
Abstract
Background:
Rates of diabetes for veterans who receive health care through the Veterans Health Administration are higher than rates in the general population. Furthermore, many veterans live in rural locations, far from Veterans Affairs (VA) hospitals, thus limiting their ability to readily seek face-to-face endocrinology care for diabetes. Telehealth (TH) technologies present an opportunity to improve access to specialty diabetes care for such patients; however, there is a lack of evidence regarding the ability of TH to improve glycemic control in comparison to traditional face-to-face consultations.
Methods:
This was a retrospective cohort study of all new endocrinology diabetes consultations at the Denver VA Medical Center over a 1-year period.
Results:
A total of 189 patients were included in the analysis. In all, 85 patients had received face-to-face (FTF) endocrinology consultation for diabetes and 104 patients had received TH consultation. Subjects were mostly males (94.7%) and the mean age was 62.8 ± 10.1 years old. HbA1c improved from 9.76% (9.40% to 10.11%) to 8.55% (8.20% to 8.91%) (P < .0001) for the TH group and from 9.56% (9.16% to 9.95%) to 8.62% (8.22% to 9.01%) (P < .0001) for the FTF group after 1 visit. This change in HbA1c was not significantly different in the TH and FTF groups (P = .24). TH visits were associated with a hypothetical savings in median distance traveled of 231.2 miles per trip (which equates to $94.79 saved per trip).
Conclusions:
Endocrinology TH consultations improved short-term glycemic control as effectively as traditional FTF visits in a veteran population with diabetes.
In 2012, 9.3% of the US population (29.1 million individuals) had diabetes and the disease ranked as the 7th leading cause of death. 1 The diabetes burden is even greater in the Veterans Health Administration (VHA), the nation’s largest integrated health care system, where at least 20% of veterans have diabetes. 2 As of August 2015, 22.8% of veterans with diabetes were considered “uncontrolled” having HbA1c values greater than 9% (from internal VA data). A significant challenge to achieving better diabetes control within the VHA system is that 3.2 million veterans—36% of the total veteran population—live in rural communities where access to specialty care is often limited. 3 Recognizing the need to incorporate new technologies to improve timely care delivery, the US Department of Veterans Affairs (VA) invested $90 million in its telehealth (TH) expansion plan in 2011. 4
TH is a broad term, encompassing telemedicine and mobile health technologies used for physician-patient interactions, diagnostics, care delivery, education, information sharing, monitoring, and reminders. 5 Currently up to 50% of US hospitals have some form of active TH program 6 and up to 57% or providers surveyed are willing to see patients over video. 7 A 2013 Cisco survey found that greater than 70% of patients are comfortable communicating with doctors via texting, email, or video instead of being seen in person, suggesting that TH services will continue to expand. 8 However, despite escalating use and good acceptance amongst providers and patients, TH care faces substantial barriers such as state-by-state variability in TH reimbursement, medical license portability, and privacy issues.9-11 Furthermore, evidence is currently insufficient to determine the ability of TH interventions to reduce overall cardiovascular disease risk, but a study is under way to address this issue.12,13
While TH holds great promise for improving access and delivery of care, there has been a call for further investigation into whether TH delivers similar outcomes as traditional face-to-face (FTF) encounters (ie, usual care) at either the same or lower costs. 14 This study’s purpose was to investigate the impact of TH versus FTF endocrinology consultations on glycemic control for veterans referred for diabetes evaluation. We hypothesized that improvement in glycemic control would be similar in patients receiving care through TH as compared to those seen by FTF.
Methods
We performed a retrospective cohort study of all new endocrinology diabetes consultations at the Denver VA Medical Center (DVAMC) between October 1, 2013, and September 30, 2014. Consults were identified in VA’s Computerized Patient Records System (CPRS) by using ICD-9 codes. The local institutional review board, the Colorado Multiple Institutional Review Board, approved the study prior to data collection.
Patients who had not been seen by endocrinology providers for 2 years prior to the visit were considered to be new consultations. Selection for either FTF or TH care took place during the course of routine primary care and was offered to patients who lived far from the DVAMC. The primary care providers placed a consult depending on the patients’ preference. Primary care providers were responsible for explaining the process of TH to the patients. Figure 1 outlines the breakdown of the number of patients in each care delivery modality and reasons for exclusion. A total of 250 initial diabetes consultations within the aforementioned time period were identified. Of these patients 119 received FTF consultations and 131 received TH visits depending on their distance to DVAMC. Sixteen patients from the FTF group and 7 patients from the TH group were excluded for the reasons listed in Figure 1. To compare the effects of different methods of care delivery on glycemia, subjects who received both TH and FTF care (“mixed visit modalities”) were excluded in this analysis. Eighteen patients in the FTF group and 20 patients in the TH group were then excluded because no follow-up HbA1c value was available. The majority of patients received either TH or FTF consultation with 1 of the 3 nurse practitioners (NP) in the Division of Endocrinology at DVAMC. Each NP had extensive prior training in diabetes and had been providing diabetes care at the Denver VA for a minimum of 2 years. All NPs provided both FTF and TH care.
