
Abstract
Health care providers need to support families and provide resources when facing their child's death and potential organ donation. Aims of this retrospective chart review in a tertiary health care system were: (1) describe characteristics of pediatric organ donors compared to those who were not; (2) determine differences between services utilized by families who selected organ donation versus those who did not. From 2017 to 2023 of 288 pediatric deaths, 76 were organ donors and 212 did not donate. Organ donors’ mean age at admission was 6.3 ± 5.8 years. Thirty-four (44.7%) participated in Honor Walks. Significant differences existed between organ donors and non-organ donors in patients who were diagnosed with SIDS (3.9% vs 13.2%; P = .025). This study provides additional data to help further our understanding of bereavement support services for families making difficult decisions regarding organ donation.
Introduction
For families suffering with the impending loss of a loved one, death at the end of a long life is more easily understood than the death of a child. Grief after death is a normal and natural reaction to loss, however, it is especially devastating for parents.1,2 At a time when it may be difficult to comprehend what has happened, health care providers ask families to make complicated, difficult decisions including those about organ and tissue donation.3,4 Organ donation not only occurs after sudden death, but in some cases, after acute complications from chronic illness. As with adult donation, pediatric donation encompasses visceral organs, cornea, or skin. 5 During this time of overwhelming grief and suffering, parents have expressed the need for providers to give ample time to understand the end-of-life information. As the families process their grief, there may be reasons to consent to organ donation in order to attach meaning to the traumatic event. 6 Most important is the desire to make meaning of their child's death and give honor to the child's life.7,8 It has been well documented that those who receive psychological support from health care providers are better able to cope with the reality of their child's death and may be more likely to consent to organ donation.
Participation in organ donation to honor the deceased may play a significant role in the grief work of families and may offer benefits to ease the suffering experience. 9 Factors such as the family's support network or previous stress and grief experiences may also influence the bereavement process. In the critical care environment, a family may initially experience hope for recovery, but when that is not plausible, comfort is derived from the idea that something valuable will come out of the death.1,10 Discussions of organ donation, therefore, must be managed in a time-sensitive way and with extraordinary care.9,11,12
Feelings of abandonment, lack of support, and poor-to-little follow-up provide the empirical findings needed for health care providers to provide early and ongoing support to donor families.11,13 Given this, rituals at end-of-life, activities that are performed in a specific place and at a designated time, can provide structure and security during the immediate period of grief and loss. Rituals often consist of spiritual and religious practices such as sacraments, funerals, and memorial services. Additional end-of-life activities include honoring the deceased with a sacred pause by health care providers in the hospital room and words of honor spoken by the family over the child.14–16 In the pediatric setting, teams of allied health care professionals including social workers, chaplains, various therapists, counselors, and child life specialists may assist families with services designed to memorialize their child.16–18
An emerging ritual with organ donation is the institution of an “Honor Walk.” Occurring prior to donation, the critical care team and other health care professionals stand in silence in an area leading to the operating room to acknowledge and honor a family's decision to donate their loved one's organs. Raising an organ donation flag has also been mentioned in the literature as another way to honor organ donors. This often occurs prior to the Honor Walk and organ donation. The family, health care providers, and chaplains gather to raise an organ donation flag as another way to commemorate the gift of life the family is offering.19,20
Despite the importance of comprehensive bereavement care, there is limited evidence describing what is working, and what is most impactful for families who agree to pediatric donation. 21 Given this, the aims of this retrospective chart review were: (1) to describe the characteristics of cases of children who were pediatric organ donors compared to those children who were not. We anticipate differences in selection of organ donation by circumstances of the child's death; (2) to determine differences, if any, between the diagnosis of the child at death and services utilized for those families who selected organ donation versus those who did not. We propose that there is a relationship between type of services selected and diagnosis of the donor.
