
Abstract
In 2018, the Veterans Health Administration (VHA) established the original 19 Headache Centers of Excellence (HCoE) program, and an evaluation center. This study utilized a Veteran engagement group method to elicit input from Veteran patients living with chronic headache on daily needs, social determinants of health, and preferences and suggestions for headache programs, services, and research priorities. Four engagement groups were conducted between July 13th and August 22nd of 2022 with Veterans who experience headache and received care at a VHA HCoE. Engagement groups were audio-recorded, de-identified, transcribed, and analyzed using rapid qualitative content matrix analysis. Participants also completed a baseline survey on demographics, technology use, headache history, and health. Patients perceived care coordination, social support, gender specific preferences and access to complementary and integrative therapies to be important aspects of headache care delivered by HCoEs. Participants expressed strong interest in effective, interactive peer support groups to share and learn from each other's experiences with headaches and treatments. Findings underscore the demand for coordinated, interdisciplinary headache care integrating complementary health approaches and addressing gender-specific needs.
Introduction
Headache is a common and pervasive neurological condition among Veterans with a high worldwide lifetime prevalence. 1 Several studies have investigated the expressed experience of individuals with headache disease2,3 and barriers to navigating headache care services. 4 There remains a need for research to further discern what Veteran patients prefer and require from headache specialists.
The Veterans Health Administration (VHA) established a national Headache Centers of Excellence (HCoE) program in 2018, which included 19 clinical sites and one Research, Education, Evaluation, and Engagement Activities Center for Headache (RE3ACH) during this study to address the high prevalence of headache among Veteran populations. HCoEs aim to engage Veterans in research to understand headache necessities and preferences. Prior HCoE RE3ACH qualitative analyses revealed that Veterans struggled to navigate the healthcare system to access evidence-based headache care. 4 Incorporating Veteran patient perspectives is critical to understanding best practices for implementation of clinical headache programs and research. Utilizing a Veteran engagement group (VEG) method, 5 we established the ACTIvated Veterans Engagement (ACTIVE) group to elicit patient input on daily needs and social determinants of health, suggestions for HCoE programs and services to assist Veterans living with headache, and feedback on HCoE-related research. By partnering with a nationally diverse sample of Veterans with headache through the establishment of ACTIVE for Headache, we aimed to develop Veteran stakeholder groups to elicit stakeholder preferences, and to inform optimal implementation of clinical programs.
Furthermore, in an effort to move away from “damage-centered” research aimed at documenting participants’ pain and suffering, and instead move towards a “desire-based framework” to capture Veterans’ wisdom about and hopes for their headache care, 6 we seek to recenter Veterans and their wishes for headache care services that address their expressed exigencies.
Methods
Design
Veterans currently receiving headache care within a VHA HCoE were purposively recruited by provider referral. Prospective participants were sent a recruitment letter and study information sheet via mail. Next, research staff attempted contact up to 3 times via telephone. Of the 19 HCoE sites contacted, we received 91 referrals from 8 HCoE sites located across the US. We recruited and consented 23 Veterans from these 8 HCoEs who have a headache diagnosis and received HCoE headache care. We utilized a mixed methods approach engaging participants in surveys and groups. Enrolled patients were invited to participate in virtual engagement groups to engage in discussion about their healthcare needs and services they would like HCoEs to provide.
Results
Quantitative Data
Demographic Data Self-Reported by Engagement Group Participants a .