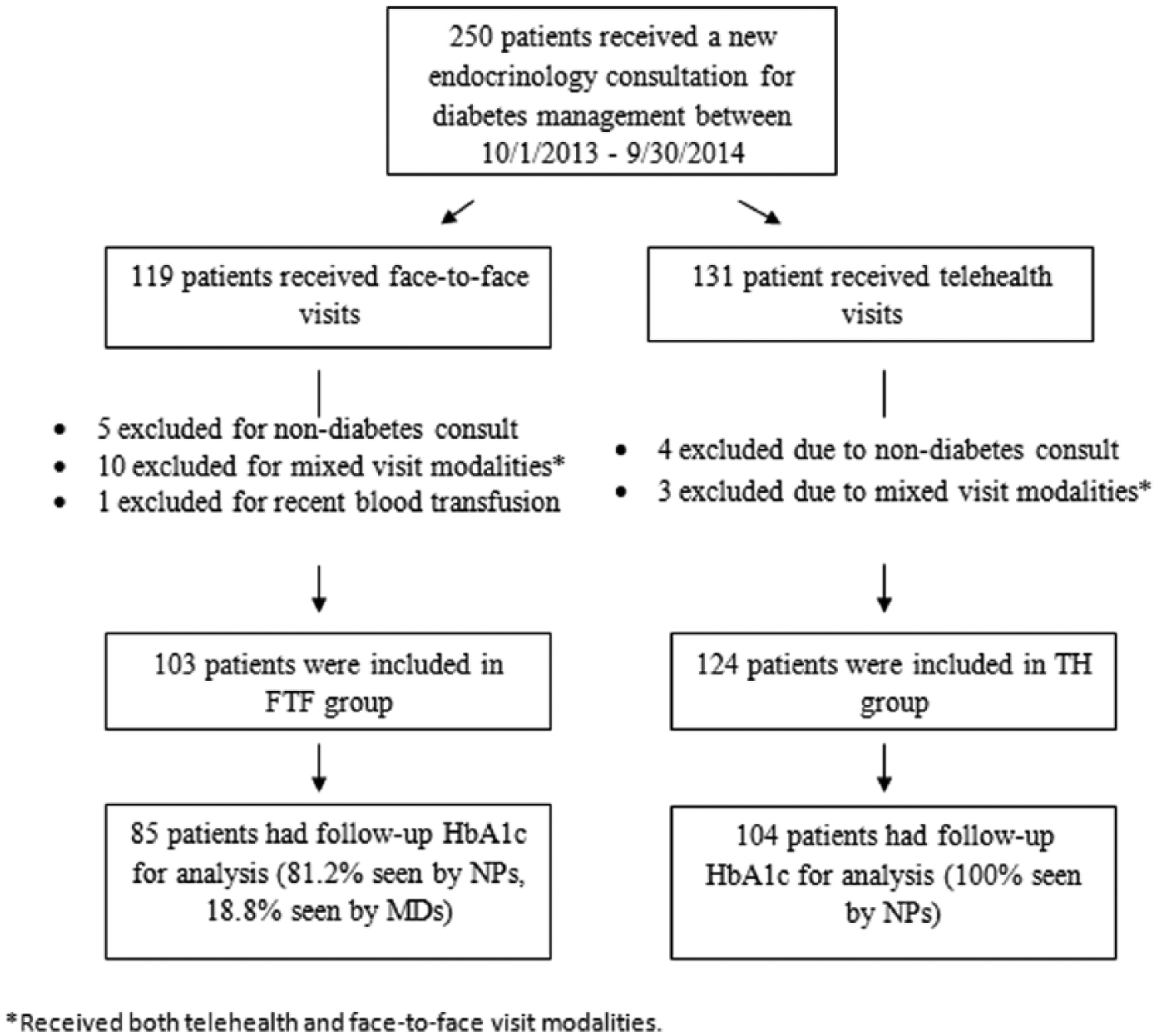
Number of patients in each care delivery modality and reasons for exclusion. Received both telehealth and face-to-face visit modalities.
Patients in the FTF group traveled to the DVAMC endocrinology clinic for their diabetes care, whereas TH patients traveled to their local primary care clinic for real-time video consultation. During both FTF and TH consultations, routine diabetes care was carried out in accordance with current American Diabetes Association (ADA) guidelines. The follow-up visits were scheduled by the provider depending on the perceived needs of each patient (ie, generally every 3-6 months).
