
Abstract
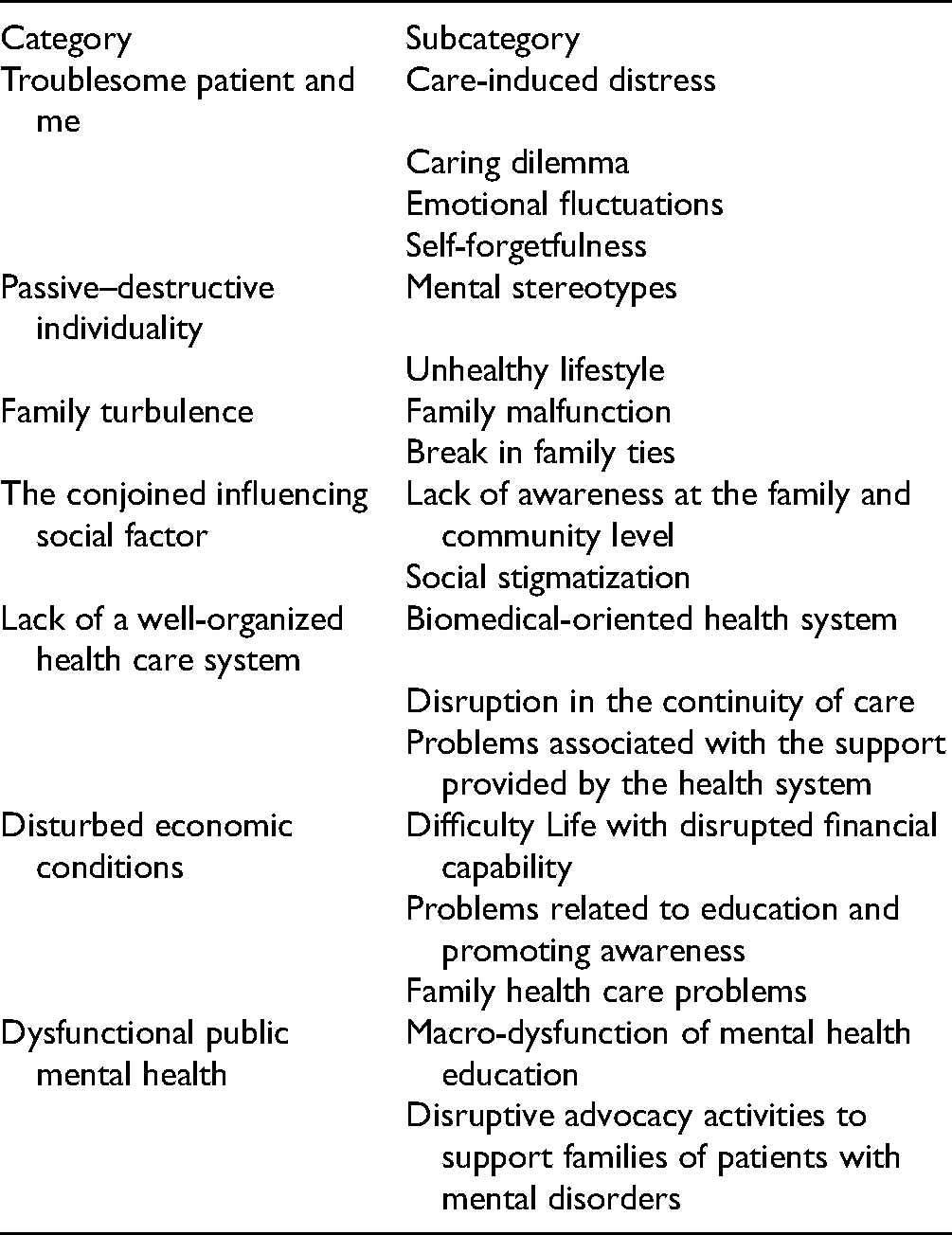
The chronic nature of severe mental illnesses is necessary for constant care provided by the family caregivers. Considering the significance of family caregivers in providing care, it is imperative to ensure their self-care if they are to play the role of caregiving effectively and efficiently well. The present study was conducted using the purposive sampling method and in-depth semi-structured interviews among 13 family caregivers and five health team members. The data were analyzed via a conventional content analysis approach. In the data analysis, seven main categories and 18 subcategories emerged: “A troublesome patient and me,” including “Care-induced distress,” “Caring dilemma,” “Emotional fluctuations,” and “Self-forgetfulness”; “Passive–destructive individuality,” including: “Mental stereotypes” and “Unhealthy lifestyle”; “Family turbulence,” including: “Family malfunction” and “Break in family ties”; “The conjoined influencing social factor,” including “Lack of awareness at the family and community level” and “Social stigmatization”; “lack of well-organized health care system,” including “Biomedical-oriented health system,” “Disruption in continuity of care,” and “Problems associated with the support provided by the health system”; “Disturbed economic conditions,” including “Difficulty in life with disrupted financial capability,” “Problems related to education and promoting awareness,” and “Family health care problems”; “Dysfunctional Public mental health,” including “Macro-dysfunction of mental health education,” and “Disruptive advocacy activities to support families of patients with mental disorders.” There are several barriers to family caregiver self-care planning that require health professionals to develop appropriate interventions.
Introduction
The global increase in mental disorders, whose high prevalence has had a severe impact on the functions of societies, is becoming a serious concern (1). According to the World Health Organization (WHO), one-fourth of households have at least one member suffering from mental disorder cared for by a family members. According to the latest official statistics published by the Ministry of Health and Medical Education and the Statistics Center of Iran, 23.6% of the population aged 15 to 64 years (population in this age range: 55,862,087) held criteria for at least one mental disorder in the last 12 months (2–4). Therefore, the role of informal caregivers of patients (such as family members and friends) with mental disorders should be taken into account (5). Informal caregivers provide most of the long-term care to chronically ill patients (6). These caregivers often report remarkable levels of stress and burden occasioned by the challenges and consequences