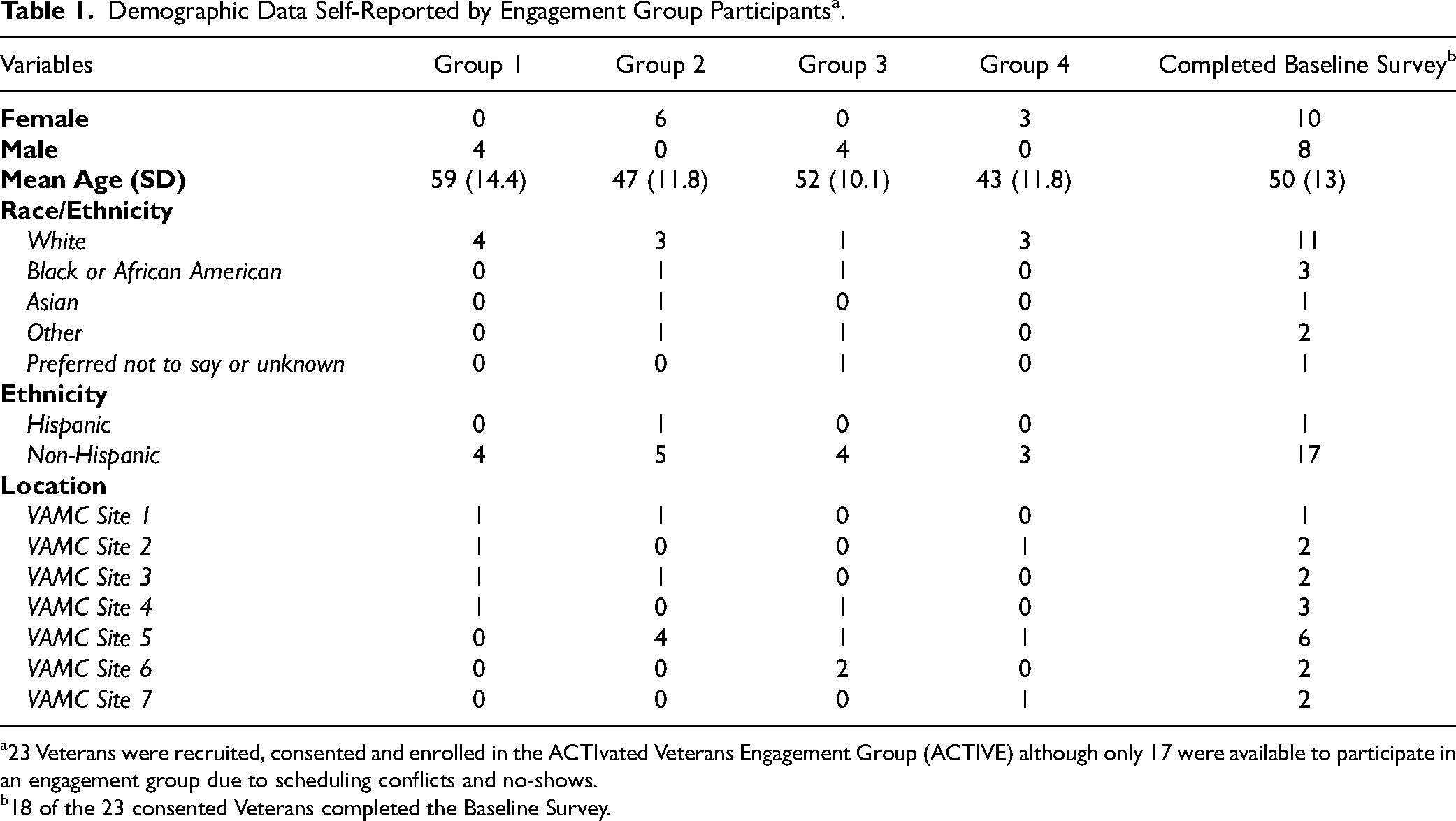
23 Veterans were recruited, consented and enrolled in the ACTIvated Veterans Engagement Group (ACTIVE) although only 17 were available to participate in an engagement group due to scheduling conflicts and no-shows.
18 of the 23 consented Veterans completed the Baseline Survey.
“So, I'm, like I said, at the beginning stages of figuring out what to do about it. So. I'm, learning now from you guys.” [ID 08–01] “And you know it took me a while to get there, but I can kind of feel like, oh, you know, my neck is tensing up, something's tensing up. OK, I’ve got to take a break, and I just kind of have to get away, especially like at work and just kind of get away from all of the BS out there and just kind of calm down… it does make the rest of the day just that much easier and that, you know, helps a lot for me.” [ID 14–03]
See Table 2 for demographics, headache experience, and healthcare utilization.
Self-Reported Demographics, Headache Types and Other Comorbidities, and Healthcare Utilization.

Note: Some survey responses may be missing or incomplete due to non-responses, participants opting out, or other data collection issues.
Engagement Groups - Thematic Content Analysis
We conducted engagement groups with 17 of the 23 enrolled Veterans receiving headache care across VHA divided among 4 groups. The semi-structured engagement groups consisted of two female groups (n = 6 women in one group, n = 3 women in the other) and two male groups (n = 4 men in one group, n = 4 men in the other). The 17 participants (9 women, 8 men) had a mean age of 50 years (SD = 12) and the majority of participants were White (n = 10), and non-Hispanic (n = 16). See Table 1.
