
Abstract
Singapore's growing elderly population faces a rising burden of chronic wounds. Studies have shown the beneficial effects of shared wound management where the patient actively manages their wound with guidance from their healthcare professionals. However, this concept faces challenges due to patient resistance. This study investigates barriers hindering patients’ participation in self-wound care. Addressing these barriers to aid the development of targeted strategies can increase the uptake of self-wound care. A locally validated survey was conducted among 328 patients in the polyclinics to assess their hesitancy toward self-wound care. A lower score on the scale indicated a high hesitation toward the concept of self-wound care. Forty-five percent of the participants expressed hesitation toward self-care. Strong family support emerged as a crucial factor in encouraging participation. Conversely, concerns about improper technique, missed diagnoses, and wound infection were prevalent. Logistic difficulties also influenced anxieties. Younger patients and those with higher education exhibited less apprehension. Educational interventions, tailored to address anxieties and empower patients with proper techniques, are critical. Fostering communication within families and examining the process of acquiring wound dressing materials are crucial in overcoming these barriers to self-wound care.
Keywords
Background
Self-wound care requires active patient participation and engagement in the wound management process. In Singapore's primary healthcare, the common wound types encountered are diabetic foot ulcers, chronic leg ulcers, pressure injuries, skin tears, and acute wounds such as lacerations and abrasions.
A study by Lo et al 1 revealed the high cost associated with wound care in Singapore. In 2017, the average hospital stay for a wound episode approached 18 days, incurring a cost of nearly $18 000 per case. The national expenditure on wound care for that year was a staggering $322 million, significantly impacting both hospitals and primary care facilities. 1 The burden of wound care is further amplified by frequent readmissions; over 40% of patients required multiple hospital visits within a year. 1 Brown 2 highlights nursing time as a key factor contributing to rising healthcare costs, as many patients require frequent wound care visits.
A growing trend emphasizes the importance of patient participation in wound care as a potential solution. 3 A collaborative approach, known as shared wound care, has shown promise in promoting healing for various wounds, including surgical incisions, accidental injuries, injection sites, abscesses, infected skin areas, and cellulitis. 4 In Singapore primary healthcare context, shared wound care is characterized by having patients, family members, physicians, and nurses jointly participate in the management and treatment of wounds. This model requires active patient involvement in their wound care routine, encompassing tasks like cleaning, dressing changes, medication application, and wound monitoring. 4 Studies suggest that shared wound management can enhance patient engagement, personalize treatment plans, and ultimately contribute to a better overall quality of life, particularly for individuals with chronic wounds.2,3
While self-management of chronic illnesses has become more accepted in recent years, some patients remain hesitant to take on wound care due to its complexities. Wound care requires not just lifestyle modifications, but also the task of cleaning the wound itself.
This study aims to identify the barriers that prevent patients from taking a more active role in their wound care management. By understanding these challenges, we can develop targeted strategies to promote the self-wound care concept to relieve the healthcare burden imposed by wound care in Singapore's aging population.
Methodology
This study was approved by National Healthcare Group, Domain Specific Review Board (DSRB), Singapore (DSRB reference no: 2019/01162). We conducted a study in Singapore between 2020 and 2022, recruiting participants from 6 polyclinics using a convenience sampling method. Patients who visited these polyclinics for wound care appointments during the study timeframe were potential participants. The study excluded individuals with cognitive, hearing, or visual impairments, as well as those who were bedridden or resided in nursing homes. Visual assessments were conducted to identify signs of cognitive and physical impairments and individuals suggestive of these impairments were excluded from the study. Most of the participants indicated that they comprehended the survey questions well. Only a small number required additional clarification, which was promptly provided by our research assistant.