Upon arrival to the local primary care clinic, those receiving TH care were placed in a private clinic room, vitals were checked, and home glucometer readings were downloaded. Patients were then assisted by either a nurse or trained TH tech to establish a video connection with the endocrine provider in Denver. TH technologies used at the primary care clinics were Global Med Education or Primary Care Cart videoconference units. Endocrinology providers at DVAMC used either a Tandberg 1700 or Tandberg MOVI camera with secured VLAN lines. Providers used close-up cameras to present educational materials from their desktops and demonstrate techniques for using blood glucose meters, insulin pens and syringes, and injection site selection. A stethoscope and otoscope were also available for use. Patients in the TH cohort received laboratory and screening tests such as dilated eye exams and monofilament testing at their local clinics. In contrast to FTF care, providers in TH visits had limited ability in performing comprehensive physical examination. Patient-related data was extracted from individual medical records in CPRS. Baseline patient characteristics are illustrated in Table 1. Providers at the DVAMC provided TH services to veterans at 18 primary clinics in Colorado, Wyoming, Montana, and Idaho (Figure 2).
Patient Baseline Characteristics (N = 189)
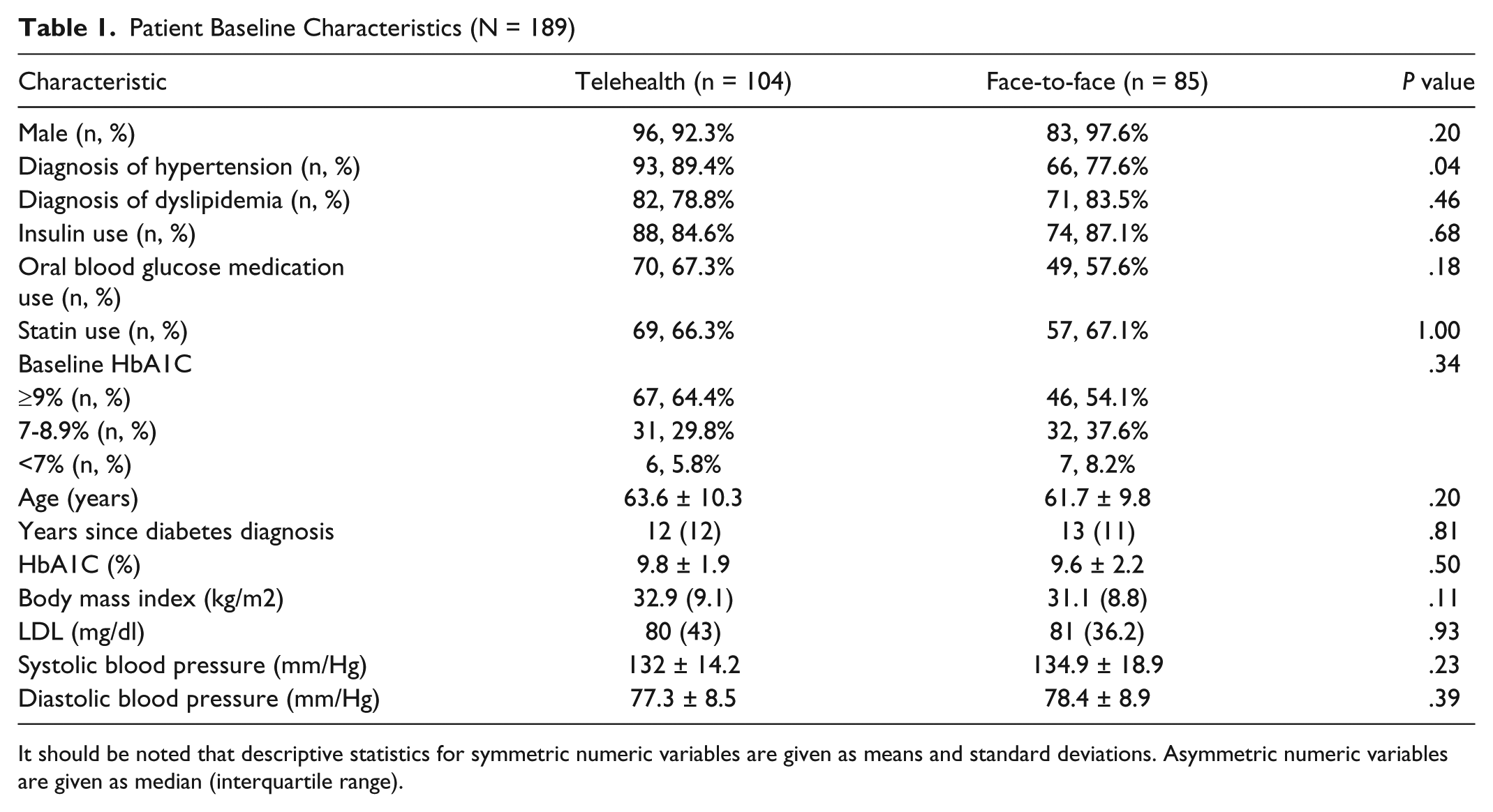
It should be noted that descriptive statistics for symmetric numeric variables are given as means and standard deviations. Asymmetric numeric variables are given as median (interquartile range).
