a hospital device is available, the team places a call to the nurse/nurse assistant who assists in establishing the video connection, and the team collects the history and physical together (“discovery rounds”).
We have continued to use this workflow since summer 2020 regardless of the number of COVID patients in our hospital, as telehealth has remained a part of delivering more and better care for patients with diabetes. Our experience has been that patients with diabetes are more comfortable with virtual care in the hospital, give richer histories, and are more open to recommendations. Our hypothesis is that since the physical presence of a large team at the bedside may be anxiety provoking for patients, they are more at ease and feel safer sharing more details during a video consult as opposed to in person.
Footnotes
Abbreviation
CMS, Centers for Medicare & Medicaid Services.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.