
Abstract
We conducted a prospective observational study on 100 consecutive patients admitted to intensive care units at Leeds General Infirmary following out-of-hospital cardiac arrest. In the non-survivors, we reviewed their potential for organ donation via donation after circulatory death. Out of the 100 patients, 53 did not survive to hospital discharge. Out of these non-survivors, 13 died very suddenly within the intensive care unit and 3 other patients subsequently died in a general ward following discharge from the intensive care unit. One patient became brainstem dead, with out-of-hospital cardiac arrest secondary to a subarachnoid haemorrhage, rather than a primary cardiac cause. This patient went on to donate via the brain death mode. The remaining 36 patients had treatment withdrawn in the intensive care unit. Of these, 29 were referred to the transplant team for potential donation after circulatory death, and 14 were deemed to be medically suitable for organ donation. However, the families of only seven agreed to proceed with the donation process. Of these seven, only one went on to donate, primarily because the majority did not die within the 3-h window for acceptable warm ischaemia. In this series, the potential for donation after circulatory death following out-of-hospital cardiac arrest was limited. We would suggest an open dialogue between intensive care unit staff and transplant teams about the realistic potential for organ donation in each case. When clinicians believe it is unlikely that donation after circulatory death will proceed due to a failure to die within the pre-requisite time, then not starting with the donation after circulatory death process should be seriously considered.
Keywords
Introduction
Organ transplantation has the potential to transform the lives of many patients. In the UK and other developed countries, there are significant numbers on waiting lists for solid organ transplants, and every year this number rises as more patients are recognised as potentially suitable for a transplant. 1 Whilst the number of organ donors is increasing, there remains a significant gap between the numbers of patients requiring organs and the number becoming donors. In 2008, the Report from the Organ Donation Taskforce 2 aimed to address the barriers to organ donation, to increase the number of deceased donors and therefore to reduce the gap between the number of donors and the number of potential recipients. As a result of the Report, there was an introduction of a UK-wide Organ Donation Service, a re-arrangement of donor co-ordination and a restructuring of organ retrieval arrangements. Despite this, there continues to be a significant gap between the number of patients awaiting a transplant and the number of organ donors.
When transplantation first began, the main source of donors came from patients donating via the donation after circulatory death (DCD) route. However, with the recognition of brainstem death in 1968, donation after brain death (DBD) became a possibility and was thought to be superior to DCD due to the reduction in warm ischaemic times. However, as the prevention and care of trauma and neurosurgical patients has improved, the number of patients who become brainstem dead has fallen, together with a reduction in donors from this source. This has led to a search for other sources of potential donors and a resurgence of interest in donation after circulatory death.
One group of patients who have potential for DCD are those with severe and life-limiting neurological impairment after resuscitation following out-of-hospital cardiac arrest (OOHCA). In the UK, we are encouraged to routinely consider all deaths, including these patients, for organ donation. However, there is experience and a belief amongst some intensive care unit (ICU) clinicians that this patient group represents a limited potential for organ donation, due to the fact that generally they do not die within the requisite short time period of warm ischaemia (around 3 h) following withdrawal of life-sustaining treatment. These patients often have poor neurological recovery but in the clinical context of good cardiovascular recovery. They are generally not brainstem dead to allow for DBD nor do they have sufficient cardiovascular or respiratory instability to die quickly and allow DCD.
A previous study performed in Leeds (2007) suggested the above to be the case. 3 This retrospective study reviewed the data on 100 consecutive patients admitted to two centres following OOHCA. Eighty-six patients died in the ICU of which 57 had withdrawal of active management within the ICU. Of these, only four patients fulfilled the criteria to be considered for organ donation. The authors concluded that ‘only a small increase in donor organs could be potentially achieved from this population’.
However since this study, much has changed in relation to the care of these patients. First, organised resuscitation services outside the hospital are generally more widespread and advanced. Second, the provision of routine acute Primary Percutaneous Coronary Intervention (PCI) after ST elevation MI (STEMI) has become standard. Third, a focus on temperature management following return of spontaneous circulation (ROSC) has become widely accepted as routine care for patients who are post-OOHCA. These changes may have altered the clinical course of this patient group and may influence their feasibility to become organ donors.