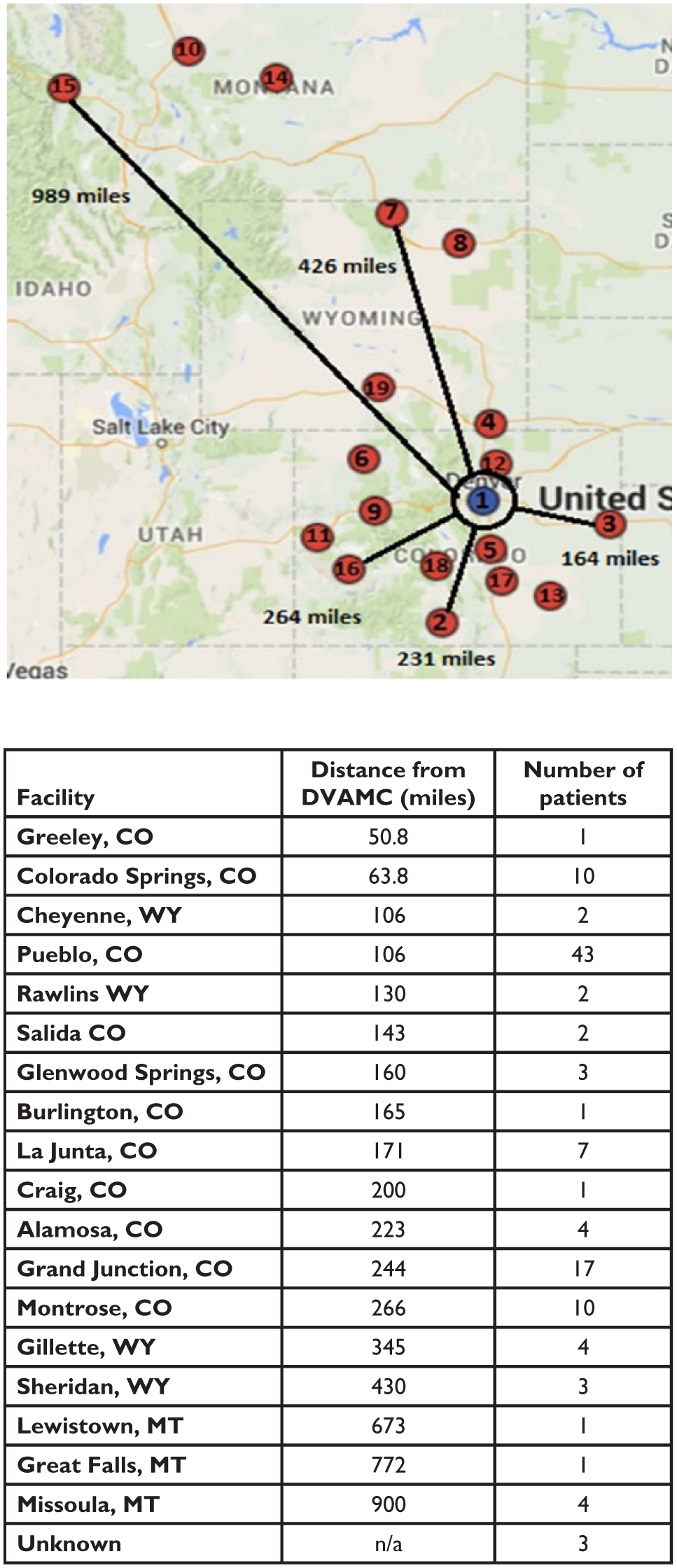
Map showing Denver VA Medical Center (1) and outlying community clinics (2-19) where telehealth visits were performed. The distance of community clinics from Denver VA and the number of patients from each clinic are summarized in the table.
Statistical Analysis
For baseline characteristics (Table 1), Student’s t-test was used to compare continuous variables and Fisher’s exact test was used to compare categorical variables between groups. A linear mixed regression model was used to model the effects of baseline HbA1c, age, visit type, and visit number on HbA1c change from baseline. Random intercepts were included for provider. An AR(1) structure was used to model the covariance in HbA1c change from baseline across visits. Several functional forms for the trend across visits were explored, including linear, quadratic, cubic, and categorical. However, the shapes of the curves in Figure 3 suggest a model that estimates the initial change in HbA1c from baseline to visit 1, then fits a linear trend for subsequent visits. By fitting a model with a linear time trend that treats visit 1 as time 0, the effects of each of the covariates on the intercept give the covariate effects on the initial drop in HbA1c from baseline to visit 1. By including interactions between each of the covariates and a linear “subsequent visit” time variable, the effects of covariates on the subsequent linear trend were modeled. While the inclusion of a baseline covariate in a change from baseline model can result in the attenuation of the treatment effect due to regression to the mean when the treatment groups differ on baseline scores, the TH and FTF groups showed negligible difference in baseline HbA1c (mean baseline HbA1c = 9.76 and 9.56, respectively; P = .5051; see Table 1), negating this concern for our data and model.
