
Abstract
Background
Mindfulness training has been associated with improved health outcomes among family caregivers of people living with dementia, but access to training is limited, especially in rural areas. Moreover, mindfulness training that addresses the unique perspectives of African American families is needed.
Objectives
The study aimed to test the feasibility and acceptability of a theory-driven, telephone-delivered mindfulness intervention for caregivers of African Americans with moderate-to-severe dementia living in rural eastern North Carolina.
Methods
In this single-arm, multiple-methods study, pairs of informal caregivers attended an 8-week mindfulness training program involving weekly one-hour telephone-delivered sessions, and an online retreat. Feasibility outcomes included enrollment, retention, attendance, and acceptability. Exploratory pre-post endpoints related to our theoretical model included perceived caregiver burden (Zarit Burden Interview), uncertainty intolerance (Intolerance of Uncertainty Scale), and positive emotions (Meaning and Purpose Scale).
Results
Seventy-eight percent of screened individuals enrolled, 86% completed the study, and 88% attended ≥6 sessions. Participants found the program valuable, especially via telephone. Perceived burden decreased from pre-to-post intervention (mean difference [MD] −2.7, (95% CI: −4.5, −1.3; Cohen’s d −0.47) and positive emotions increased (MD 2.7, 95% CI 0.81, 4.5; d = 0.37). Both inhibitory (MD -1.0, 95% CI -1.8, −0.09; d = −0.28) and prospective (MD -1.2, 95% CI -2.7, 0.3; d = −0.20) intolerance of uncertainty were lower post-intervention.
Discussion
A telephone-delivered mindfulness training intervention was feasible and shows promise for reducing perceived burden among rural-dwelling informal caregivers of African Americans with dementia. Further testing in a randomized parallel-group trial comparing mindfulness training to a credible control intervention is warranted.
Trial registration
ClinicalTrials.gov NCT04058886.
Introduction
Providing care for a loved one with dementia is associated with emotional, financial, and physical costs1,2 Caregivers of a family member with dementia report higher rates of stress, anxiety, depression, and poor physical health compared with other caregivers and have higher rates of family conflict.5,15,23-25 As with many other diseases, the cost of Alzheimer’s disease and related dementias (ADRD) takes a higher toll for many in minority racial and/or low-income groups. The costs for African American caregivers often include higher caregiving hours and lower levels of formal service use, as compared with other caregivers.3,4 These costs may be greater for African American caregivers and their families in rural areas, who may have limited access to resources to help manage caregiving stress and any associated family conflict. 5
In addition to increased costs and limited access to resources for African American caregivers, existing programs may not address the unique circumstances for caregivers in this group. For example, several authors describe cultural considerations that mark caregiving experiences for African Americans.6-10 They conclude that culturally congruent and family-centered approaches are needed to ensure that interventions do not ‘miss the mark’. 11
Mindfulness training, in which participants are taught to regulate attention to present-moment experience via behavioral techniques such as mindfulness of breathing, has been documented as both feasible and culturally acceptable in African American adults.12-14 In addition, a systematic review has shown the feasibility, acceptability, and improved health outcomes of mindfulness training interventions for caregivers of family members with dementia. 2 In another review, including a network meta-analysis, researchers found that mindfulness-based interventions were associated with a moderate effect on perceived caregiver burden. 41 However, little is known about the outcomes of mindfulness programs for caregivers of African Americans with dementia, particularly those living in rural areas, where typical in-person formats for mindfulness training are less accessible. 15 Moreover, most mindfulness training programs lack an emphasis on family relationships, which may be particularly pertinent to informal caregiving for rural African Americans with long-term illnesses such as dementia. Therefore, this study developed and tested the feasibility of offering a telephone-based, family-centered mindfulness training program to pairs of rural family ADRD caregivers to ease caregiver burden and enhance family functioning.
The purpose of the current study was to explore the following specific aims: (1) To determine the feasibility and acceptability of a telephone-delivered mindfulness training intervention in decreasing perceived caregiver burden among rural, informal caregiving teams of African American people with dementia; (2) to explore, on a preliminary basis, the effects of the training on perceived caregiver burden and relevant secondary outcomes for both caregiving team members, including emotional regulation, tolerance of uncertainty, emotional and physical health, and family conflict.
Methods
Conceptual Model
The designed intervention and selected measures were based on a conceptual model developed for the study. The conceptual model (Figure 1) combines Pearlin’s Stress Process Model
16
with Mishel’s Reconceptualized Uncertainty in Illness Theory.17,18 Pearlin proposed a complex model of caregiver stress involving multiple mediating and interacting components, including background and context (e.g., family and network composition), primary stressors (e.g., problematic behaviors of the care recipient, secondary role strains such as family conflict), secondary intrapsychic strains (e.g., role captivity), mediators (e.g., coping), and outcomes (e.g., anxiety). In our study, Pearlin’s model was simplified in the following ways. We expected that mindfulness training would increase positive coping strategies and cognitive flexibility, reduce family conflict, and reduce perceived caregiving burden, as well as improve outcomes associated with elevated levels of burden such as anxiety, anger, and poor physical health. To address cognitive flexibility, a demonstrated outcome of mindfulness training, Mishel’s reconceptualization of uncertainty was added to the model.