Methods
Setting and Sample
This was a retrospective cohort study at a tertiary-care, freestanding urban pediatric health care system with two pediatric intensive care units (PICU); one a Level 1 Trauma Unit and one a Level 2, with a combined average of over 6000 patients admitted annually to the PICUs. Of that number, 638 children have died while 288 patients, when meeting the criteria, were referred to the state's organ procurement organization (OPO) for organ donation consideration.
During this period of 2017-2022, 76 families made the decision to donate their child's organs. Inclusion criteria for this study: (1) all pediatric patients ages 0-21 years admitted to the PICUs from January 1, 2017, to March 31, 2022, who died in the PICU; (2) met organ donation eligibility criteria: (a) determination of brain death via protocol; (b) withdrawal of cardiorespiratory support being considered on the grounds of a poor prognosis; and (c) the OPO facilitating organ retrieval and the treating physicians considered the individual to be medically suitable for donation of visceral organs, or just corneas or tissues, preceding or at the time of their death5,18,22; (3) pediatric patients in the PICU identified by organ procurement criteria as potential donors, whose families were approached about organ donation were included in the retrospective review. This study included all clinical processes for donation of organs guided by the state and hospital clinical transplant protocols.18,22
Patient demographics extracted from the electronic medical record (EMR) included: age, race, sex/gender, language, insurance, and religious affiliation. Specific patient characteristics extracted from the EMR included admission diagnosis and circumstances, PICU length of stay, cardiac downtime, death circumstances, and organs donated. Also extracted from the EMR were additional variables of support services such as chaplaincy, social work, family experience liaisons, child life services, music therapy, outside supports, organ donation flag-raising ceremonies, and Honor Walks.
Data Analysis
Descriptive statistics were computed for demographic and clinical characteristics. Continuous variables were summarized as means and standard deviation. We calculated counts and percentages for categorical variables. Differences in continuous variables were tested using two sample t-test. Differences in categorical variables were calculated using Chi-square test and Fisher's exact test, respectively. All statistical analyses were conducted in SAS version 9.4 and statistical significance was evaluated at the 0.05 threshold. 23 All data was extracted from the EMR and saved in a password-protected file on a password-protected secure server. This study received the health care system's Institutional Review Board approval (Study #00000815).
Results
A total of 288 pediatric deaths between 2017 and 2022 met the inclusion criteria. The majority of the pediatric patients had public insurance, 69.5% (n = 198) and the mean age of 5.7 ± 6.0 years. From this group, 76 (26.4%) of the children were organ donors and 59% of the donors were male (n = 45). Those who became organ donors had a mean age at admission of 6.3 ± 5.8 years. Also from the total sample, 212 (73.6%) were not organ donors. Those who did not donate had a mean age of 5.5 ± 6.1 years (P = .345). Please see Table 1 for demographic and clinical characteristics of donor and non-donor; with comparison by organ donation.
Demographic and Clinical Characteristics of Donor and Non-Donor; with Comparison by Organ Donation.