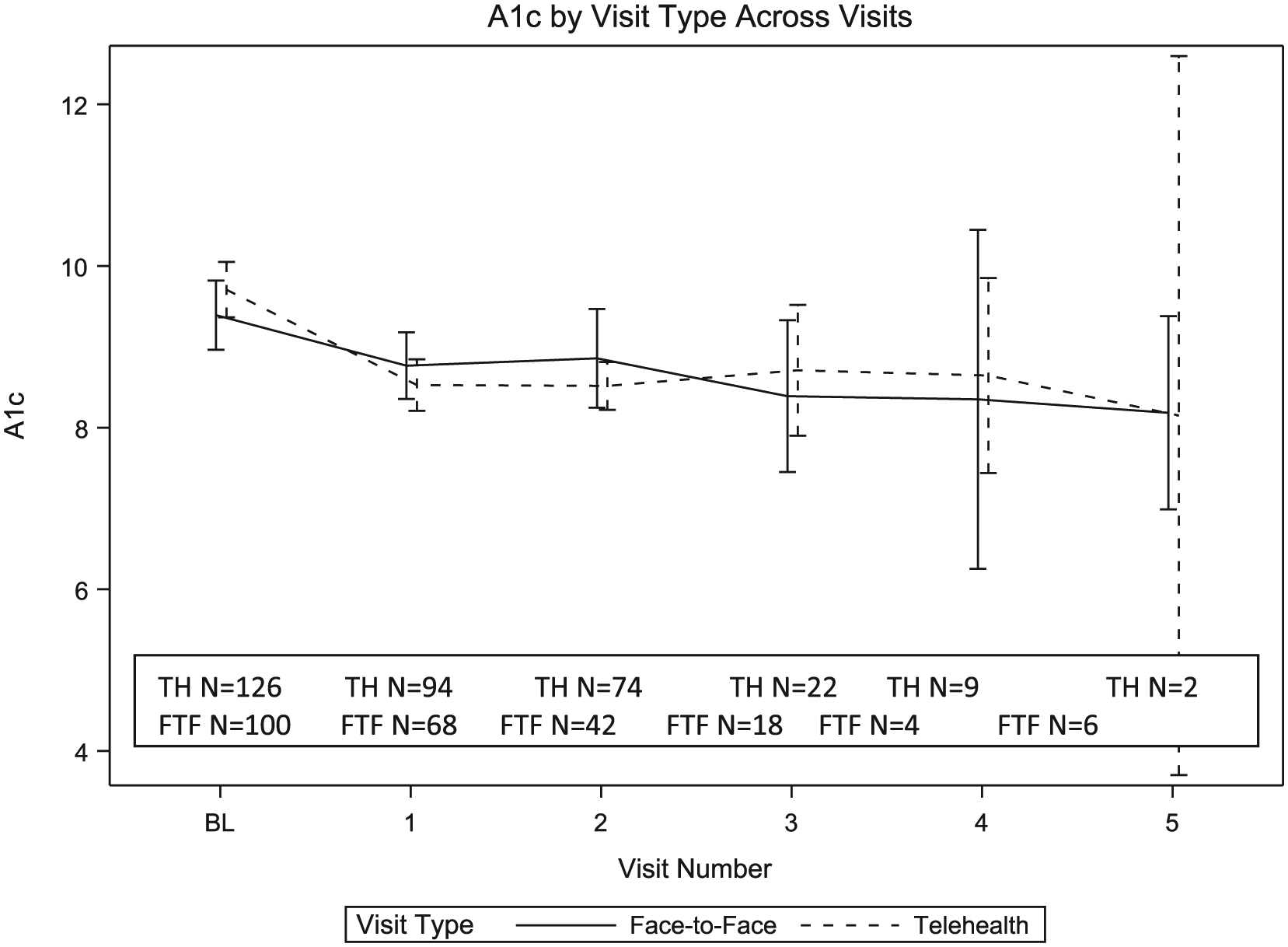
Means and 95% confidence intervals for HbA1c by visit type across visits show estimated HbA1c change from baseline by treatment group.
For each patient Google Maps was used to calculate the distance traveled to receive care. At least 1 TH visit was delivered to 18 different outpatient clinics. Home addresses were available for most subjects, but when only a PO box address was available, the “home address” used was the automatically generated address that is created when only a town name (and not a specific address) is entered into Google Maps. For the TH group, round trip mileage was the distance between home and the local outpatient clinic where they received TH services. For the FTF group round trip mileage was the distance between home and the DVAMC.
Results
Subjects were comprised of mostly males (94.7%), reflecting the norm for a veteran population, and their mean age was 62.8 ± 10.1 years. The mean baseline HbA1c prior to the initial consultation visit was 9.7 ± 2.1% and similar between the 2 groups. The only statistically significant difference between the 2 groups was that the TH group had a higher prevalence of hypertension (Table 1).
