
Abstract
Introduction
Organ donation and transplantation can be lifesaving. Many donors are older adults. National Donor Registries can promote adherence to patients’ rights and safeguard patient integrity if the question about organ donation arises. However, a majority have not entered the National Donor Registry in Sweden.
Objective
Investigate how sociodemographic factors, health-related factors, and attitudes toward organ donation are associated with whether or not older adults in Sweden are registered in the National Donor Registry.
Methods
A cross-sectional survey design was chosen to explore associations between individual characteristics and registration behavior among older adults. Data was collected through the Swedish National Study on Ageing and Care (SNAC)-IT survey in 2023, a sub-study to the SNAC. 436 participants 60 years old or older answered the survey. The survey included questions on sociodemographic and health-related factors and attitudes toward organ donation. Data was analyzed using descriptive statistics, Spearman's rank correlation, and the Chi-square test.
Results
Registration in the Swedish National Donor Registry was low among older adults, with only 25.5% of participants listed despite 70.4% expressing a positive attitude toward organ donation. Among those who oppose organ donation only 6.9% were in the registry. Younger age, higher self-rated health, better health-related quality of life (EQ-5D VAS), being unmarried, being a previous smoker, and having a positive attitude toward donation were all significantly associated with being registered (p < 0.05). These findings demonstrate a gap between supportive beliefs and registration behavior among older adults.
Conclusion
There is a gap between beliefs and actions regarding organ donation among older adults. While most have a positive attitude toward organ donation, they are not registered in the National Donor Registry. Additionally, the vast majority who oppose organ donation after death are not registered, raising the risk that their actual wishes may be disregarded due to presumed consent.
Keywords
Introduction
Transplantation of organs and tissues can be a lifesaving treatment for someone with end-stage organ failure. It can also improve quality of life and increase health (Morton & Fontaine, 2018). The process of organ transplantation is complex, and finding a match is not easy (Morton & Fontaine, 2018). Identifying all potential donors is pivotal for decreasing the imbalance between organs needed and organs available (Cuende et al., 2007; Lewis et al., 2021; Pérez-Sáez et al., 2017), and donor registries are often used as an aid.
Review of Literature
In Sweden, as in many other countries, there is a National Donor Registry. In the Swedish National Donor Registry, it is possible to register preferences for donating organs and/or tissues upon death. It is possible to register both “yes” and “no” to donation (Nationellt Donationscentrum [Swedish National Donation Centre], n.d.). In May 2025, nearly 1.9 million of the Swedish population (about 18%) had chosen to register their preferences. 80% of them were positive towards donating their organs upon death (Socialstyrelsen [National Board of Helath and Welfare], n.d.). Hence, the Swedish population is more positive towards organ donation than has been shown in other countries (Febrero et al., 2022). It is well established that a documented statement of an individual's organ donation preferences can help facilitate decision-making if the question arises (Siminoff & Lawrence, 2002).
In 2023, a total of 258 persons donated their organs after death in Sweden (Scanditransplant, 2024), the highest number recorded to date. Nevertheless, as of January 2025, approximately 700 people remain on the national waiting list for a life-saving organ transplant (Socialstyrelsen [National Board of Helath and Welfare], n.d.). Looking at a European context, 3–4% of those on the waiting lists in the EU die every year (Vanholder et al., 2021).
An important component to address regarding organ donation is that global demographics are changing with an increasing aging population (Roser, n.d.). In 2024, about 27% of the Swedish population was aged 60 years or older (Statistikmyndigheten, SCB [Statistics Sweden], n.d.). This is also reflected when looking at statistics regarding organ donation and transplantation. Scanditransplant reports that the median age for donors was around 60 years (depending on cause of death) (Scanditransplant, n.d.). In 2024, organ donors in Sweden were 5–88 years old (Nationellt Donationscentrum [Swedish National Donation Centre], n.d.). Looking at the Swedish waiting list, about 30% are aged 60 years or older, and 298 persons aged 60 years or older were transplanted in Sweden during 2023 [personal communication, The National Donation Center, 2024].