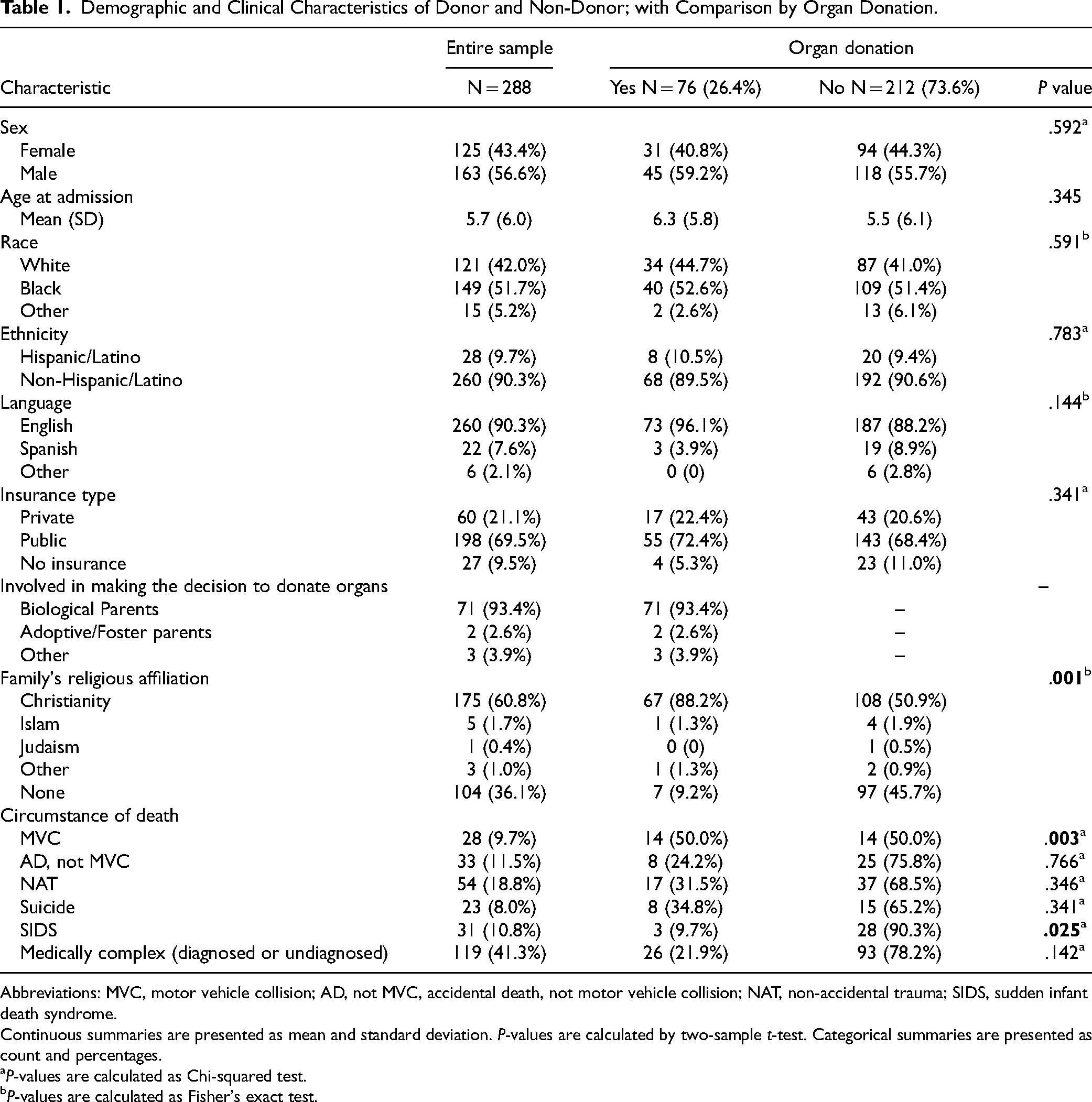
Abbreviations: MVC, motor vehicle collision; AD, not MVC, accidental death, not motor vehicle collision; NAT, non-accidental trauma; SIDS, sudden infant death syndrome.
Continuous summaries are presented as mean and standard deviation. P-values are calculated by two-sample t-test. Categorical summaries are presented as count and percentages.
aP-values are calculated as Chi-squared test.
bP-values are calculated as Fisher's exact test.
The majority of the patients in this sample died of a previously diagnosed or undiagnosed complex medical illness at the time of admission; of those 119 (41.2%) patients, 26 (21.9.2%) consented for donation; 93 (78.2%) did not (P = .142). Significant differences existed between pediatric patients diagnosed with sudden infant death syndrome (SIDS). Of the 31 with SIDS; 3 (9.7%) were donors versus 28 (90.3%) who did not (P = .025). Please see Table 2 for type of organ donated by organ donors.
Type of Organ Donated by Organ Donors (N = 76).