associated with caregiving roles and responsibilities (5); however, they are required to provide care despite numerous complications (7). Despite some challenges and consequences such as financial strain, emotional distress, social isolation, disruption in work, and other family roles, the caregivers often have to continue the role of caregiving (8). Consequently, caregiver self-care also needs to consider. Caregivers can guarantee a good level of care for others when they practice good self-care (9).
Self-care includes all the behaviors and decisions related to health care that individuals consider to ensure their own and their families’ physical, mental, social, and spiritual health. Caregiver self-care has been considered as self-efficacy and mindfulness (10,11). Self-care in family caregivers (FCs) has been a challenging subject for a while (12). These challenges affect families and ultimately lead to creating health problems for caregivers (13).
Barriers to self-care for the caregivers of patients with mental disorders require further research (6,10–13). The present study seeks to broaden the FCs’ and treatment systems’ horizons concerning barriers to self-care planning for FCs of patients with severe mental illness (SMI) and identify how mental health service providers can help caregivers practice effective self-care.
Methods
Study Design and Participants
The present qualitative study was conducted using the conventional content analysis approach from December 2020 to June 2021. The aim of content analysis is to describe the knowledge and a deeper comprehension of the phenomenon under study. This method supposes that facts are defined in different ways comprehending them is based on subjective explanation and the interaction of the researcher, participants, and values that dominate them (14).
Participants included 13 FCs and five mental health team members (Table 1). This study was carried out in a referral mental health center in Tehran. The inclusion criteria for informal caregivers included caring for a patient with severe mental disorders including schizophrenia, mood disorders (bipolar disorder and major depressive disorder), and schizoaffective disorder, providing care for at least one year and not <21 h per week, and 18 to 65 years of age. The inclusion criteria for selecting mental health team members included at least one year of formal experience related to FCs of patients with severe mental illnesses. Interviews were conducted following obtaining written consent from the participants and approval of the ethics committee. Since the participants included non-English speaking individuals, the interviews were not conducted in English. Therefore, after the completion of interviews and qualitative analysis, the transcripts were translated into English.