The study utilized a validated self-wound care acceptance survey developed by Goh et al in 2022. 5 This survey demonstrated strong internal consistency, reliability coefficient of 0.81, and moderate validity, CVI of 0.72. Participants answered a questionnaire with various sections. The first section addressed demographics and socioeconomic status (11 questions), while the second section focused on their wounds (4 questions). To gauge patients’ reservations or hesitations toward self-wound care, the researchers employed 8 questions from Section C. These questions centered on negative thoughts, family involvement, and logistical difficulties associated with self-wound care. Participants responded using a 5-point Likert scale ranging from strongly disagree to strongly agree. A higher score on the scale indicated a reduced hesitation toward the concept of self-wound care.
The collected data were analyzed using SPSS 28. Descriptive statistics were used for data description. As the data followed a normal distribution, parametric tests including t-test and one-way ANOVA were employed to identify any differences between groups.
Results
Among the 328 participants who took part in the study, it was found that 66% were male, while the remaining 34% were female. In terms of ethnicity, 65% of the participants identified as Chinese, 16% as Indian, and 13% as Malay. The remaining participants belonged to various other racial backgrounds. A significant majority, 63% of the participants were aged 51 and above. Most of the participants were employed, took personal responsibility for their medical expenses, had a secondary level of education, relied on public transportation to access the clinic, and lived in public housing. Eighty-eight percent of the participants were able to independently carry out their daily activities without any assistance. A significant 85% of the participants enjoyed strong support from their families, while 73% benefited from a good social support system. It was reported that 73% of the participants had wounds on their upper and lower limbs. The majority of these wounds, 67% were surgical wounds without limb loss, abrasions, and lacerations, while the remaining 33% consisted of diabetic foot ulcers, arterial/venous/chronic ulcers, pressure injuries, skin tears, and amputations (refer to Table 1).Overall, 45% expressed disagreement on performing self-wound care themselves
Demographics and Wound-Related Variables and the Scores on Questions on Self-Wound Care Hesitancy (n = 328).

* Q1 to Q8 are the eight questions in the self-wound care survey.
* Minimum score 1; maximum score 5.
* The higher the score, the less hesitation toward self-wound care.