Multiple bereavement services were utilized by the majority of the families of the pediatric patients before death; 34 (44.7%) organ donors’ families participated in the Honor Walk and 26 (34.2%) participated in the organ donation flag-raising ceremony, while 18 (52.9%) participated in both events. Overall, of the total sample 288 (96.2%) families utilized chaplaincy services for support. Little differences in the use of chaplaincy between those families who agreed to donation versus those who did not; 100% (n = 76) versus 95.3% (n = 202), respectively (P = .068). Those who donated versus those who did not rely on family support for their grief; 96.1% (n = 73) versus 87.3% (n = 185), respectively (P = .031). See Table 3 for outline of bereavement services utilized.
Donor Family Selection of Bereavement Support Services.

aP-values are calculated as Chi-squared test.
bP-values are calculated as Fisher's exact test.
Discussion
With this study, we highlighted characteristics of not only those who consent to pediatric organ donation but also those who do not. We also sought to examine the relationship, if any, between characteristics of the child's death, selection of organ donation, and utilization of services for grief support in our health care system. This study provides additional information that may help to further understand the needs of families as they make the difficult decision for organ donation.
In our health care system, families who consented to donation of their child's organs had only a few significant differences from families who did not consent; namely donation of organs from a child who died as a result of injuries sustained in a motor vehicle accident (MVA) and those who died as a result of SIDS. For families experiencing grief and loss in both scenarios, organ donation may balance the pain and suffering with the associated loss. Kentish-Barnes et al reported families felt empowered and that they were active partners in an overwhelming situation, even if they chose to not donate. 24 Unfortunately, the vast majority of parents of a child who may be eligible for organ donation are rarely approached.24,25 It has been reported at one children's hospital, 23% of all withdrawal of therapy cases were not referred to an OPO while in 2017 alone, over 6500 people died while on a waiting list for an organ donation.19,26
Organ donation is not at the forefront of a parent's mind when the death of an infant is unexpected, as is the case with SIDS. 5 Our data supports the need for greater awareness of pediatric organ donations, as only 26.4% of those eligible donated their child's organs. 27 Almost 2000 children under 18 are waiting for organs; 25% are under five years of age. 27 There is a dearth of organs available to infants because of the limited availability of organs that fit their anatomic size. Typically, they must receive organs from other young children. 9
Of interest and in need of future study is organ donation in the case of a child's death due to non-accidental trauma (NAT). In a retrospective review of the Scientific Registry of Transplant recipients from 2008 to 2019, it appears the NAT group was less likely to be approached about organ donation, but these families were more likely to consent. 28 In fact, seventeen of the fifty-four families who experienced the death of a child from NAT in our health care system agreed to donate. Thus, organ donation can be one way for families and medical professionals to make some sense out of a senseless event. Although when a child has died potentially at the hand of a parent or caregiver, the situation presents unique ethical concerns. These can include the protection of evidence in the surgical and autopsy findings. Early discussions surrounding organ donation in fatal child abuse cases are imperative and bringing the health care team, investigators, forensic team, and the OPO together could prevent further trauma to the health care providers and families involved. 5
Similar to national findings, more families in our study declined donation than accepted.27,29 Prior exposure to organ donation information, personal beliefs, and behaviors regarding organ donation, who first mentions the possibility of organ donation, interactions with the health care and OPO team, along with family disagreement about donation all influence the decision to donate.24,25 The health care team, in concert with the OPO, can support the families through commitment to building a trusting relationship and tailoring communication to match spiritual or cultural expectations. 9 Parents of pediatric donor candidates need to feel supported by the critical care team and OPO coordinator regardless of their decision, and to have enough time to discuss donation with family members involved. 25 Several studies reported if parents perceived any health care providers or OPO professionals appeared insensitive, this was a key factor in not consenting to donation among the 50% of parents who were initially undecided.26,30 Families who reported higher satisfaction with their health care providers also tailored communication to match spiritual or cultural expectations.24,25 Additionally, important to families is the need to explain in simple, less frightening language they can understand and process to make their final decision. 24
Finally, organ donations have been reported to drop precipitously during the Covid-19 pandemic. 28 Our data potentially reflects this decrease as well, given 2 years of data was collected from 2020 to 2022. Renewed greater public organ donation educational efforts need to continue to highlight the importance of organ donation to impact organ donation attitudes and beliefs more favorably. 29 Understanding the perspective of the families of dying children may provide valuable insight for an interdisciplinary approach to end-of-life care.