18
Mishel’s reconceptualized theory of uncertainty posits that, although uncertainty is usually an aversive experience, the uncertainty inherent in chronic illness can result in a probabilistic rather than a mechanistic worldview allowing the individual to accept uncertainty as a natural part of life. Mindfulness training, with its emphasis on acceptance of what is, would be expected to enhance the transition from uncertainty as a negative experience to one that is accommodated. This transition is further enhanced through the support of others who share the expanded approach to uncertainty.
18
Conceptual model guiding the Mindful Coping and Communication in Caregiving intervention for rural Black/African American family caregivers of people living with dementia Abbreviations: CR = Care Recipient Constructs presented in darker text were measured and reported here.
In addition to the original model, the team included positive psychology concepts as part of the process of tailoring the intervention to a rural Black/African American population. Specifically, the intervention included an awareness of strengths and an appreciation for resilience amid difficulties. These concepts are discussed in greater detail below.
Study Design
This mixed-methods study used a pre-post design to assess the feasibility and acceptability of telephone-delivered mindfulness training for rural caregivers of African American individuals with moderate to severe dementia. Feasibility metrics included an 85% study retention rate and completion of at least 6 of the 8 intervention sessions. Acceptability was defined through post-participation interviews.
Inclusion and Exclusion Criteria.

aCaregivers and care partners were considered cognitively impaired if, in the assessment of the interviewer, they were unable to answer questions coherently and express understanding of the consent form.
Recruitment, Screening, and Enrollment
Research team members presented the study and distributed study flyers to local community organizations, doctor’s offices, and hospitals. The local Council on Aging, local caregiver support groups, local churches, and medical providers referred community members to the study. Potential participants accessed the study website and completed a brief pre-screening questionnaire. Potential primary caregiver participants were eligible to be contacted if they were living in a rural county in Eastern North Carolina and caring for a Black/African American individual living with dementia. Based on the pre-screening, all 77 potential participants were contacted by telephone to set up a screening and enrollment visit. Initially, primary caregivers were screened and enrolled in the home and care partners were enrolled by telephone, but after March 2020, because of the COVID-19 pandemic, all participants supplied verbal informed consents and were screened and enrolled by telephone. Screening, also done over the telephone during the pandemic, included an assessment of cognitive impairment using the AD-8 Dementia Screening Tool19,20 and the Functional Activities Questionnaire (FAQ). 21 A score of at least 2 on the AD-8 or at least 8 on the FAQ conferred eligibility (Table 1). If eligible, participants completed a set of questionnaires administered by the research staff, including the Functional Assessment Staging Tool for dementia (FAST) to assess the degree of impairment due to dementia as perceived by the primary caregiver. 22 Once four pairs of caregiving teams (primary caregiver and care partner) were assembled, the intervention began. All study procedures were reviewed and approved by the Institutional Review Board of the University of North Carolina at Chapel Hill.
Stakeholder Engagement
Initially, based on intensive in-person community engagement efforts, the research study was planned exclusively in two counties in rural eastern NC. Community engagement was deemed important to the conduct of the study and was initiated after grant funding was received. To facilitate engagement, a community advisory board (CAB) was recruited. The CAB evaluated and made recommendations regarding presentation of mindfulness concepts and participated in decisions regarding recruitment. To recruit CAB members, research team members compiled a contact list of organizations and businesses that provided services to older adults, persons with ADRD, and their caregivers. These organizations and businesses included local doctor’s offices, hospitals, respite groups, in-home care providers, Area Agencies on Aging (AAA), ADRD support groups, and local churches. Potential CAB members were contacted via email, telephone, and in-person at local community events. Additional members were found using a snowball sampling technique. 23 The research team aimed to recruit a CAB consisting of clinicians, faith leaders, community members, and caregivers with experience both working with rural African American families, and with caregivers of patients with ADRD.
Five community members were successfully recruited to the CAB. These members included two staff members from a rural AAA, including the executive director and the director of caregiver education programming, both white women. These staff members had years of experience engaging with community members around issues facing older adults, working with African American families in rural NC, and leading educational offerings for caregivers. The other three CAB members had lived experience as African American caregivers of rural older adults with dementia.
With the pivot to remote activities due to the COVID-19 pandemic, recruitment was expanded to all rural areas in eastern NC. An online summit was held with representatives from senior centers across eastern NC to explain the purpose of the study, introduce mindfulness, and encourage participant referrals to the study. The first CAB meeting was held in person and introduced members to one another and to the research team, provided an overview of the current project, introduced the importance of stakeholder engagement, and supplied tips for successful community-academic partnership building. The first meeting also included an overall introduction to research, expectations and benefits of participation as a stakeholder, and participation in experiential mindfulness activities. Stakeholders were asked to recommend recruitment strategies and caregiver resources to include in the participant resource guide.
CAB members evaluated intervention components both experientially and through review of language in the mindfulness curriculum, making suggestions for improvements where needed. CAB members actively took part in the mindfulness session with the instructor and reported gaining tremendous benefit and increased understanding of the program after participating.