When taking a closer look at the Swedish National Donor Registry, 37% of the registered persons were aged 60 years or older in June 2024 [personal communication with National Donor Registry, 2024]. As shown above, both organ donors and organ recipients can be older adults. The high proportion of older adults in the Swedish National Donor Registry is noteworthy since previous studies have shown that many older adults think that they might be too old or too sick to be a donor, hence opting out to register (Downing & Jones, 2008; Febrero et al., 2022). Further, there are several other factors that might influence the choice to enter the registry. While most previous studies have explored attitudes toward organ donation within the general population, there remains a notable gap in research specifically addressing older adults.
Therefore, the aim of this study was to investigate how sociodemographic factors, health-related factors, and attitudes toward organ donation are associated with whether or not older adults in Sweden are registered in the National Donor Registry.
Methods
Design
This cross-sectional study used data from the Swedish National Study on Ageing and Care (SNAC) (Lagergren et al., 2004), specifically drawing from the 2023 survey conducted within the SNAC-IT sub-study (Anderberg, 2020). This study adhered to the STROBE (Strengthening the Reporting of Observational studies in Epidemiology) guideline for cross-sectional studies (Appendix 1).
Research Question
This exploratory study was guided by the following research question: “What are the registration patterns toward organ donation among older adults in Sweden, and which sociodemographic, health-related, and attitudinal factors are associated with registration in the National Donor Registry?”. This question captures both the descriptive and analytical aim of the study and aligns with the exploratory design.
Sample
Data collection was conducted as part of the established national study SNAC, which is based on a randomly selected cohort of older adults in Sweden. This sampling method helps reduce selection bias and enhances the generalizability of the findings to the broader Swedish older adult population.
The SNAC project was established as a comprehensive initiative aimed at studying the health and social care needs of Sweden's aging population. The SNAC cohort comprises a randomized sample of the older population in Sweden with individuals aged 60 and older, gathering extensive data to support aging research. The SNAC-IT consists of a subset of the Blekinge cohort of the SNAC (midsized cities with rural areas) and focuses on data from technological, sociological, and health science perspectives on the aging population in Sweden.
Inclusion and Exclusion Criteria
The participants received the SNAC-IT survey via mail or email (N = 587), according to their preferences. All participants who completed the survey were eligible for inclusion. Participants were excluded from this study if they either responded “I do not want to disclose” or did not provide a response to the question about being registered in the Swedish National Donor Registry, the interest variable.
Compliance with Ethical Standards
This study was conducted in compliance with the Declaration of Helsinki and received approval from the Research Ethics Committee at Lund University (LU 604–00, LU 744-00). Written informed consent was obtained from all SNAC participants. All data in this study were anonymized.
Variables
Interest Variable
The interest variable of this study relates to the question: “Have you signed up for the National Donor Registry (where you decide whether you want to donate organs or tissues after death)?” from the 2023 SNAC-IT survey, which yields a yes or no response (those who answered “I do not want to disclose” were excluded from this study).
Predictor Variables
Sociodemographic Data
The collected sociodemographic data included information on age, gender (male, female), education level (primary school, high school, university or higher), marital status (married, widowed, unmarried, divorced), living situation (living alone, living with spouse or partner, other), occupation (currently working, retired, early retiree), and religious affiliation (religious, non-religious).
Health-Related Data
Health-related data were collected for the study, including body mass index (BMI; kg/m2), defined according to World Health Organization guidelines (WHO, n.d.). Smoking habits were categorized as “Never smoked,” “No, have stopped smoking,” or “Yes.” Alcohol consumption was recorded in the following categories: “Never,” “Once a month or less,” “2–4 times a month,” “2–3 times a week,” and “4 times a week or more.” General health data was assessed using two variables: self-assessed health categorized as “bad,” “fair,” “good,” “very good,” and “excellent” and the visual analog scale of the EuroQol 5 Dimensions instrument (EQ-5D VAS), which is a vertical scale from 0 (worst imaginable health state) to 100 (best imaginable health state) (EuroQol Group, 2024).
Attitudes About Organ Donation
The attitudes of the participants towards organ donation were gathered through a survey question: “Are you in favor of donating organs or tissues after death?” The possible responses to this question were “Yes,” “No,” and “Don't know.”