Four topics emerged from the qualitative analysis: (1) Care coordination needs and suggestions; (2) Support groups and family education interest; (3) Nonpharmacologic care interest and suggestions based on complementary integrated health received; (4) Gender-specific insights and barriers to care. See Figure 1. The following themes were identified within each topic.

Major topics and associated themes with illustrative quotes from our qualitative analysis of the ACTIvated veterans engagement group.
Ideas offered to improve care coordination included streamlined communication with providers via MyHealtheVet (ie, electronic, asynchronous, secure patient-provider messaging tool), 9 having the ability to send headache journal data straight to providers to have an accountability partner, and recording an “origin story” video with headache history and background that would live in their medical chart.
Men Veterans also expressed ways in which they feel their gender and military training exacerbates their struggle to manage headache pain socially. They discussed ways in which their military training and social role expectation as men have taught them to be tough and hide pain, which results in difficulty admit pain and delays care-seeking.
Discussion
Through our establishment of Veteran engagement groups offered by a national VA headache research consortium, Veteran groups shared their experiences living with headache and suggestions for future clinical and research focus topics. Results indicate most Veteran participants had suffered from headache disease for three or more years, and had seen multiple providers for their headache disease while seeking relief. Generally, they described their headache care navigation journey as complex in a variety of ways. These findings are consistent with previous results where Veterans reported the long-term journey of headache care starting with DoD and transitioning out to community care and into the VHA seeking symptom relief. 4
Our Veteran participants with headache disease described difficulties finding specialized headache care due to inadequacies in care coordination between providers and services that patients with headache see prior to visits with headache specialists. Based on Veteran participant feedback, satisfactory care coordination might involve implementing technological solutions that facilitate seamless communication between primary care and headache specialty care services, reducing the need for repetitive information sharing, and enhancing the continuity of care. Overall, our findings support a need for coordinated headache management across services and exploration into the proposed solutions. Previous research demonstrates coordinated headache management significantly improves outcomes for patients who have substantial unmet needs and proposed a coordinated headache management program consisting of patient education, diagnosis, and treatment by a professional trained in headache, and proactive case management follow up. 10 The VA HCoEs provide a coordinated headache program with trained headache specialists. Perhaps future efforts would expand this coordinated care into primary care and other services.
Further, as Lindsey et al (2023) proposed, a better-defined headache care pathway from primary care to headache specialty care may especially help facilitate appropriate referrals and make healthcare navigation easier for patients with headache diseases. A previous qualitative study from our research group found that headache neurologists emphasized their specialty represents only one component of the comprehensive care required to effectively treat patients with chronic headaches, and they advocated for treatment to be delivered through a comprehensive, multidisciplinary center to best meet patients’ needs. 11 Similarly, Veterans in our engagement groups expressed a preference for a coordinated care approach where multiple specialists work together under one umbrella. Endorsed by neurology specialists and Veterans alike, this approach may prevent the frustration of Veterans repeating their medical history to each new provider and ensure a smoother referral process through continuity of shared information.