Recommended pre-pandemic recruitment strategies included recruiting from in-person events at local senior centers and businesses. Once the COVID-19 pandemic began, strategies shifted to connecting with the AAA program director to coordinate handing out flyers when doing Meals on Wheels programs, and Facebook advertising.
Intervention
The study intervention was based on a Mindfulness-based Stress Reduction (MBSR) format, 24 but modified in several ways to address our conceptual model as well as to fit the pragmatic needs of rural caregivers and their care partners. To enhance cultural congruence, we selected certified MBSR instructors who were Black/African American. One of our instructors, an Black/African American male who was familiar with the culture and language characteristics of Black men and women in the rural southern United States, was available to offer feedback on tailoring of the intervention. Our other certified MBSR instructor was a Black woman who likewise was familiar and comfortable with Southern Black idioms and culture.
Because we were interested in enhancing family function, we included as participants caregiving dyads consisting of caregivers (CG) and their self-selected care partners (CP). Up to four CG-CP dyads participated in the mindfulness training sessions. Because caregivers of individuals with ADRD had neither the time nor the ability to travel to participate in mindfulness training, the program was offered over the telephone in 8 weekly one-hour sessions. The telephone was chosen to mitigate the barriers to participation inherent in spotty internet service in some rural areas, in addition to potential lack of comfort with internet-based technology. Adaptation of MBSR to the telephone was facilitated by consultation with an experienced MBSR instructor (MB) who had extensive experience teaching MBSR to groups over the telephone. Caregivers received instructions on how to call in to the group teleconference on Zoom using either a password protected secure link or specific number and access code. Initially, a 3-hour in-person retreat (with respite care as needed) was planned but had to be abandoned after the onset of the pandemic. It was replaced by a 2.5-hour retreat by teleconference.
Since family conflict is a significant source of stress in caregiving situations and is associated with high caregiver burden and negative outcomes, we included curriculum content in established MBSR techniques such as mindfulness of breathing (sitting meditation), mindfulness of sound, mindful eating, body scan, walking meditation, breathing space, mindful presence (including experiencing thoughts and emotions) and compassion practices, as well as instruction in mindful “relaxation breathing” (paced breathing), mindful listening and mindful communication. Training in mindful listening was introduced in session four, with a mindful communication exercise between CG-CP dyads introduced during the retreat (held between sessions 5 and 6). CG-CP dyads were encouraged to practice mindful communication both formally and informally, between sessions.
Final Components of the Telephone-Based Mindfulness Intervention.
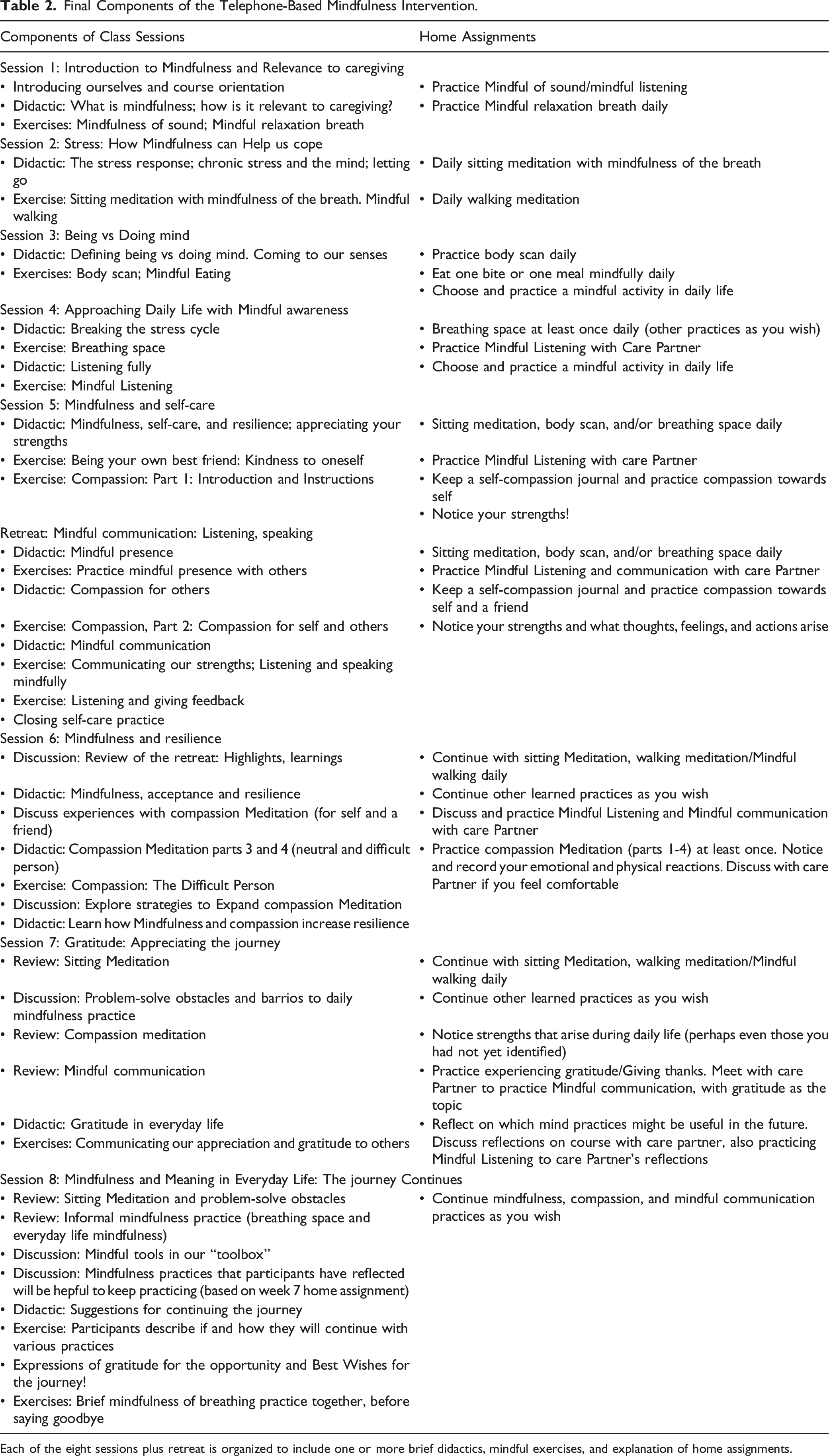
Each of the eight sessions plus retreat is organized to include one or more brief didactics, mindful exercises, and explanation of home assignments.