Figure 3 shows group means and 95% confidence intervals for HbA1c across visits. Note that this plot only gives mean estimates by group and does not reflect the estimates of the linear mixed model, nor does it take other covariates into account, such as baseline HbA1c. There appears to be an initial drop in HbA1c from baseline to visit 1 in both groups, followed by a flat linear trend. This provided the motivation for estimating the change from baseline to visit 1 separately from the subsequent trend in the linear mixed model.
HbA1c improved from 9.76% (9.40% to 10.11%) to 8.55% (8.20% to 8.91%) (P < .0001) for the TH group and from 9.56% (9.16% to 9.95%) to 8.62% (8.22% to 9.01%) (P < .0001) for the FTF group (Figure 4) at the first follow up visit. In other words, the estimated drop in HbA1c from baseline to visit 1 in the TH group was 0.277 percentage points greater than the drop in HbA1c from baseline to visit 1 in the FTF group (95% CI: 0.741 percentage points greater drop to 0.186 percentage points lesser drop). In addition, the percentage of patients with poorly controlled diabetes (defined as HbA1c ≥ 9%) decreased from 64.4% to 35.6% in TH group and from 54.2% to 27.1% in FTF group.
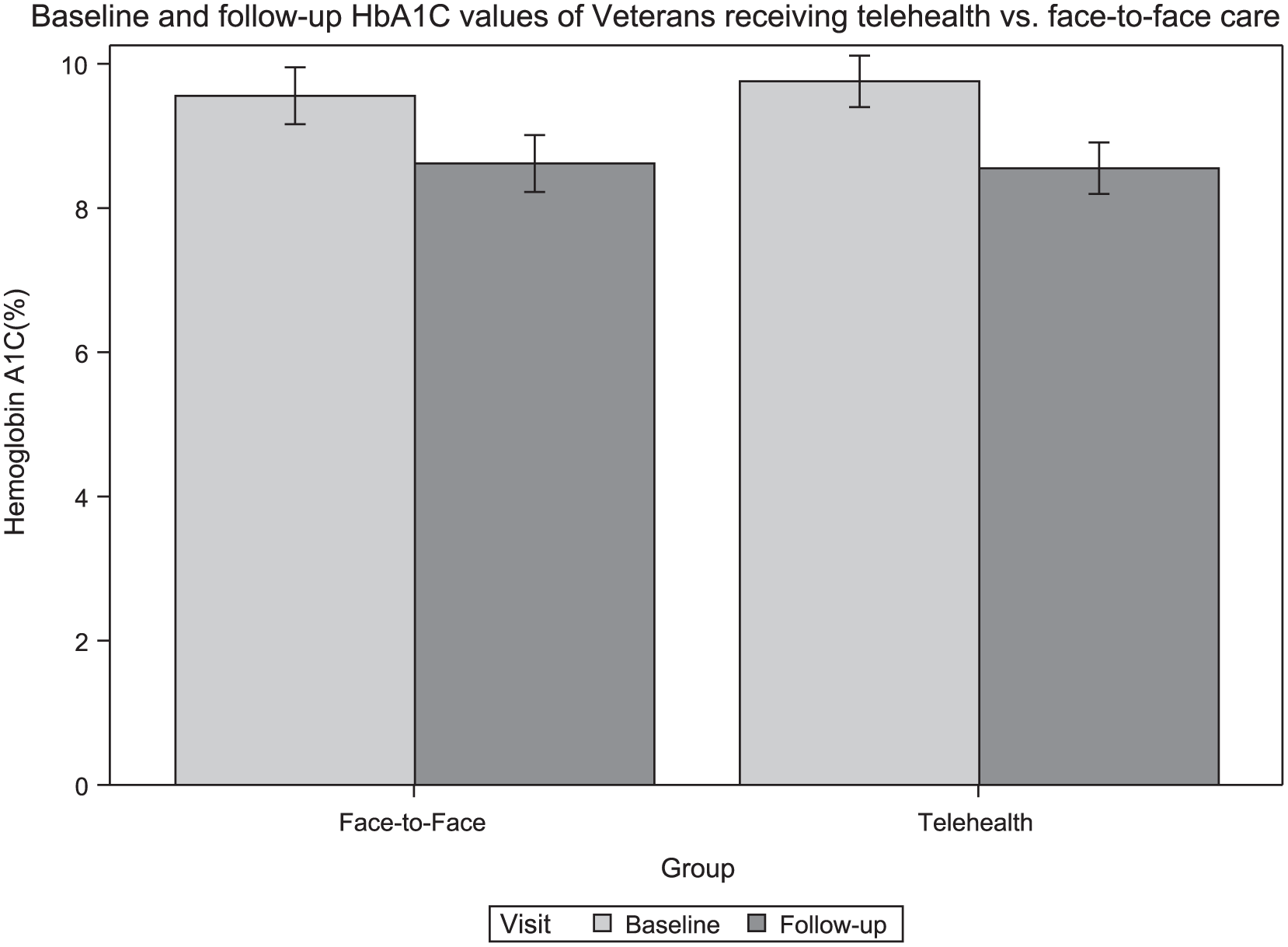
Initial and follow-up HbA1c levels of telehealth and face-to-face groups.