Characteristics of Participants.

Procedure and Interview Process
Data collection commenced via face-to-face in-depth, semi-structured interviews, which were directed based on the study purposes and depending on the participants’ responses and emerging concepts. The interviews lasted 54 min on average and continued until data saturation were reached.
Study Analysis
Immediately after each interview, it was transcribed verbatim. Data analysis was performed using Granheim and Lundman's content analysis method. MAXQDA version 10 software was used to manage the data.
Trustworthiness
To establish trustworthiness, credibility was first ensured via prolonged engagement with participants, continuous data comparison, member check, and peer check methods. For conformability, bracketing (suspension of researcher's presuppositions) was performed, and a dependability audit was conducted by three research team members. Finally, to ensure transferability, a rich analytical description of the context, methodology, and limitations was provided.
Ethical Consideration
Ethics Committee of Tehran University of Medical Sciences approved this study (code: IR.TUMS.FNM.REC. 1399.079). Written informed consent and permission to audio-record the interviews were obtained from all study participants.
Results
Eighteen key informants, including caregivers (n = 13) and health team members (n = 5), were extracted in the interview. Participant characteristics are summarized in Table 1. Quotations were coded as FCs and Health Care Team (HCT) and the interview number. The qualitative data analysis results are defined in barriers to self-care planning for FCs of patients with SMI and are provided in Table 2.
Barriers to Self-Care Planning for Family Caregivers of Patients With Severe Mental Illness (SMI).
Troublesome Patient and me
This category included four subcategories:
Care-induced distress. Caregivers provided constant care for the patient, and it had been imposed on them. Moreover, the patient's recovery was gradual, and caregivers felt worn-out and exhausted.Caring for a person with a severe mental disorder puts a lot of pressure on the family; you have to go through it; you have no choice. (FC5) Caring dilemma. Caregivers had encountered various problems in controlling their behaviors and tolerating the patient, felt scared and insecure in relation to the patient, and were sometimes injured by the patient's harmful behaviors.She cries a lot; screams a lot; I don't know how to treat her; I’m afraid of her; She got very angry and said she’d strangle me; She's hit over my head with a mug two or three times. (FC12) Emotional fluctuation. Problems associated with care and recalling unpleasant memories of the patient's behavior had caused apathy, decreased patience, and irritation for caregivers and disturbed their peace.At a certain point, recovery slows down, and you don't get positive results, so you become unmotivated. (FC5) She gets my peace; as soon as I enter the house, the repetition of those behaviors and the events that happen gets on my nerves. (FC7) Self-forgetfulness. Families of SMI patients were unable to engage in their favorite activities, and their entertainment and recreation were disturbed by the care burden. They could not spare time to care for themselves and health care follow-ups. In fact, they had overlooked their needs and considered them their last priority.Caregivers don't spend time for themselves. In fact, they don't have time to go for recreation or do screening and annual examinations; they don't spend any time for their physical and mental health; they ignore themselves. (HCT5)
Passive–Destructive Individuality
This category included two subcategories:
Mental stereotypes. Families with erroneous mental stereotypes about the illness considered themselves the causes of disease and felt guilty and remorse for not pursuing the patient's treatment.Families ask if it was their fault and they’d done something wrong; they believed that they’d neglected the patient, and if they had understood earlier, they would’ve referred sooner. (HCT2) Unhealthy lifestyle. As a result of fatigue and problems resulting from constant care, adverse lifestyle such as sleep disorders or physical activity disruptions become prevalent.I have to get up and give my son his medicines. Then, I can no longer sleep, and I’m pestered because I don't rest and sleep for 8 h; I used to exercise in the morning, but now I’m so tired that I can't get up in the morning, so I don't do it. (FC1)
Family Turbulence
This category included two subcategories:
Family malfunction. The lives of families with SMI patients were in turmoil, and they failed to experience adequate normal conditions. Normally, one family member takes responsibility for caring for the patient, and other members are not engaged in care and support.Family members always have separated with each other; it's never been normal; my father has washed his hands off life and doesn't take any responsibility for my ill mother. (FC7) Break in family ties. Regarding the patient-related problems, conflict had arisen within a family, and members condemned each other. Furthermore, the interpersonal and intimate relationship among the spouses was affected as a result of their busy schedule dealing with the patient. Considering the patient's abnormal behaviors, families had distanced themselves from relatives and cut ties.There's often intense tension within the family; they want to know who was to blame. (HCT2) There's no time for my wife and me to unburden ourselves; we don't visit our relatives because our child isn't well; he talks nonsense or suddenly gets aggressive; it's a real shame for me. (FC2)
The Conjoined Influencing Social Factor
This category included two subcategories:
Lack of awareness at the family and community level. There is unawareness in the family and society concerning mental disorders and self-care.Families don't know much about the illness and how to deal with the patient's delusions and similar issues. (HCT3) There's a lot of unawareness in our society; these issues are a stigma; families don't have enough knowledge and don't know how to take care of themselves and their mental status. (HCT2) Social stigmatization. FCs were concerned about being stigmatized in society. The community's inappropriate reaction had negatively affected their social interactions, and the family was excluded and isolated by society, which ultimately had an adverse impact on family mental health.All families are anxious that relatives and acquaintances will notice the illness, and they’ll be labeled in the family; fear of social disgrace causes them to become more reserved, which puts a lot of mental pressure and stress on them. (HCT2)
Lack of Well-Organized Health Care System
This category included three subcategories:
Biomedical-oriented health system. Physicians emphasize pharmacological interventions, and they do not refer clients to non-pharmacological interventions, including family education. Caregivers expressed inadequacies in the health system.Some residents and psychiatrists don't have a good attitude towards non-pharmacological treatments; their focus is on the pharmacological treatment for the patient. (HCT5) Our health and education systems lack enough determined strategies and an official roadmap. (FC3) Disruption in the continuity of care. Access to health services, including short-term and long-term hospitalization, is limited for patients, and families do not receive adequate support.There’re few public hospitals, and patients are hardly admitted; in our country, there's no standard long-term care center at a reasonable cost. (FC7) Access to mental health services is limited; for example, waiting time for the psychiatric appointment; home care program is not covered by insurance organizations. (HCT5) Problems associated with the support provided by the health system. The health care system and physicians disregard the patients’ families and do not provide them with support.Healthcare system pays very little attention to families; no one cares about the family, and they’re ignored. (HCT5)
Disturbed Economic Conditions
This category included three subcategories:
Difficulty in life with disrupted financial capability. Patients’ families encounter numerous economic problems in life. Financial support in the community is inadequate, and the majority of caregivers do not have the opportunity to engage in recreational activities due to financial problems.I’m a janitor, and my monthly salary is twenty three million Rials ($ 90); how can I buy fruit and rice? People don't help at all; I work, but I have to pay off my debt because our child is in the hospital; I can't travel with my wife or go to our town. (FC2) Problems related to education and promoting awareness. Due to financial problems, patients’ families do not pursue education on mental health as individual or group psychotherapy courses.People are under financial pressure, and it may be difficult for them to pay for the educational course. (HCT5) Family health care problems. The family cannot afford to pay for the patient's medical expenses and multiple hospitalizations, and regarding financial problems, medical follow-ups and family health are marginalized, and the family's self-care behavior is disrupted.My son is getting hospitalized again; I need money to bring him to the hospital; my wife is sick; there's a cyst in her breast; poor her! she's forgotten all about her disease. (FC2)
Dysfunctional Public Mental Health
This category included two subcategories:
Macro-dysfunction of mental health education. General and specialized mental health training for families and the community is defective, indirectly inhibiting caregivers’ self-care.The basis of everything is education; education shouldn't be classical; it should be by case; you can never see a psychiatrist to speak on TV or radio about a mental disorder in a family. It’ll be a kind of care if it happens, which means less effort for me. (FC3) Disruptive advocacy activities to support families of patients with mental disorders. There are macro-level deficiencies in the support provided for families. There is no regulation to support the families of patients with mental disorders as well as agents to pursue advocacy activities.Families’ rights aren't being respected very much. Our country is still unsuccessful in the mental health law that is being passed; families are too involved and worried that they can't be engaged in advocacy activities, or aren't guided properly. (HCT5)
Discussion
In summary, most of the FCs were married and employed. Six caregivers; care duration was less than five years and the rest was more than five years in which four caregivers experienced more than 10 years. Eight patients’ care providers were their parents. The patient's recovery is gradual, and caregivers feel worn-out and exhausted. Caregivers encountered various problems in controlling their behaviors and tolerating the patient, feel scared and insecure in relation to the patient, and are sometimes injured by the patient's harmful behaviors and disturb their peace. Families of SMI patients are unable to engage in their favorite activities and their entertainment. Families feel guilty and remorse for not pursuing the patient's treatment. Families suffer from sleep disorders or physical activity disruptions. Conflicts have arisen within a family and members. Patients and caregivers do not receive adequate medical, financial, psychological, and educational support.
Caregivers take diverse, constant, and intricate responsibilities in the patient management. Numerous studies introduce the burden of care as a barrier to FCs’ self-care (12,15–17). FCs experience feelings such as ineffective coping, chronic stress, and persistent care anxiety (emotional burden) (18) and scarcely care for themselves due to high perceived stress (10) that can be due to multiple factors such as lack of financial, medical, and social support and sometimes stigma. Inadequate time for practicing self-care was expressed by caregivers, which was the same as other studies (19,20), and caregivers were prevented to follow the therapeutical follow-ups; so they encountered self-forgetfulness. Caregivers fail to plan or attend medical appointments (11).
Due to inaccurate mental stereotypes, families consider themselves for the patient's illness. The knowledge of FCs for a proper understanding of rehabilitation and psychiatric recovery concepts is low (13). Complications associated with caregiving have led to caregivers’ unhealthy lifestyle and disturbance in their sleep, physical activities, exercise, and health. According to Wang et al. (11), providing care disrupts caregivers’ ability to maintain a healthy lifestyle.
Families with SMI patients meet a chaotic life. One of the barriers to self-care is the lack of family support (21). Families with SMI patients stated that due to care-related problems, breaking in family ties had occurred within the family and relatives. Previous unresolved family problems, changes in the family life cycle, and a family member with a chronic illness increase the family needs (22).
There are countless deficiencies in the community and family awareness related to mental disorders and caregivers’ self-care. Insufficient knowledge in the caregivers and community has been reported in numerous studies (2,13,15,21). In a study by Wang et al. (11), self-care knowledge was an essential prerequisite and facilitator for achieving caregivers’ self-care management. One of the challenges of mental health care worldwide is labeling and stigmatization (13). The issue of stigma in FCs was confirmed in several studies (13,17,23,24). Stigma excludes the family from society and leads to social isolation (2,18,25). The stigma associated with mental disorders leads to seeking help originating from widespread unawareness about the illness and therefore acts as a mechanism of social exclusion (13).
Numerous problems can be found in providing mental health services to SMI patients and their caregivers. Oliveira et al. (19) identified barriers to dementia caregivers’ self-care as poor management and consistency of services. Families had restricted access to health services and did not receive adequate support and follow-ups. In a study by Tamizi et al. (15), FCs of schizophrenia patients had encountered the challenge of providing inefficient mental health care services and had limited access to services. There are countless challenges to accessing psychiatric prescribers in the United States (26), no specific attention is paid to caregivers of patients with severe mental disorders at the time of admission, transfer, and discharge, and most caregivers are abandoned without support (27). Caregivers’ and patients’ needs for information, education, and medical support are unmet (16,28).