The sessions were taught by one of two experienced MBSR instructors. Homework assignments consisted of practicing the techniques presented in the sessions with the support of recordings. CG-CP dyads were encouraged to communicate (via telephone or in person) about weekly home assignments. The 2.5-hour retreat, initially undertaken as a three-hour in-person meeting at a local senior center, was held over Zoom during the pandemic. The retreat involved reviewing mindful practices as well as focusing on mindful communication skill development; subsequent home assignments included mindful communication between caregiving dyads. Two manuals were created—one manual to guide the instructor in facilitating the intervention, and one to guide the CG-CP dyads as they participated in the intervention. To facilitate fidelity assessments, with the permission of the participants, all intervention sessions were audio recorded.
Participants received a binder containing a participant mindfulness-training manual that included information about each training session, instructions pertaining to each mindfulness exercise, other handouts, and directions for accessing the mindfulness recordings. In addition, the binder included information about local and national resources for caregivers of persons living with ADRD. In four of the cohorts (cohorts 4-8, n = 12), the primary caregivers also received the same information on an electronic study tablet that included tagged online links to caregiving resources. The purpose of the tablets was to evaluate if participants found them more useful than the printed handbooks for accessing these resources.
Outcome Measures
Feasibility and Acceptability
Feasibility, the primary outcome, was measured by the following: (1) percentage of individuals expressing interest who enrolled in the trial (benchmark: 50%); (2) percentage of enrolled participants who attended at least 6 of the 8 intervention sessions (benchmark: 80%); and (3) percentage of enrolled participants who completed the study (benchmark: 85%). Attendance can also be considered a measure of acceptability.
Acceptability was also measured qualitatively via post-participation interviews that asked open-ended questions designed to assess what aspects of the intervention the participants found beneficial/useful, and difficult, and whether mindfulness training was perceived as a good fit. From the interviews, acceptability was defined as the percentage of participants expressing comfort with the intervention components and home assignments. These interviews also investigated the timing and setting of the intervention. The interviews were conducted by study staff (investigators, research fellows, research assistants) within three weeks of the end of the intervention. The 30-minute interviews were recorded, transcribed, and transcriptions were reviewed for accuracy prior to analysis.
Exploratory Pre-post Endpoints
Multiple exploratory pre-post endpoints were assessed through targeted questionnaires based on the study’s conceptual model. Here we present data on measures key to understanding feasibility and the intrapersonal impact of the intervention, including a primary stressor (appraisal of neuropsychiatric symptoms), key outcomes (caregiver burden and self-efficacy), potential mediating variables (coping, intolerance of uncertainty, self-efficacy for managing emotions) and caregiver health outcomes (emotional distress, global physical health, and meaning and purpose). Additional details are available in our previous publication of the study protocol. 29 Please note that variables pertaining to family function are reported in a companion paper. 30
Caregiver Burden
The ZBI was developed to assess burden among caregivers of persons with cognitive impairment. 31 To reduce participant burden, this study used the shortened 12-item version, which was highly correlated with the longer version 32 and exhibited good discrimination. 33 Items are scored as occurring never (0) to almost always (5) and are summed for a total score.
Caregiver Distress Associated With Neuropsychiatric Symptoms
The Neuropsychiatric Inventory (NPI) measures the severity of neuropsychiatric symptoms such as delusions and the degree to which the caregiver is disturbed by the symptoms. 34 This study focuses on the degree to which caregivers are disturbed by the symptoms as an outcome likely to be impacted by mindfulness.