Statistical Analysis
All analyses were performed using R (version 1.4.1717; RStudio). Descriptive statistics were used to summarize the characteristics of the participants for all predictor variables and the variable of interest (In the registry). To examine associations between variables, statistical tests were chosen based on the scale of measurement. For continuous variables (age, BMI, and EQ-5D VAS), Spearman's rank correlation coefficient was applied because it does not require the assumption of normally distributed data and is less sensitive to outliers than Pearson's correlation. For categorical variables, Chi-square tests of independence were used because they are appropriate for assessing whether the distribution of responses in one categorical variable differs significantly across the categories of another. In addition, standardized residuals were examined to determine which categories contributed most to significant results, with residuals greater than 2 or less than −2 interpreted as statistically meaningful deviations from expected frequencies.
A significance level of 0.05 was adopted for all tests. Analyses were conducted using complete case analysis, with participants with missing data excluded from the analyses. This decision was made to preserve internal consistency and avoid the introduction of bias associated with imputation in an exploratory context. The extent of missingness is reported for each variable. The exclusion of incomplete responses and the use of standardized instruments aimed to reduce potential biases in interpretation. No subgroup or interaction analyses were conducted, as the primary aim was to explore associations across the full sample rather than to test predefined effect modifications. However, to strengthen confidence in the findings, sensitivity analyses were also performed. A logistic regression model was fitted to examine whether non-response on the outcome variable (In the registry) was systematically associated with sociodemographic or health-related predictors. In addition, missing values were imputed (mean for continuous variables and mode for categorical variables, e.g., BMI, EQ-5D VAS, alcohol), and the correlation (Spearman) and Chi-square tests were repeated.
Results
Sample Characteristics
In total, 436 participants answered the SNAC-IT survey (74.2% response rate). 21 participants were excluded from this study, 14 because they responded “I do not want to disclose” to the question about being registered in the National Donor Registry, and 7 did not provide any response to this question. The final analysis was conducted on the responses from 415 participants.
Descriptive information about the participants is presented in Table 1. The average age of the participants was 77.9 years (SD: 7.7), with a gender distribution of 53.5% male and 46.5% female participants. Regarding the attitudes of older adults on organ donation, 70.4% of the participants were positive, 11.8% were uncertain, and 17% were opposed. Although the majority of participants expressed positive views on organ donation, only 25.5% were registered in the Swedish National Donor Registry.
Descriptive Information About the Characteristics of the Participants of the Study.

BMI- body mass index.
Research Question Results
The Spearman's rank correlation coefficient was applied to examine the associations between the variable “In the registry” and the continuous predictors: age, BMI, and the EQ-5D VAS score. The Chi-square test was used to analyze the associations between “In the registry” and the remaining categorical variables. The results of these analyses are shown in Table 2.
Results for the Spearman Rank Correlation Coefficient and the Chi-Square Test for the Participants.

A significance level of 0.05 was adopted for all tests (in bold).
BMI - body mass index.
Several variables were significantly associated with registration in the Swedish National Donor Registry, including age, EQ-5D VAS score, marital status, self-assessed health, smoking history, and attitude toward organ donation. For the numeric predictors, a weak but significant negative correlation was found between age and registry inclusion (p = 0.004, rho = −0.14), indicating that younger individuals were more likely to be in the registry. Similarly, a significant positive correlation was observed between EQ-5D VAS scores and registry inclusion (p = 0.02, rho = 0.13), indicating that individuals who reported better perceived health status were slightly more likely to be included in the registry.
Among the categorical variables, marital status was significantly associated with registry inclusion (p = 0081, X2 = 11.80). The analysis of the residuals revealed a significant excess of unmarried individuals in the registry, while widowed individuals were significantly less likely to be registered.
The Self-assessed health variable also showed a significant association with the “In the registry” variable (p = 0.01, X2 = 13.10). Individuals reporting “Very Good” health had an excess of observations in the registry, whereas those reporting “Fair” health had a significant deficit. It is important to highlight that the extreme ends of the health scale (“Bad” and “Excellent”) had very low observation counts, with only 15 and 14 individuals, respectively, which may limit the interpretability of findings for these categories.
Smoking status was another significant factor (p = 0.014, X2 = 8.61). Individuals who had never smoked showed a deficit of observations in the registry, while those who had stopped smoking had a significant excess.