We therefore conducted a prospective observational study of all the OOHCA patients admitted to the ICU in a large university teaching referral hospital (Leeds General Infirmary) with regional PCI facilities over an approximate one-year period. Our aim was to determine whether the organ donor potential had improved since the original study in 2007.
Method
One hundred consecutive patients admitted to the ICU following OOHCA were followed throughout their stay by the primary investigator. The anonymised data collection form is shown in online Appendix 1. The study was considered to be a service improvement audit rather than clinical research by the local research ethics committee and therefore did not require consent procedures.
All patients had been resuscitated and spontaneous circulation restored either in the community or in the Emergency Department (ED). All were assessed as soon as possible after ROSC by cardiology specialists for suitability for PCI. Patients were referred for critical care support and admission when they failed to awaken adequately following ROSC, or remained unstable requiring cardiovascular and/or respiratory support.
Following ROSC, all patients were stabilised in the ED and standard supportive care commenced. This included tracheal intubation and assisted ventilation, invasive monitoring with central and arterial lines, inotrope or vasopressor support as indicated, and sedation with infusions of propofol and subsequently alfentanil. All patients had urinary catheterisation and hourly urine output monitored. Once stabilised, the patients were transferred to an ICU, either directly from the ED or via the cardiology catheter labs.
Following admission to ICU, therapeutic hypothermia was commenced as standard care. The target temperature was 33℃ (as per two landmark papers from 20024,5) and interventions to achieve this included cold intravenous fluids, ice packs and surface cooling via the ‘cair cooler’ device. Our ability to cool patients to target temperature was variable and some patients failed to reach target temperature at all despite the above measures. Approximately nine months into the study, the TTM trial was published 6 which disputed the value of cooling to 33℃ and therefore during the subsequent three months, temperature management was less consistent, with some patients being targeted at 33℃ and others at 36.5℃.
Following the period of temperature management (typically 24 h), during which time patients were sedated and paralysed, they were re-warmed and subsequently sedation was discontinued. A period of monitoring of brain function then commenced. For the patients who regained reasonable brain function relatively rapidly, extubation and discharge from the ICU followed. For the remaining patients, a period of observation then began.
Like many ICUs, we have no precise protocol for the timing of neurological assessment for prognosis or for the use of investigations to aid in prognostication (this may change in light of the recent ERC/ESICM guidelines 7 ). Most patients were therefore observed, usually for a period of several days, and many who failed to awaken subsequently underwent EEG and CT brain scans. The decision to withdraw treatment was then made by using a combination of clinical findings, CT and EEG results, along with discussions with family members as to their