Only five organ donations occurred after circulatory death in our health care system while the majority occurred following brain death and this is demonstrated in the scientific literature. Donor management is distinctly different with brain death and donation after circulatory death. Donation after circulatory death remains an ethical challenge as death must occur quickly after removal of life-sustaining equipment and parents may feel the death is rushed or less than peaceful.31–34
Regarding the selection of support services utilized, chaplaincy and social work were involved in all organ donation cases as these are standard practices. It appears religious support is important for donor families as this can be an avenue that provides comfort. In addition, Child Life and Music Therapy participated in legacy-making opportunities with the majority of organ donation families. These activities included the making of handprints and footprints, securing a lock of hair and heartbeat recordings that were placed inside of a stuffed animal. In our health care system, families are clearly utilizing the current services regardless of donation decision.
Bereavement literature suggests that the formation of connections with others and building community after a child's death is an essential part of the healing process. A majority of organ donor families utilized outside support from their extended families and community networks. In particular, the OPO has been cited as an ongoing source of family support with bereavement groups and celebration of life activities.5,27 Additionally, connections with the PICU health care providers is reported as an effective bereavement tool for parents in the weeks following their child's death. 2 Along those same lines, the child's primary care provider has a vital role in supporting the family after the death, especially if the relationship has been longstanding. Meeting with the parents face to face, and listening may allow providers to recommend further bereavement support and mental health services.6,34–36,37,38
For families choosing organ donation in our health care system, an organ donation flag-raising ceremony is available for donor families. Additionally, an Honor Walk was introduced in 2019 as another support tool to honor the donation of the child and the family.
Implications for Bereavement Services
Scientific evidence suggests families that receive multiple avenues of support may experience less symptoms of complicated grief during bereavement.3,6 Caring for each family's grief throughout the trajectory of their child's illness or injury and death may promote healthy coping and resilience for the future. Bereavement services may be a meaningful and lasting component of care that cannot be overlooked. 6 However, future research is needed to fully understand which services institutions provide the most assistance to parents in their grief work. There is still a need to understand how participation in specific services such as these may help grieving families begin processing their loss.
Limitations
Our study had several limitations. The retrospective nature of the study does not lend itself to generalizability to other pediatric health care systems. In addition, the study did not demonstrate a relationship between characteristic of the child's death and choice of organ donation and support services utilized. Families were utilizing the support services offered regardless of donation. Lastly, future research is warranted on participation in organ donation flag raising ceremonies and Honor Walks as the newer support services being offered.
Conclusion
When caring for the family and the child who will be an organ donor, health care providers and support services can impact the decisions parents make regarding organ donations.36,39 By recognizing for families that “grief is not a problem to be solved, but a process to live through,” 40 health care providers can leverage both internal hospital resources and community networks to support and surround families as they journey through a difficult time. Developing opportunities to partner with the OPO outside the PICU deserves consideration as it could be beneficial for donor families as the OPO offers a wide array of bereavement supports. 22 In addition, partnering with faith-based organizations and other support groups could facilitate further continuation of care within the community. A future qualitative study is planned to examine lived experiences of families participating in organ donation and support activities for its impact on their bereavement process. Connecting with grieving families after the first year will contribute new information on the emerging trend of Honor Walks, organ donation flag-raising ceremonies and the efficacy of other support activities thus adding to the body of literature about these practices.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.