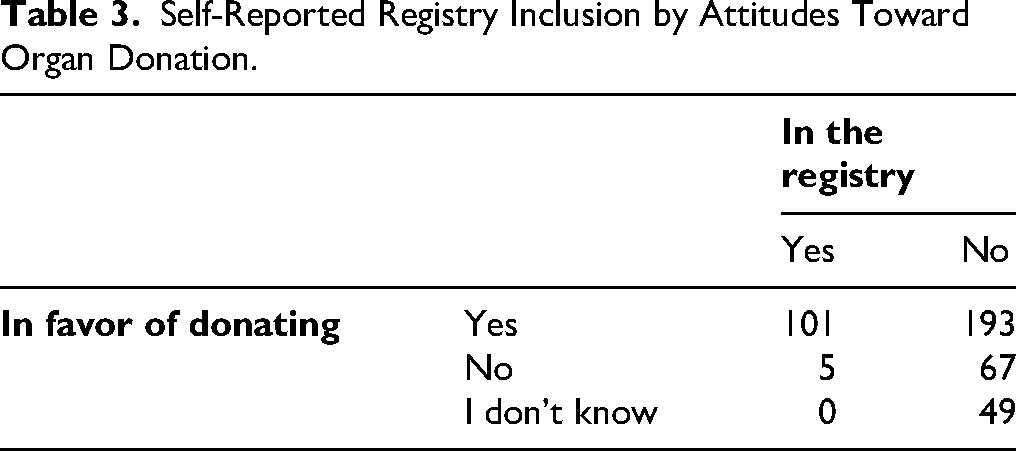
Attitudes toward donation were significantly associated with self-reported registry inclusion (p < 0.001, X2 = 41.90). Individuals who expressed to be in favor of donation were much more likely to indicate willingness to be in the registry, whereas those who were not in favor or uncertain were underrepresented. This is a noteworthy finding; however, the majority of older adults, regardless of whether they are in favor of or oppose organ donation, are not in the national registry (see Table 3).
Self-Reported Registry Inclusion by Attitudes Toward Organ Donation.
In contrast, no significant associations were identified between registry inclusion and religion, education level, occupation, alcohol consumption, or living situation.
Sensitivity Analysis
To strengthen confidence in the findings, two additional analyses were performed. First, a logistic regression model was fitted to evaluate whether non-response in the “In the registry” variable was systematically associated with sociodemographic or health-related predictors (e.g., age, BMI, EQ-5D VAS). No significant associations were detected, suggesting that non-response was not related to observed characteristics. This provides some reassurance regarding the representativeness of the study sample, although we acknowledge that residual bias due to unmeasured factors cannot be completely ruled out.
Second, mean imputation was applied for continuous variables and mode imputation for categorical variables (e.g., BMI, EQ-5D VAS, alcohol), after which the correlation (Spearman) and Chi-square tests were repeated. Although some p-values differed slightly compared with the complete case analysis, no changes were observed in the overall conclusions. These analyses indicate that the main results are stable and not sensitive to the way missing data or non-response were handled. The detailed results from this imputation-based analysis are presented in Table 4.
Results of Sensitivity Analyses Using Mean and Mode Imputation for Missing Data.

A significance level of 0.05 was adopted for all tests (in bold).
BMI - body mass index.
Discussion
The aim of this study was to investigate how sociodemographic factors, health-related factors, and attitudes toward organ donation are associated with whether or not older adults in Sweden are registered in the National Donor Registry.
Discussion of Results
The main findings of this study were that 71% of the participants were positive towards organ donation. However, regardless of their attitudes towards organ donation, only 26% had registered in the National Donor Registry, indicating a significant gap between beliefs and practice. Further, the results show that those with higher health-related quality of life, higher self-assessed health, and unmarried participants were more likely to be in the National Donor Registry. Finally, the results show that those who oppose organ donation were less likely to be in the National Donor Registry.