perceived views of what course of action the patient would have been likely to wish. The exact timing of these investigations and discussions were dictated by the ICU consultant in charge and therefore the timeframe from admission to ICU to treatment withdrawal were variable amongst this patient group. As yet, we do not have access to somatosensory evoked potentials to aid in prognostication.
Organ donation data.
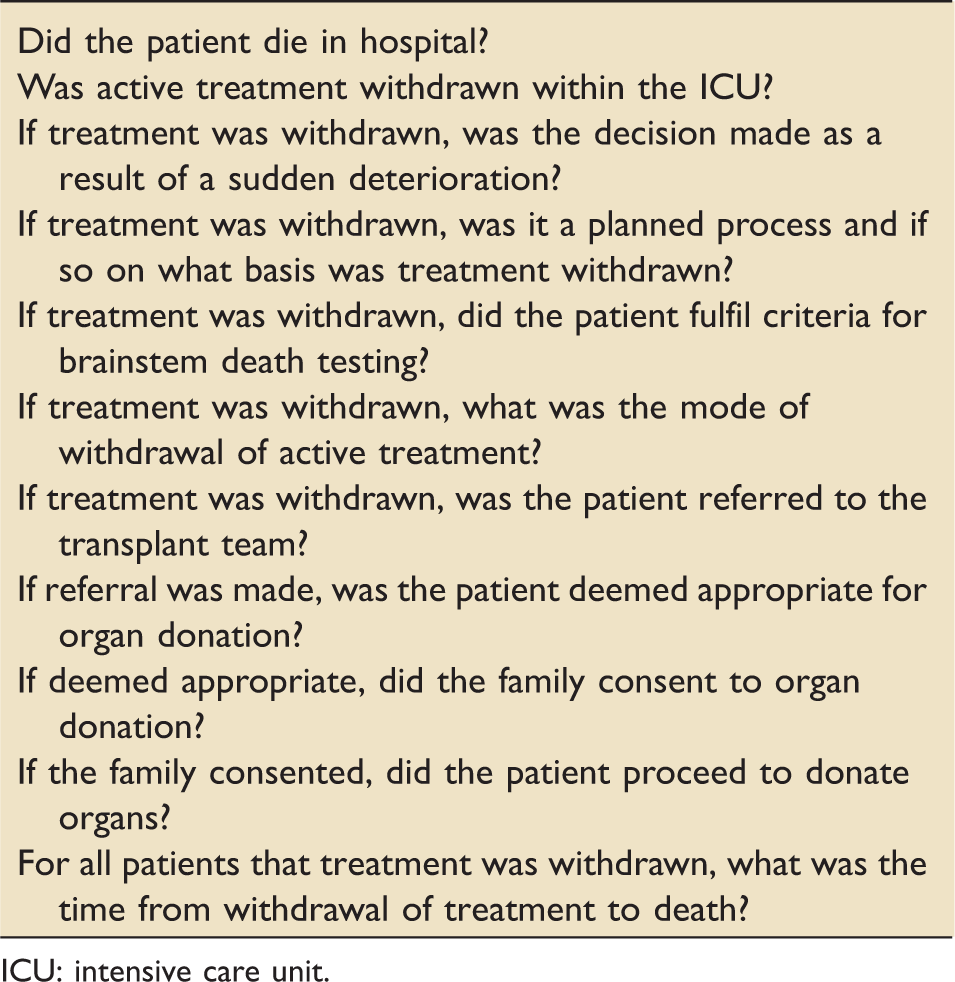
ICU: intensive care unit.
Results
Baseline data.
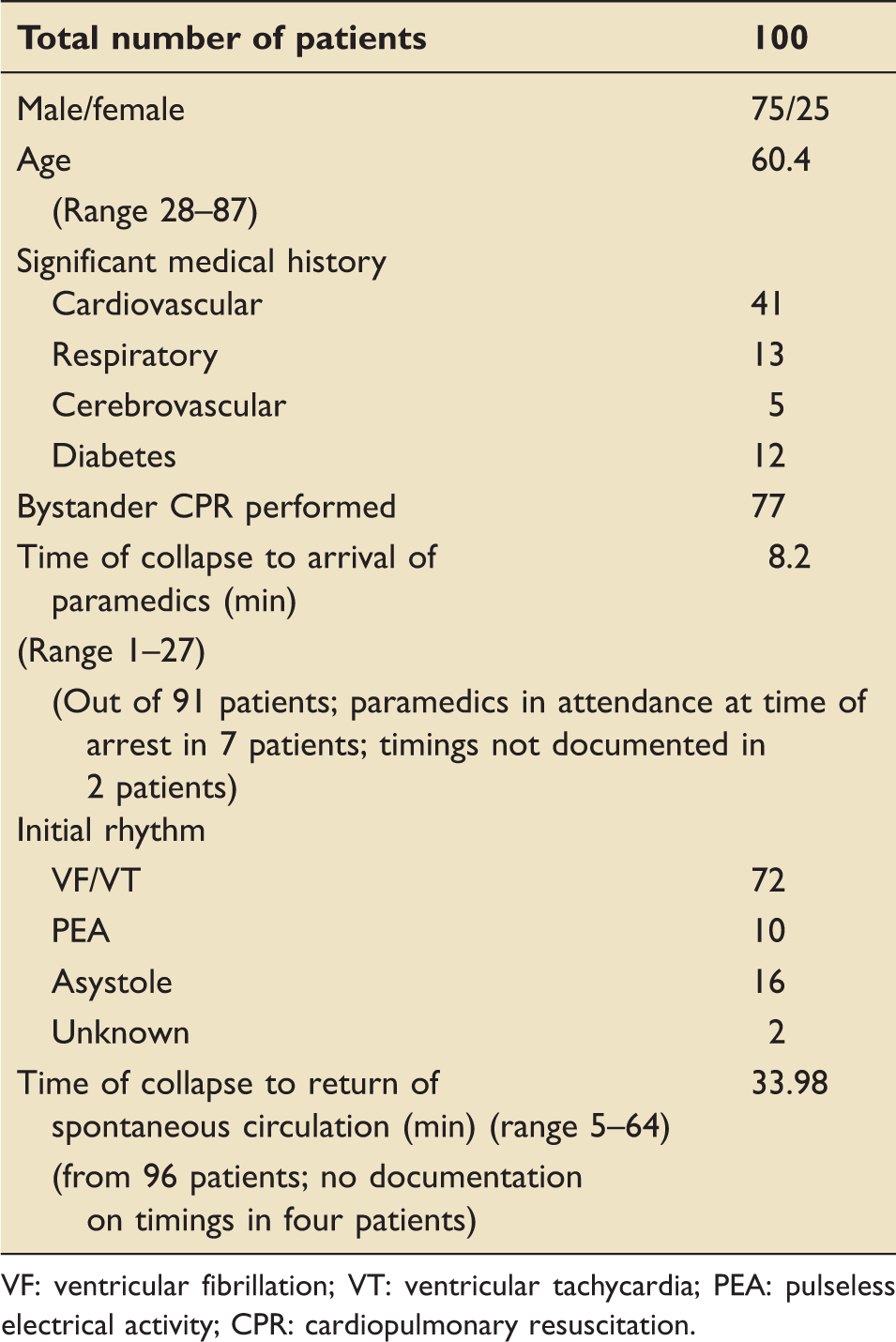
VF: ventricular fibrillation; VT: ventricular tachycardia; PEA: pulseless electrical activity; CPR: cardiopulmonary resuscitation.
Of the 100 patients, one patient had two episodes of OOHCA and was therefore admitted and documented twice and survived both episodes. Fifty-three patients died within the hospital setting, either in the ICU or in the ward. Forty-six survived and were discharged from the unit (taking into account that one patient represented two patient episodes).
Of the 53 patients who died, 13 died very suddenly in the ICU (further cardiac arrest/death on maximal support or sudden deterioration precipitating rapid withdrawal of organ support). For these 13 patients, the potential for ‘uncontrolled’ organ donation was not possible, because as yet we do not have the structure and support mechanisms in place to allow ‘uncontrolled’ DCD to take place. Three of the patients who died did so subsequently on a general ward following discharge from ICU without full withdrawal of active treatment within the ICU setting.
Mode of active treatment withdrawal.
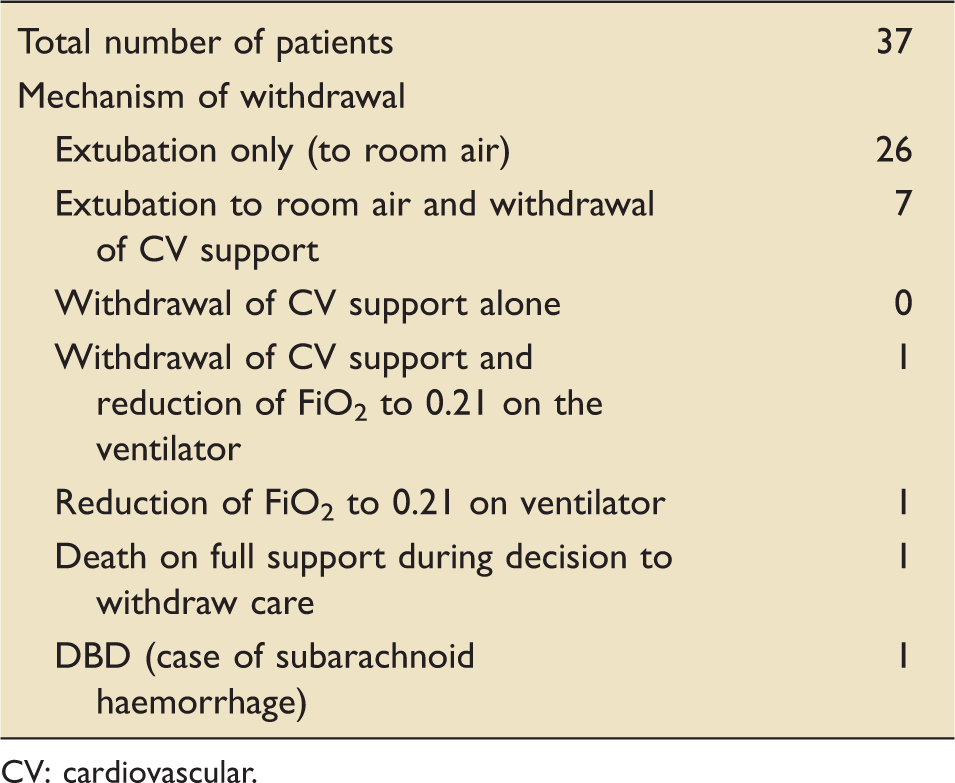
CV: cardiovascular.