Those patients with higher baseline HbA1c saw a greater decrease in HbA1c from baseline to visit 1. For every additional percentage point of baseline HbA1c, the initial drop was 0.645 percentage points greater (95% CI: 0.532 to 0.758 percentage point drop, P < .0001). Importantly, the change in HbA1c from baseline to visit 1 was not significantly different in the TH and FTF groups (P = .2397). Also, there was no significant effect of age on HbA1c change from baseline across all time points (P = .8681).
The TH group’s round-trip distance traveled was reduced by a median of 231.2 miles per patient visit as calculated using Google Maps (Figure 5). Since the DVAMC currently compensates patients $0.41 for every mile traveled to care, this hypothetically equates to approximately $94.79 savings per patient visit (based on miles saved if TH patients had traveled to DVAMC instead of TH facility).
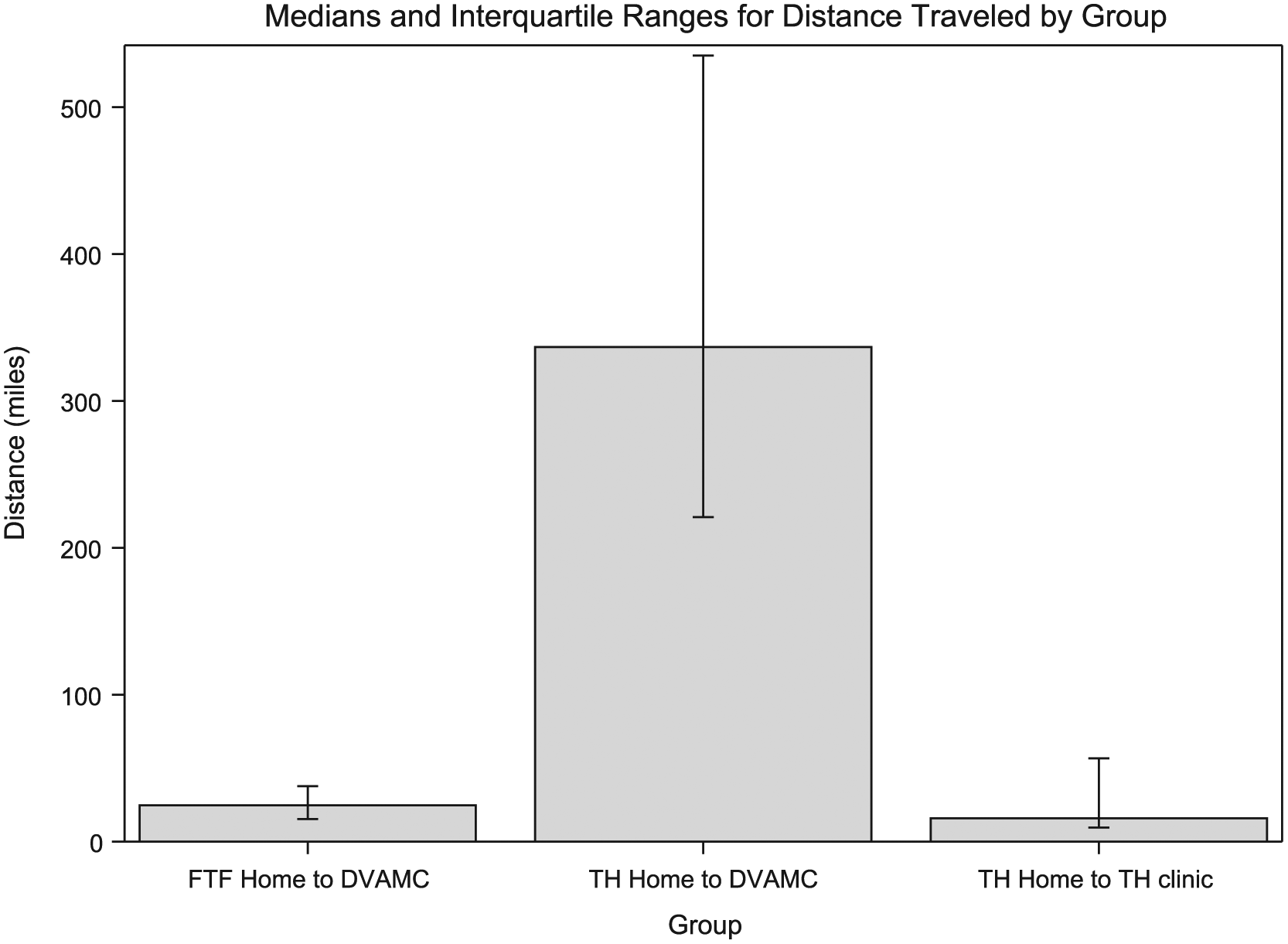
Median miles traveled for diabetes care in the FTF group (FTF home to DVAMC), the TH group (TH home to TH clinic), and a group representing the hypothetical situation where TH participants travelled to DVAMC instead of receiving care at their local TH clinic (TH home to DVAMC).