The discrepancy found between individuals stated attitudes and their actual registration behavior aligns with previous findings (Sutherland et al., 2020). However, explaining the underlying reasons for this gap remains challenging, as most existing studies and statistical reports tend to focus either on general attitudes toward organ donation or on the number of individuals who have registered in national donor registries. One possible explanation for the low number of individuals who have registered a refusal in the present study may be limited public awareness, either of the presumed consent system or of the option to register a “no.” To our knowledge, no studies have specifically investigated public awareness of presumed consent or the procedural possibility of registering a refusal. Another contributing factor may be a tendency to postpone decisions that are perceived as emotionally sensitive or ethically complex (Offer et al., 2025). Research from Australia suggests that offering immediate registration opportunities may be an effective strategy for increasing registration rates (Sharpe et al., 2017; Sutherland et al., 2020). Moreover, negative attitudes toward organ donation have been shown to correlate with procrastination in registration behavior (Sharpe et al., 2017). Although, Australia does not have presumed consent, but an opt-in system. In light of these findings, providing face-to-face opportunities to ask questions about organ donation may facilitate registration in the Swedish context as well. Such interventions could be particularly relevant in settings where older adults are present, and where tailored communication may help bridge attitudinal and behavioral gaps.
The fact that 26% of the participants in this study were registered in the National Donor Registry is a somewhat unexpected finding. 26% is a higher percentage than 18% for the Swedish population in general. This outcome is contrary to previous studies showing that many older adults think that they might be too old or too sick to be a donor, hence opting out of registering (Downing & Jones, 2008, 2018; Febrero et al., 2022). One way to overcome misunderstandings regarding organ donation is, as mentioned above, to provide more information; although, affective attitudes are not easily changed by information (Vorstius Kruijff et al., 2018). Further, both information as well as talking about organ donation can be emotional (Downing & Jones, 2018; Luo et al., 2022; Vorstius Kruijff et al., 2018) and older adults have been shown to be less likely to want more information about organ donation (Södereld et al., 2024).
The present study shows that unmarried individuals were more likely to be registered in the National Donor Registry. A previous study indicated that marital status was not significantly associated with individuals’ awareness of their own willingness to donate organs (Siminoff & Lawrence, 2002). Although, it is not known whether these were preferences communicated through family discussions or documented in any registry. Another study reported that less than a third of older adults had discussed organ donation in a social or family setting (Febrero et al., 2022). Further, a recent Swedish study shows that 42.7% of the participants had not made their preferences known in any way (Södereld et al., 2024). Knowing the patient's preferences regarding organ donation will ease the burden of relatives and make them more comfortable with the decision made, if the situation occurs (Siminoff & Lawrence, 2002).
The most important, and somewhat alarming finding from the present study is that those who oppose organ donation were less likely to be in the National Donor Registry. Only 6.9% of those who oppose organ donation were in the registry. It is stipulated by Swedish law that the patient's autonomy and integrity must be respected during healthcare. In addition, healthcare should, as far as possible, be designed and carried out in collaboration with the patient (Patientlag [Patient Act], 2014). However, Sweden, like many other countries, has what is called presumed consent regarding organ donation (Lag om transplantation mm [Law regarding transplantation etc], 2024). This is an assumption that a patient would have given consent for a certain treatment or procedure, even if the patient has not explicitly done so. Hence, “yes” to organ donation upon death is seen as the default choice. There are discussions about whether it is ethically right to say no to donate (Dalal, 2015). It is not known why individuals opposing organ donation in this study were not listed in the National Donor Registry. Previous research on attitudes towards donation is sparce, particularly within the context of Northern European countries. It is known that context affects peoples’ willingness to register in donor registries (AlHajri et al., 2021). Moreover, the predominant focus of prior studies has been on the perspectives of health care professionals and their views of the challenges and complexity regarding organ donation, leaving the views of the general population comparatively underexplored.
Those who oppose organ donation might not dare to register “no” to organ donation in the National Donor Registry due to social stigma. This situation may increase the risk that health care professionals act against the patient's wishes. This risk is especially significant if the patient has not in any other way shared his or her wishes with relatives or maybe does not have anyone to share this kind of information with. These ethical concerns have also been raised in Denmark, where debates about introducing presumed consent have prompted discussions on autonomy, public trust, and the risk of a pressure to conform. Researchers highlight that presumed consent, if not accompanied by transparent communication and public engagement, may challenge the principle of self-determination (Jensen & Larsen, 2020). To overcome the risk of violating patient autonomy, it is important to increase awareness of the option to register a “no” to donation in the Swedish National Donor Registry. Additionally, the significance of this choice must be communicated, emphasizing that everyone has the right to have their decisions respected. But to enable this, the decision must be known.