Self-Efficacy
The Patient-Reported Outcomes Measurement Information System (PROMIS) general and emotion self-management short forms were developed in collaboration with the National Institutes of Health to create population-normed measures with high reliability, validity, and precision. 35 Convergent validity with other self-report measures has been shown. 35
Coping Styles
The Cognitive Emotion Regulation Questionnaire (CERQ) measures cognitive strategies for coping with events perceived as negative in 9 domains: Self-blame, Acceptance, Rumination, Positive refocusing, Refocus on planning, Positive reappraisal, Putting into perspective, Catastrophizing, and Blaming others. Reliability and convergent validity of the original scale was good. This study used the shortened, 18-item form of the questionnaire which also has positive psychometric properties. 36
Uncertainty Tolerance
This study used the 12-item version of the Intolerance of Uncertainty Scale (IUS). 37 Prospective intolerance of uncertainty (IU) involves cognition to reduce uncertainty of future events; (Example: “One should always look ahead so as to avoid surprises”). Inhibitory IU involves avoidance of uncertainty through one’s behavior (example: “The smallest doubt stops me from acting”). The subscales show high reliability). 38
Emotional Distress
PROMIS anger and anxiety short forms measure constructs related to emotional distress. Both scales are measured over 7 days and are reportedly responsive to change. 39
Perceived Health
The PROMIS global health short form measures general self-rated physical health, function, pain, and fatigue with a marginal reliability of 0.81. 40
Meaning and Purpose
The population normed PROMIS Meaning and Purpose scale assesses positive emotions and overall well-being. The measure has good internal consistency and convergent validity. 41
Mindfulness
Mindfulness was assessed with the Cognitive and Affective Mindfulness Scale-Revised (CAMS-R). 42 The CAMS-R has acceptable internal consistency and both convergent and discriminant validity. It addresses four facets of mindfulness: attention, present focus, awareness, and acceptance. The authors recommend that the global score be used as the internal consistency of the facets is not high. 42
Analyses
Quantitative Analysis
For all quantitative questionnaire measures, the outcome is the change in the measure from baseline to post-participation. After examining variable distributions and missing data patterns, we conducted exploratory, descriptive analyses to assess patterns of change associated with participation in the programs for each of the outcomes. We explored the endpoints using repeated measures mixed models with individuals nested in families nested in cohorts as random effects. We adjusted for primary caregiver vs care partner status and the degree of impairment of the care recipient as measured by the Functional Assessment Staging Test (FAST) for dementia. 43 In this small study, it was not possible to formally assess subgroups, mediation, or adjust models for gender, age, or relationship to the caregiver. All analyses were conducted using Stata software (StataCorp. 2019. Stata Statistical Software: Release 16. College Station, TX: StataCorp LLC).
Qualitative Analysis
Post-participation interviews with study participants provided qualitative data for analysis of acceptability. Informal qualitative data collected from CAB members and recruitment partners were added to the interpretation of the findings. Interviews were conducted by a trained research assistant or postdoctoral fellow via telephone. The post-participation interviews were recorded and transcribed by Otter. ai software. Team members compared the transcriptions to the recorded audio file to check for accuracy. Interview questions pertaining to acceptability sought participant feedback regarding the timing and logistics of the intervention as well as feedback concerning completing the intervention with their care partner. In total, 51 participants completed the post-participation interview.
One research team member performed the initial analysis, coding each transcript using Atlas. ti to assign descriptive meaning to sections of the data. 44 Other trained study team members checked the initial coding for quality, read assigned transcripts and reviewed the preliminary codes to confirm that they accurately reflected the data, adding more codes where appropriate. The team met regularly via email and virtual meetings to discuss the coding process and to clarify descriptive codes that did not adequately reflect the data. Decisions to keep, clarify, or discard specific codes were documented in an audit trail to maintain transparency and promote dependability, a benchmark of qualitative rigor.45,46 After all codes were finalized, a detailed codebook was created, which included each code, its definition, and an example quote, along with any comments. Team members then grouped similar codes so that patterns could be identified. Themes pertaining to acceptability were determined from the observed patterns The qualitative analysis team also met to discuss pertinent examples of participant feedback regarding acceptability of the mindfulness training and receipt of the included electronic tablet. In addition, notes from CAB meetings were reviewed for other perspectives, though data were not collected formally from CAB participants.
Results
Description of the Sample
Characteristics of the Sample of Caregivers.