Organ donation data.
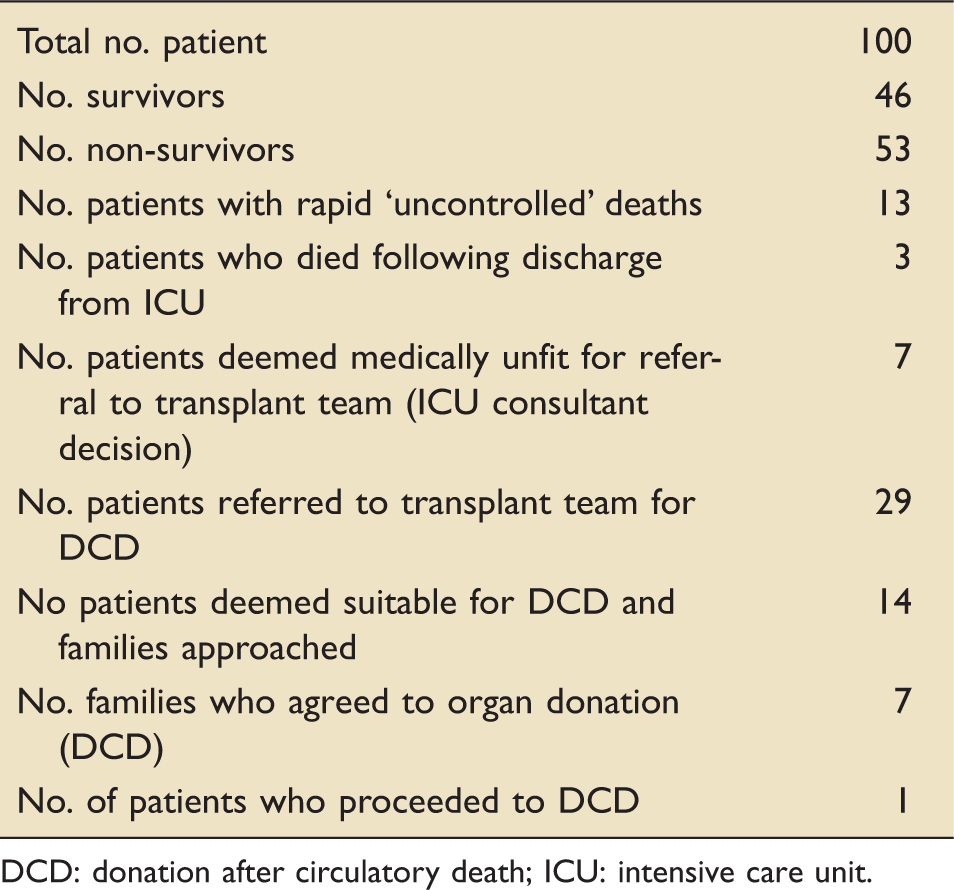
DCD: donation after circulatory death; ICU: intensive care unit.
Of the seven patients who would have theoretically been appropriate for DCD but whose families refused consent, 5 of these actually died within the 3-h ‘window period’ (5 min; 20 min; 22 min; 1 h 20 min; 2 h 35 min; 6 h 46 min; 20 h). However, as close monitoring was not maintained because the DCD process was not in place, and the transplant team were not resident during this time frame, we do not know whether they would have remained suitable for donation, or if a period of hypoxia or hypotension may have precluded donation. Unfortunately, this degree of data collection does not occur in patients in whom treatment withdrawal has occurred and therefore it is unclear as to whether any of these patients would have gone on to donate had the families agreed to DCD.