Strengths and Limitations
The study uses data from the SNAC, which is a nationally representative, randomly selected cohort of older adults in Sweden. It is a strength of this study that the sampling method helps minimize selection bias and enhances the generalizability of the results to the wider population of older adults in Sweden. Furthermore, the high response rate (74.2%) increases the representativeness of the sample. The relatively large sample size compared to other studies on organ donation attitudes is another strength that further adds to the validity of the results.
Although, some limitations need to be acknowledged. Firstly, the study addresses a topic that can be sensitive to many individuals, which may have introduced social desirability bias. This concept refers to the individuals’ tendency to respond in ways they believe are more socially acceptable or favorable (Caputo, 2017). While the use of an anonymous survey likely minimized this bias, previous research has shown that social desirability can still occur even in anonymous self-administered surveys, particularly when addressing socially sensitive or value-laden topics such as organ donation (Jann et al., 2019; Krumpal, 2013).
Regarding generalizability, the study was conducted on a Swedish sample, so limitations exist when extrapolating the results to other contexts. Also, the fact that only 26% were in the registry must be taken into consideration when interpreting the results. Additionally, in some categorical variables certain response categories were underrepresented, which may have influenced the interpretation of standardized residuals in the chi-square analyses. Lastly, the cross-sectional design used in this study limits the ability to infer causality between the predictor variables and being in the registry.
Implications for Practice
A documented statement of organ donation preferences is crucial for all ages. Making an informed decision on this matter requires information and facts—something health care professionals, especially nurses, can provide. Nurses are often the first point of contact and can identify opportunities to discuss organ donation during routine assessments and/or health education. This will promote adherence to patients’ rights, safeguarding their integrity and freedom of choice in medical care. It is imperative for nurses to encourage registration in the National Donor Registry. Further, it is needed to stress that there is no right or wrong preference; the most important thing is that the preference is documented or mediated in any way. Nurses also require knowledge about the registration procedure. This will enable nurses to provide guidance to patients if such support is requested. Addressing organ donation across multiple settings can be the key to make the topic less emotionally charged and more approachable. However, there is a challenge to reach out with information without causing discomfort and emotional distress, especially to older adults. Here, nursing interventions such as providing individualized information and using a sensitive approach can promote a safe environment where patients feel supported and respected.
Conclusions
A majority of the participants were positive towards organ donation. However, only 26% of the participants were in the National Donor Registry indicating a gap between beliefs and practice. Most of those who oppose organ donation upon death were not in the National Donor Registry, which entails a risk that care will be conducted against their wishes if the question about organ donation arises. Future qualitative studies are needed to gain a deeper understanding regarding older individuals’ attitudes toward organ donation and the sociodemographic factors that influence their attitude. Another important question to answer in future studies is why there is a gap between beliefs and actions regarding organ donation among older adults.
Supplemental Material
sj-docx-1-son-10.1177_23779608251409669 - Supplemental material for Investigating Organ Donation Registration Among Older Adults in Sweden, a Survey Study
Supplemental material, sj-docx-1-son-10.1177_23779608251409669 for Investigating Organ Donation Registration Among Older Adults in Sweden, a Survey Study by Charlotte Romare, Bruna G. Palm and Ana Luiza Dallora in SAGE Open Nursing
Footnotes
Acknowledgements
The authors would like to acknowledge the Participants of the SNAC-IT study. Further, a special thanks to Ulrika Isaksson, database manager at SNAC.
Compliance with Ethical Standards
This study was conducted in compliance with the Declaration of Helsinki and received approval from the Research Ethics Committee at Lund University (LU 604-00, LU 744-00). Written informed consent was obtained from all SNAC participants. All data in this study were anonymized.
Author Contributions
Design and acquisition of data were made by CR and ALD. The analysis of data was made by ALD and BP. All three authors interpreted the data. Drafting the manuscript was mainly done by CR and ALD, with contributions from BP. All three authors have approved the final version of the submitted manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Blekinge Institute of Technology (BTH).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
SNAC data is available upon request through the SNAC application process.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.