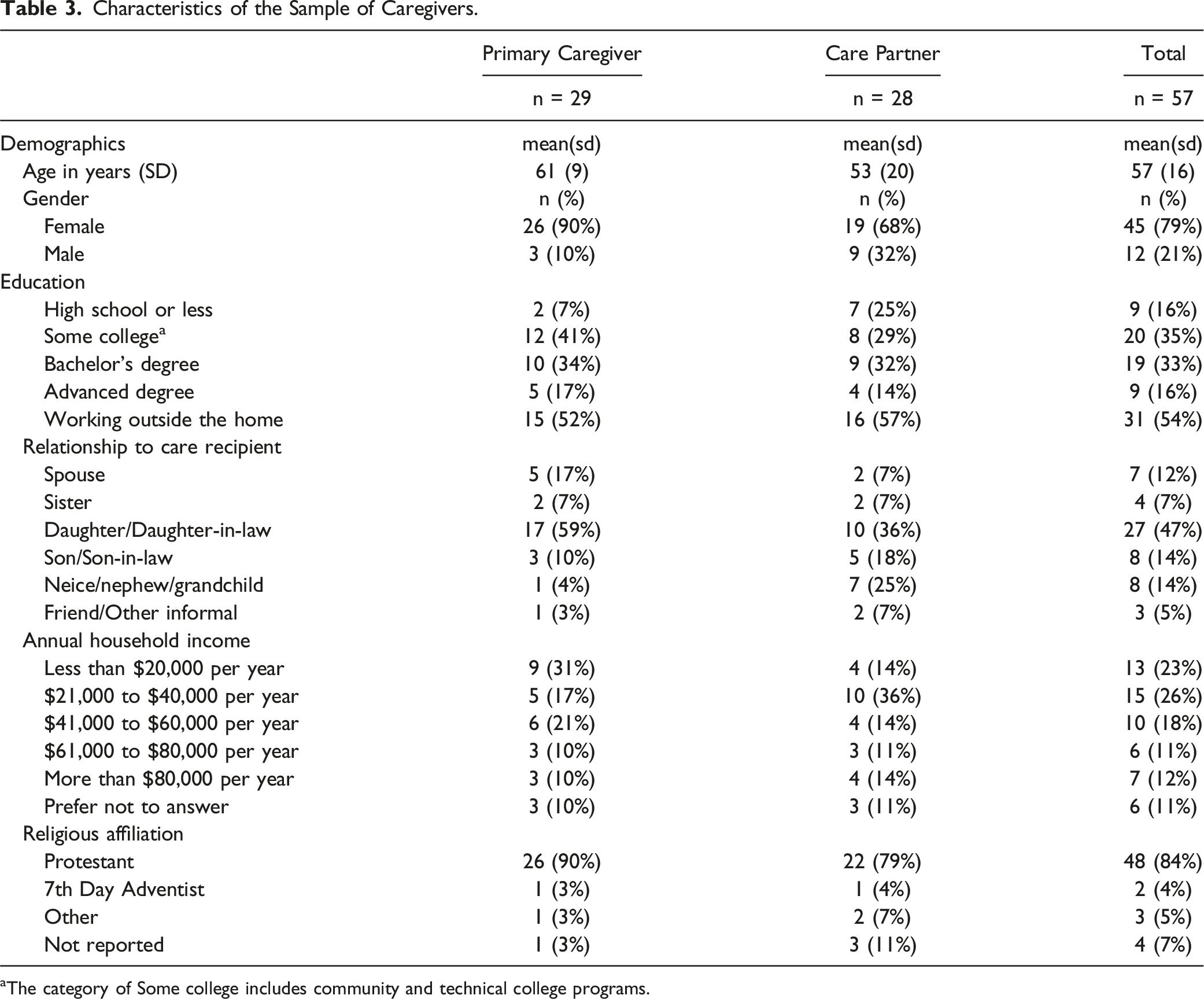
aThe category of Some college includes community and technical college programs.
Feasibility: Enrollment, Completion, Attendance
Among the 77 screened caregivers and care partners, 60/77 (77.9%) enrolled in the study. Five were not interested, two did not have time to participate, five were unable to find a care partner, one had concerns about COVID-19, and four were ineligible for other reasons. Sixty individuals enrolled in the study, and fifty-seven took part in one of nine cohorts of the intervention—one withdrew due to a new job, and a pair withdrew due to illness before the start of the intervention (Figure 2). Four individuals withdrew after the start of the intervention due to family illness, and one withdrew due to difficulties related to hearing loss. Hence, we conducted nine cohorts of the intervention with 57 individuals. Of the 57, 87.7 percent attended six or more of the 8 sessions, and 52 did not withdraw from the study and were considered to have completed the study. Of the 52, 51 completed all post-participation assessments including the post-participation interview. Hence, the retention rate was 52/60 or 86.7% and the rate of measure completion was 51/60 or 85%, thereby meeting our benchmark. One of the 52 was unable to participate in the post-intervention interview. Study Flow diagram for Mindful Coping and Communication in Caregiving.
CAB members assisted with engaging local organizations to distribute flyers and inform senior center staff about the study and reported high engagement from local partners.
Acceptability: Interview Data
Acceptability of Class and Program Length
Among those who responded to a question about the length of the program, 74% thought it was about right. Sixteen percent thought it could be shorter (e.g., 6 weeks), especially if the program were occurring around a holiday and 9% said the program was too short. Several respondents suggested a post-program refresher, reunion, or retreat.
Over 90% of respondents felt that the length of the class sessions (about an hour) was about right. They noted that sometimes the class did not start on time, because the instructor was courteously waiting for others to join, but that added time. One person suggested a gathering time followed by a hard start. A few people thought the class could be longer. Similarly, more than 90% of respondents thought the class was at the right time of day (7 pm). A few wanted an earlier start, and a few wanted a later start. Several participants said that no other time would have been better. Regarding the training period, one participant (ID149) summarized, “I must be clear it really…wasn’t too long or too short. And each time it was like it could have…stood alone, independent of the other. And yet, it…was fantastic. So, there was…closure on each evening.”