FCs have a lackluster life and disrupted affordability. They are unable to cover treatment expenses, and there is insufficient financial support in the community, which inhibits their self-care behaviors. The results of a study by Daniel et al. (29) showed that financial factors significantly predicted the types of barriers reported by FCs. Caregivers' financial problems have been considered as a barrier to their self-care (19,21).
Macro-dysfunction of mental health education leads to low awareness of the community and caregivers that were reported in our interviews as well in “Lack of awareness at the family and community level” subtheme. Families are unaware of their patient's disorders and coping strategies, which is a secondary yet major barrier to caregivers’ self-care. One of the health system challenges is caregivers’ educational needs, which is consistent with a study by Tamizi et al. (15).
There is no available law to protect the families of patients with mental disorders or agency to implement the advocacy activities of FCs of patients with SMI. The lack of legislation and insufficient public health policies result in system weakness and complicated access to the treatment (13). Caregivers of patients with SMI expect to have representatives in family support organizations to provide them with emotional and operational support at the political level (18). We can say that the most main need for the families with SMI patients is the support of any kind in which we had some subtheme in this regard including difficulty in life with disrupted financial capability, problems associated with the support provided by the health system, and disruptive advocacy activities to support families of patients with mental disorders.
To plan caregiver self-care, individual factors, the patient receiving care, family, community, health system, economic status, macro-level education, and regional laws need to consider. Self-care is an individual as well as a social issue in which various factors such as personal preferences, belief systems, and socio-cultural contexts must be considered (10). Caregivers’ concerns are not taken into account, and these individuals are disregarded and unsupported (27). Consequently, caregivers require special intervention programs to promote self-care. It is strongly suggested to establish organizations to support patients with chronic diseases and caregivers. Awareness of the population of these patients and caregivers can be done in different ways, for example, inquiries from hospitals, offices, clinics, and even the establishment of a national Internet network to report patients with chronic diseases who can provide psychological, financial, medical, social, and recreation support.
Conclusion
Caregiver self-care is critical to managing patients’ and caregivers’ lives, health, and well-being. There are numerous barriers to FC self-care planning (troublesome patient and me, passive–destructive individuality, family turbulence, the conjoined influencing social factor, lack of well-organized health care system, disturbed economic conditions, and dysfunctional public mental health), which provides a broader perspective for mental health team staff and policymakers to understand caregiver needs and take measures to address them. According to the obtained results, it is required to consider potential goals for future interventions assessing multiple aspects of will caregivers’ self-care. Future research and policies should also consider providing better support for specific self-care management in FCs of patients with severe mental illnesses.
Limitations
There were some limitations in this study. The researchers acknowledge that the results of this study cannot be generalized to every caregiver. Participants were non-English speaking individuals; therefore, the article was translated into English after completing the qualitative analysis. In the process of data collection for the research, individuals may have difficulty expressing themselves in a clinical setting, and the interviews can be disrupted. We relied on participant self-report of their experiences, and recall bias is possible.
Footnotes
Authors’ Note
MRK, MACH, NS, ZM, and FN contributed to study conception and design; MRK contributed to data collection; all authors contributed to data analysis and interpretation; MRK and MCH contributed to the drafting of the article, and all authors were involved in critical revision of article.
Ethical Consideration
The Ethics Committee of Tehran University of Medical Sciences approved this study (code: IR.TUMS.FNM.REC. 1399.079). Written informed consent and permission to audio-record the interviews were obtained from all study participants.
Acknowledgments
The authors would like to thank the Tehran University of Medical Sciences which supported this research project. In addition, all the FCs and health care teams who participated in this study would be appreciated.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Tehran University of Medical Sciences.