Discussion
There is an ongoing shortfall between the number of patients awaiting transplantation and the number of patients becoming donors. As a result, DCD donation has become a focus for potential deceased organ donors, with the demonstration that many organs tolerate warm ischaemic times and are suitable for transplantation after DCD. 9 Patients who are having treatment withdrawn following OOHCA have been identified as potential DCD donors. There is a policy of ‘referring all’ patients considered suitable for DCD donation in an attempt to ensure no potential donors are missed and organ donation maximised. Frequently, this results in progressing with the DCD process in all patients assessed as being potentially suitable for DCD regardless of consideration of the likelihood of organ donation actually occurring. This can result in many DCD’s being ‘stood down’ and the transplant team disbanded when the patient fails to die within the requisite time frame.
The previous retrospective study published in 2007 3 reported that of 100 patients, only four would have been appropriate for consideration of DCD. In our prospective study, this figure has increased significantly, with 15 patients being deemed appropriate for organ donation by the transplant team. However, despite this, only one patient actually went on to donate via the DCD pathway (and one via DBD who had sustained a SAH).
Like the 2007 paper,
3
this series also suggests that patients who die following OOHCA represent a limited source for potential solid organ donation. It seems that these patients tend to fall into one of two categories
They are either too unstable or on too much organ support to be considered potential donors because the timeframe for setting up the process is too long in the setting of gross cardiorespiratory instability (and we do not yet have the ability to facilitate ‘uncontrolled’ DCD). They are on minimal cardiovascular and/or respiratory support and progress through the potential organ donation process but fail to die within the requisite timeframe.
It appears that in order to progress through the process, AND die in an appropriate timeframe, patients need to be receiving a significant degree of cardiovascular and/or respiratory organ support, such that rapid death will occur on its removal, but not so much support that it precludes the option of organ donation. Unfortunately in this study population, few patients fitted into this category.
Paradoxically it is possible that more effective resuscitation, PCI, temperature management and other supportive care may have had an impact on this pool of potential donors by:
Improving patient survival in the short and long term Preserving myocardial, lung and brain function such that the patient survives in the short term but does not make a good functional neurological recovery. Then when treatment is withdrawn the patient takes a long time to die due to partially preserved vital organ function.
Whilst we agree that all potential patients should be referred, we would argue that an open discussion should take place between the ICU clinician and the transplant team, about the realistic potential of achieving donation. In patients that are felt unlikely to die within the requisite time frame, we would suggest that not progressing with the donation process should be considered a potential option. We would advocate a ‘patient by patient’ approach to DCD, with consideration of the likelihood of donation actually occurring being an active part of the discussion.
The DCD process is a lengthy and costly process. The patient continues to occupy an ICU bed and the entire transplant team needs to be in situ in the hospital for the withdrawal process to occur and a staffed theatre needs to be kept vacant. In patients for whom we believe there is minimal chance of donation actually occurring, our more considered approach would lead to more appropriate (and cost saving) use of the transplant services.
Following this study our local transplant team have adopted a more pragmatic approach in trying to assess whether such potential donors are likely to die within the requisite time frame, and decisions have been made not to proceed with potential DCD due to the perceived unlikely possibility of DCD occurring. To date, we are unaware of any potential donors being ‘missed’ as a result of this approach.
Currently, we are unaware of methods for predicting which patients are likely to die within the requisite 3 h once active treatment is withdrawn. There is usually a clinical opinion as to whether the patient is likely to die based primarily on the level of cardiorespiratory support, but there is no validated tool to assist in our prediction. Several authors have looked at using parameters such as levels of cardiorespiratory support as well as clinician opinion to predict time to death from withdrawal of treatment10–12 but as yet there is no validated tool in common use. It may be that in the future a tool can be constructed, based on parameters such as A-a O2 gradients, respiratory effort, gag reflexes, inotropic/vasopressor support, use of intra-aortic balloon pump, to aid in our identification of patients who have a realistic likelihood of proceeding to organ donation following treatment withdrawal.
We would be interested to know whether our experience in this group of patients is mirrored in other national and international centres.
Conclusion
We question whether it is reasonable to routinely put a large number of patients, who are dying after OOHCA, through the potential donation process when the chances of donation are low. We advocate a move towards a more considered approach that balances the risks and benefits for every patient and family, based on careful medical assessment and frank discussions with the transplant teams. Validated tools for predicting accurate prognosis for withdrawal of treatment, and the predicted speed of death after treatment withdrawal are required.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Andrew Bodenham is an editor for JICS.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.