Acceptability of Telephone-Based Training
While some respondents said that they missed seeing other caregivers face-to-face, the majority said that completing the training via telephone was both feasible and acceptable. Several participants asserted that learning mindfulness over the telephone enabled them to focus more completely on the training. One respondent (ID4) said, “I was more relaxed. I didn’t have any distractions. I didn’t have to worry…about looking and feeling or any of that, and not [being] looked at [by] anybody else, I really enjoy [being] able to just kind of be free and do it.”
Another participant (ID148) observed that completing the training at home via telephone enabled her to spend more quality time with her care partner, her husband. She said, “I was just able to listen and not have to be distracted because of what was going on. Or what could have gone on in a group setting. My husband and I usually sit in the same space. We would sit side by side when we would do that. So, there was a time to…kind of share with him too in what was going on.”
Acceptability with Respect to Reducing Perceived Caregiver Burden
Many participants found the training to be helpful in reducing caregiving burden, as they learned how to better support their caregiving partner. For example, one participant (ID143) said, “I… was able to see what she was going through in comparison to what I’m doing. And the fact that she’s there. And, you know, hands on. And I’m trying to be helpful. Say okay, what can I do, to lighten…the burden off her by not being there? And one of the things that I have learned that just the fact that knowing that someone else cares and knowing that someone else is there…That makes a difference.”
Other participants acknowledged that the training enabled them to better shoulder the caregiving burden. Participant 106 said, “I’m still a caregiver. So, it’s not like this experience decreased the load that I carry. I just think it’s having the knowledge of…I have a tool that can help me sort of look into how I’m going to care for myself and caring for myself better or to not be carrying the stress, or recognizing when stress triggers are manifesting; that I have techniques for coping with that.”
All but one of the 51 individuals who completed the post-participation interviews felt that the program was a good fit for them. One respondent (ID150) affirmed, “The study helped me to realize I got to take it one day at a time. Don’t think about the future, the past, just think about that day, what I can do that day and what I can’t, and not feel guilty about things I can’t do.”
Quantitative Measures
Change in Measures From Pre-to-post-intervention (Adjusted).
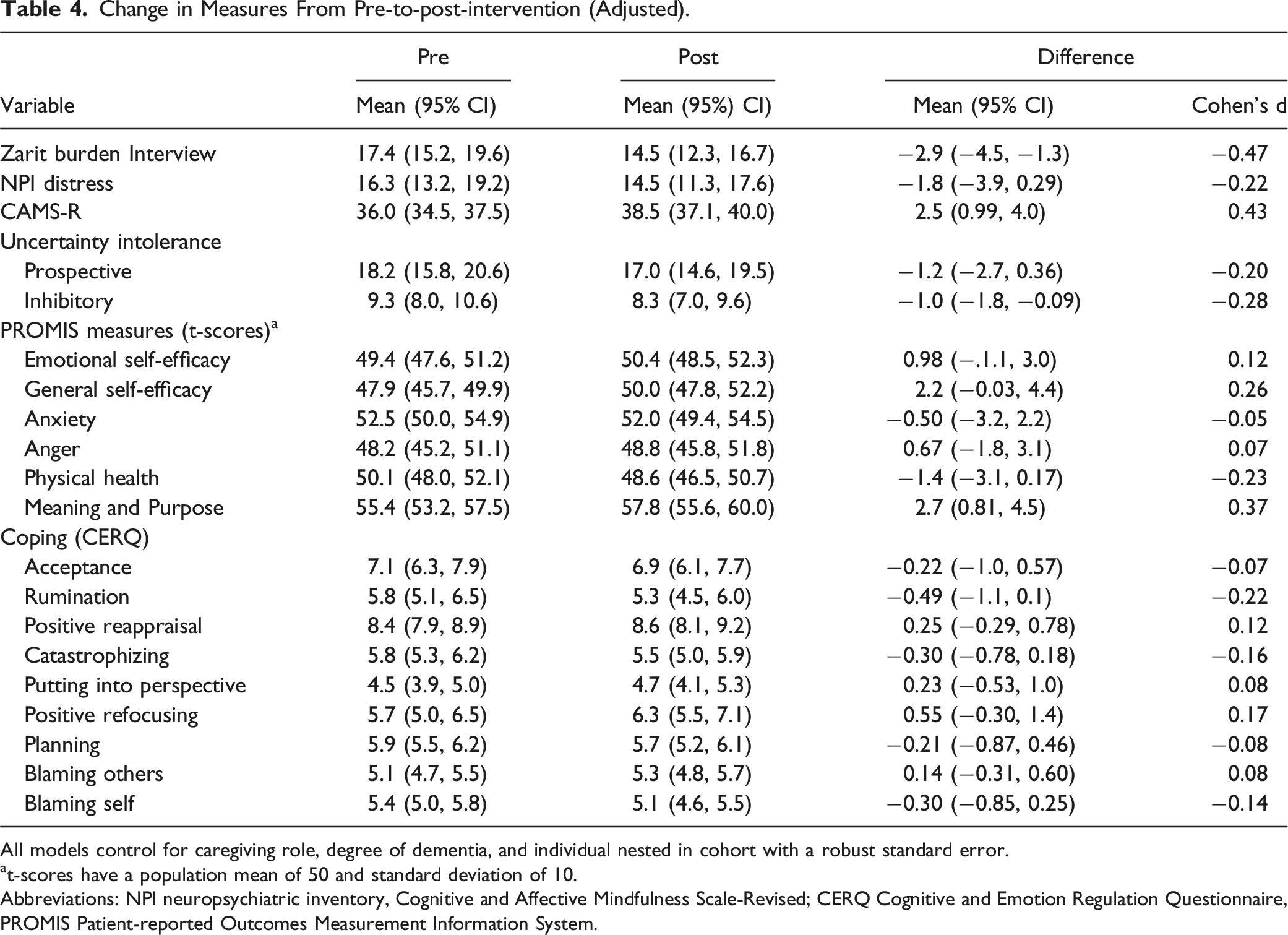
All models control for caregiving role, degree of dementia, and individual nested in cohort with a robust standard error.