Discussion
A large number of veterans with diabetes fail to meet goals for glycemic control and a lack of access to specialty care may be a contributor to this issue. The VA has spearheaded the use of TH care to improve specialty care access; however, scant published data is available regarding the efficacy of diabetes care provided by TH as compared to usual care within the VA system. In this retrospective study, we found that diabetes TH consultations for VA patients with poorly controlled diabetes were similar to traditional FTF endocrinology visits in their ability to improve short-term glycemic control. This study also showed that endocrine consultation via TH saved travel time and cost for patients. The rate of patient satisfaction in TH as compared to FTF group was also similar in a larger cohort of patients (not specific to endocrinology) in our institution (data not shown).
This study is unique because of its focus on subspecialty TH versus usual FTF diabetes care provided to veterans within the VA system; however, previous studies also supported the efficacy of TH on diabetes outcomes in other health care settings. A meta-analysis of 35 randomized controlled trials (RCTs) employing a heterogeneous selection of TH interventions revealed a significant, albeit slight, decrease in HbA1c in the intervention group compared to the control group. 15 In a recent Cochrane Database systematic review that only considered RCTs of interactive TH interventions that involved direct patient-provider interaction and was delivered in addition to, or substituting for, usual care compared with usual care alone found that in studies recruiting participants with diabetes (16 studies, N = 2768) those allocated to TH had lower HbA1c values (mean difference -0.31, 95% CI -0.37 to -0.24; p <0.00001) at a median of 9 months of follow-up. 16
Our findings also demonstrated that a single endocrinology consultation (independent of the modality) improved glycemic control and decreased the percentage of patients who had poorly controlled diabetes. While VA performance measures advocate for targeted HbA1c levels after assessment of microvascular complications, major comorbidities, and life expectancy, achieving HbA1c values that are at least less than 9% is considered a universal goal. 17 Our findings therefore suggest that TH endocrine consultations have the potential to markedly improve glycemic quality measures for rural veterans with limited access to FTF endocrine care.
Although a detailed analysis of overall cost savings was not performed in this study, we did find that decreased travel alone led to a savings of approximately $94.79 per patient per TH visit. While several VA TH studies have noted cost savings from decreased travel,18-20 in general, cost-effectiveness studies of TH care have yielded inconsistent findings and conflicting evidence. 5 With regards to TH care for type 2 diabetes, a recent meta-analysis found that only 2 of 35 studies included assessment of cost-effectiveness. 15 Clearly more robust economic analyses of TH care are needed. 14 Future cost-effectiveness studies of TH diabetes care should focus on such items as medication usage and adherence, outpatient visit frequency, hospital admissions, and emergency department visits.
This study has limitations that serve as opportunities for future studies. First, the retrospective cohort design is inherently nonrandomized. While the analyses presented indicate that there were no meaningful differences between the TH and FTF visits in their ability to improve short-term glycemic control, one cannot exclude nonrandom effects that have not been specifically assessed. In addition, this study was not designed to compare long-term changes in glycemic control between FTF and TH patients. Although we found short-term improvements in glycemic control, recidivism to an uncontrolled state is known to be a common problem in the management of other chronic conditions such as hypertension. 21 Thus, there is a need for longitudinal studies of TH care for diabetes with a follow-up period of several years. Our study focused only on changes in glycemic control and not on other measures that constitute truly comprehensive diabetes care. Future studies should analyze non-HbA1c outcomes such as hypoglycemia, the rate of screening for diabetes complications, and the appropriate use of other medications such as statins. Our sample size was not large enough to yield meaningful subgroup analyses; therefore we were unable to identify which subpopulations might benefit most from TH care. Last, a small number of patients included in the study did not have uncontrolled diabetes at the time of referral to endocrinology, but rather consultation was requested for management of certain VA nonformulary diabetes medications (ie, U-500 insulin or GLP-1 agonists), for insulin pump management, or for management of hypoglycemia. Such patients likely received unmeasured benefits from endocrinology consultation that go beyond simple HbA1c measurement.
In summary, endocrinology TH consultations improved short-term glycemic control as effectively as traditional FTF visits in a veteran population with diabetes with potential financial benefits for patients and the health care system.
Footnotes
Acknowledgements
Michael P. Ho, MD, PhD, Amy Diesburg-Stanwood, FNP-BC, ND, Christina Cunningham, ANP-BC, and the rest of the Denver VA Endocrinology medical staff.
Abbreviations
ADA, American Diabetes Association; CPRS, Computerized Patient Records System; DVAMC, Denver VA Medical Center; FTF, face-to-face; HbA1c, hemoglobin A1c; NP, nurse practitioner; RCT, randomized controlled trial; TH, telehealth; VA, Veterans Affairs; VHA, Veterans Health Administration;
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: BERD Seed grant supported by CCTSI UL1 grant.