Consistent with Kuruvilla et al,
12
our participants expressed a strong desire for a more holistic approach to headache management that considers a range of non-pharmaceutical interventions to effectively meet individual needs. They highlighted a variety of complementary and integrative therapies they believe could benefit their headache management including biofeedback
Our findings indicate that understanding and addressing gender-specific insights in headache care for Veterans involves believing and validating women's pain experiences, providing sensitivity training to healthcare providers and administrative personnel, and recognizing the impact of military training and social expectations on men's willingness to seek headache care. Existing literature demonstrates gender bias in pain treatment as part of the patient-provider encounter and the extent to which minority patients’ pain is often undertreated and has led patients to mistrust our healthcare system.13–15 Specifically, findings indicate women with chronic pain struggle for legitimacy, and report being mistrusted and psychologized by health care providers. 13 Women expressed feeling invisible and stressed the need for healthcare providers to listen attentively and take their pain seriously from their past experiences. Proposed solutions included sensitivity training for healthcare providers and administrative personnel to improve understanding and responsiveness to women's pain concerns. Women also appreciated the supportive environment of women-only healthcare settings and groups, which fostered a sense of validation and community. Previous studies also showed many women Veterans preferred gender-specific health care settings and suggest providing them with options to choose female providers, providing training in gender-sensitive care, offering women-only groups/spaces, and locating pain care within women's clinics when possible. 16
Veteran men highlighted how their gender and military training contribute to their challenges in managing headache pain. Military culture often emphasizes toughness and stoicism, which can lead to reluctance to admitting pain and delays in seeking care.17,18 This social expectation to “tough it out” can exacerbate their struggles with pain management. Healthcare providers were encouraged to be mindful of these cultural influences and to adopt a more sensitive approach when working with male-identifying veterans, ensuring that their unique barriers to seeking and receiving care are addressed effectively. Also prior research has found that men are often less inclined to seek assistance for headache disorders and other medical conditions compared to women. 19 This reluctance is attributed to a desire for autonomy and control, a lack of recognition of their own health needs, and adherence to traditional gender role norms.19–21
Both men and women in our study expressed a strong interest in effective, interactive peer support groups facilitated or monitored by professionals to share and learn from each other's experiences with headaches and treatments. Overall, Veterans underscored the critical role of peer support in coping with headaches, emphasizing the need for structured, professionally facilitated groups and educational initiatives aimed at increasing understanding and support from their social circles. This desire for support is consistent with existing research underscoring the prevalence of poor social support and loneliness among those with chronic headache. 22
Strengths & Limitations
This study consists of a limited sample size from approximately one-third of the HCoEs in the US. However, our sample is from multiple centers across the US and includes both men and women and a diverse patient sample. Previous research outside of the VA has reported larger proportions of women in their samples. 23 Overall, this study's direct elicitation of feedback from Veterans grounds our findings in the real experiences of those the HCoEs aim to serve. Our findings also highlight common challenges faced by the broader Veteran population, with participants reflecting on their experiences navigating VA healthcare services beyond headache care.
Conclusion
Our engagement groups revealed varying important concerns and preferences for future headache services. Veteran patients identified numerous ideas and innovations to streamline provider communication, optimize appointment efficiency, address gender-specific challenges to receiving appropriate care, and improve headache management. Many participants highlighted the underlying need for a headache community to support and advocate for difficulties related to living with headache. Veterans also emphasized interest in holistic interventions beyond medications, corroborating results from previous research. Overall, participants desired high quality headache care which is coordinated across multiple disciplines, incorporates complementary and integrative health approaches and educational initiatives into headache care planning, and attends to gender-specific needs.
ACTIVE for Headache will continue to serve as a resource for clinicians, researchers, administrators, and policy makers as the VA continues improving headache care quality and delivery across the HCoEs and throughout the largest integrated healthcare system in the United States. We plan to disseminate our findings to these Veterans engagement groups and further plan for future engagement. ACTIvated Veterans Engagement groups are continuing to inform the HCoE's clinical and research initiatives as well as provide a safe space for gender-specific groups to share experiences, preferences and receive support.
Footnotes
Acknowledgements
The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States government . We would like to express our profound gratitude to our veteran group facilitators, Christine Calabrese and Sean A. Baird , who brought their lived experience into leading engagement group discussions.
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by OD, SB, HL, TD. The first draft of the manuscript was written by OD, and all authors commented on previous versions of the manuscript. All authors reviewed and approved the final manuscript.
Data Availability
The data used and analyzed must remain on the US Department of Veteran Affairs (VA) servers. A limited de-identified data set may be available upon request and fulfillment of the VA data use agreements.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Sico has received grant support from the Department of Veterans Affairs, the American Academy of Neurology, and the American Heart Association/American Stroke Association. Dr. Damush was supported by the VA Health Services Research & Development Research Career Scientist Award, RCS 19-002. All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Ethical Considerations
The VA Connecticut Healthcare System Institutional Review Board approved this research study, #JS0010.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was funded by
Veterans’ Health Administration Headache Centers of Excellence (Sico), and Dr. Damush was supported by the VA Health Services Research & Development Research Career Scientist Award, (grant number RCS 19-002).
Statement of Informed Consent
This study received a waiver of written informed consent and waiver of HIPAA authorization. Participants were informed that the purpose of the interview was to learn about their experience with headache and hear their input on what the VA's Headache Centers of Excellence (HCoEs) can do to treat headache and improve clinical and research initiatives and that the results of this project may be reported in medical journals or at meetings. Patients provided verbal consent to participate and for publication. Participants also verbally consented to have engagement groups audio recorded and transcribed.