at-scores have a population mean of 50 and standard deviation of 10.
Abbreviations: NPI neuropsychiatric inventory, Cognitive and Affective Mindfulness Scale-Revised; CERQ Cognitive and Emotion Regulation Questionnaire, PROMIS Patient-reported Outcomes Measurement Information System.
Discussion
The results of this research study significantly strengthen the empirical evidence that a telephone-delivered culturally tailored mindfulness training program is acceptable, feasible, and helpful for African American caregivers. Ninety-five percent (57/60) of enrolled caregivers participated in the intervention and 86.7% (52/60) of enrollees completed the 8-week intervention. Ninety-eight percent (50/51) felt that the program was a good fit for them. In terms of telephone delivery, the majority stated that completing the training via telephone was feasible, acceptable, and facilitated their ability to participate. Several participants added that learning mindfulness over the telephone enabled them to focus more completely on the training.
Many of our intentional decisions mirrored those of Watson-Singleton et al, (2019) 14 for providing a culturally responsive mindfulness-based intervention for African Americans. One such strategy was the intentional choice that a Black/African American certified in MBSR training serve as instructor/facilitator for the group and participate in intervention development. In addition, we added a mindfulness-based exercise involving awareness of personal strengths and their impact on daily life challenges.
While the eligibility requirement that a care partner take part in the intervention posed difficulty for some of the participants, the inclusion of a care partner was an often-mentioned benefit for many of the CG-CP dyads. This finding supports those of Berk et al (2018) that participating in a group with a partner was valuable and had a positive influence on their relationship. 47 The dyad in their study consisted of the caregiver and the person living with dementia. Our study, designed for caregivers of persons with moderate-to-severe dementia, extends this benefit to caregiving pairs (CG-CP dyads).
Our findings are also consistent with other group-based mindfulness interventions that document an association with decreased perceived caregiver burden. 48 We found that caregiver burden decreased significantly from before to after the intervention. However, the improvement in perceived caregiver burden did not differ significantly by caregiving role (primary vs care-partner We also found that the pattern of changes in coping strategies (reduced rumination, self-blame, catastrophizing and increased positive reappraisal) were consistent with improvement expectations. In addition, participation in the mindfulness intervention was associated with an increase in positive emotions as measured by the PROMIS Meaning and Purpose Scale as is consistent with prior expectations of mindfulness benefits. 49
Our findings support the use of a culturally congruent mindfulness training intervention for caregivers in rural areas who are providing care for older African Americans with ADRD. The Mindfulness training intervention was accessible by telephone, thereby eliminating the need to travel to an intervention site and simplifying the pivot to a fully remote study in response to the COVID-19 pandemic.
Study Limitations and Strengths
This study was designed to develop and determine the feasibility and acceptability of a telephone-delivered, culturally tailored mindfulness training intervention to reduce perceived caregiver burden in rural ADRD caregivers and their care partners who were caring informally for African American family members. Without a control group, pre-post differences cannot be clearly attributed to the intervention. However, the feasibility metrics and qualitative findings support its assessment as a feasible intervention. Moreover, our community partners were enthusiastic about the intervention and its potential to benefit their constituents. In particular, they recommended that the mindfulness intervention be implemented through state agencies as an option for caregiving families.
Additional limitations include the fact that, in our sample population, 49% had a college education. This may not be representative of the larger population of caregivers of people living with dementia in eastern North Carolina making the results less generalizable.
Strengths of the study include its innovative, theory-based intervention, multiple methods design and in-depth focus on caregivers of African Americans with ADRD. Research has shown that this subgroup of caregivers benefits when an intervention addresses their cultural values, and this study reflects our recognition of the need to address culture and context in this subgroup of ADRD caregivers. 4
Conclusion
The needs of family caregivers are great, and there is a substantial need for caregiving resources that families can access easily and that are effective in reducing burden. This telephone-delivered mindfulness intervention provided participants with an applicable and helpful skill in a delivery format that was both feasible and accessible for a rural population with a high caregiving burden. The findings of this feasibility study are encouraging and call for further investigation in a parallel group randomized controlled trial.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Kessonga Giscombé is currently employed with Headspace, Inc. His employment there began after he participated in the development of this intervention. The authors declare no conflicts of interest associated with this work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Center for Advancing Translational Sciences (UL1TR002489), National Institute on Aging (R21AG061728), National Center for Complementary and Integrative Health (T32AT003378).