* P-value <.05 denotes significance.
Using one-way ANOVA test.
Using independent t-test.
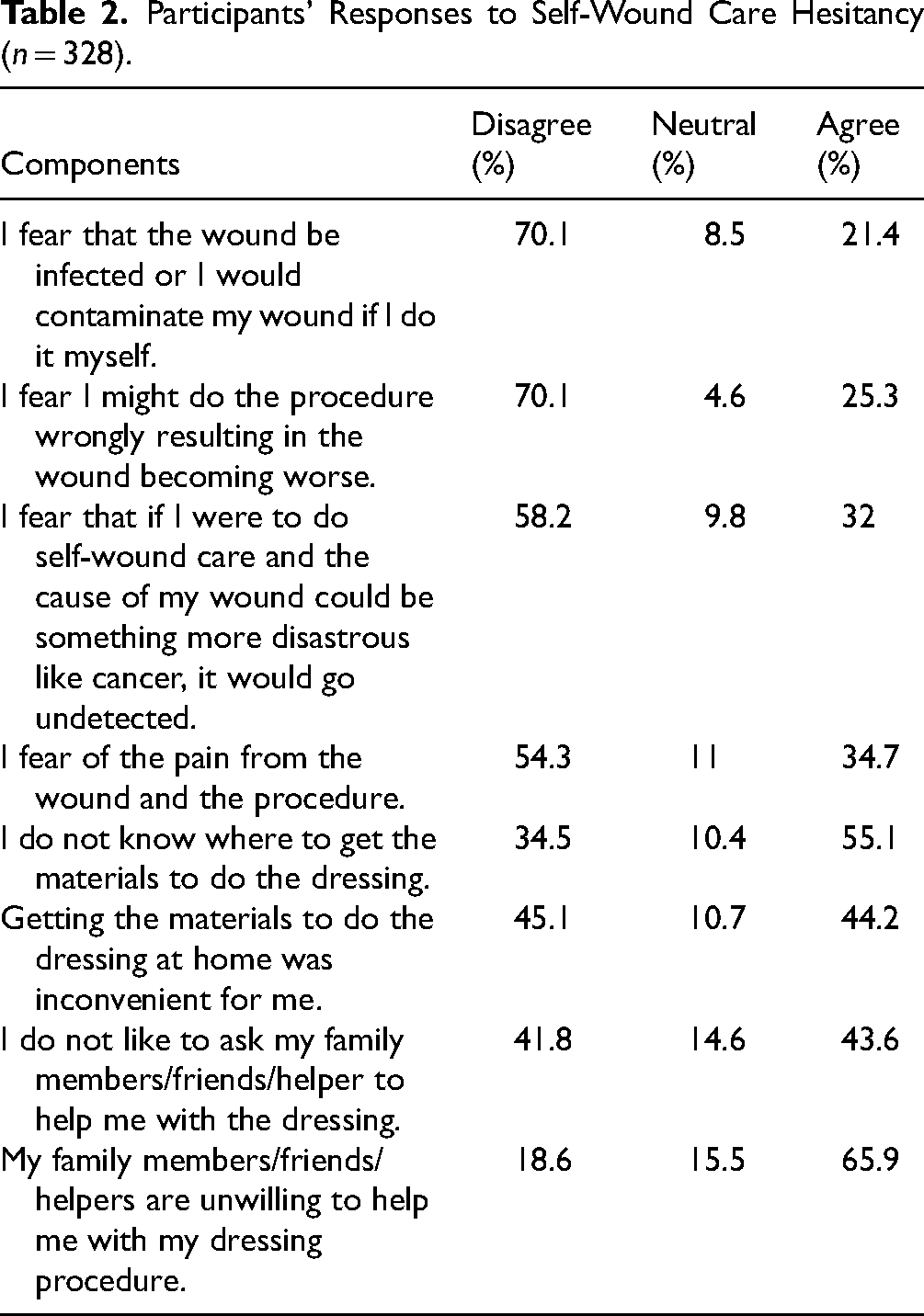
Sixty-six percent of the participants expressed that their family members, friends, or helpers exhibited an unwillingness to assist them with the process of dressing, especially individuals whose medical expenses were covered by Medisave and those who were beneficiaries of social assistance. They displayed a greater inclination toward the belief that their family members and friends would be disinclined to assist them in the dressing procedure, F(6321) = 2.815, P = .011, than those whose medical expenses were covered by other means. Conversely, females significantly agreed that their family members, friends, or helpers would be willing to help in the self-wound care process than males, t(326) = 2.102, P = .036. It was observed that the younger age group generally had family members who were open to helping them with self-wound care than the older age groups, F(2325) = 6.128, P = .002. Both students and males serving national service significantly agreed that their family members and friends were more willing to assist with dressing when requested than other occupational groups, F(4323) = 3.482, P = .008. Furthermore, individuals with good family support agreed that their family members would be willing to aid in the dressing procedure than those with poor family support, t(325) = −3.687, P < .001). Among the participants, 55.1% acknowledged their unfamiliarity with the means to acquire the necessary materials for dressing. Furthermore, 44.2% of the participants concurred that the procurement of dressing materials for home use posed an inconvenience.
Forty-four percent of participants were hesitant to ask family, friends, or helpers for dressing procedure assistance. This trend was interestingly reversed among those with good family support, who indicated a greater willingness to seek help from family members for dressing procedure, t(325) = −2.338, P = .020. Older participants were more likely to dislike the idea of asking family members for dressing procedure assistance, F(2325) = 3.697, P = .026. Participants with a secondary education background showed a higher tendency to avoid asking family or friends for help as well, likely due to concerns about inconveniencing them, F(4323) = 4.287, P = .002.
Pain during the procedure was a concern for 34.7% of participants, while 32% expressed apprehension that self-wound care at home might lead to missed diagnoses of serious underlying conditions, like cancer. This fear was significantly lower for those independent in daily activities compared to those who were dependent, t(57.503) = −3.280, P = .002. Younger participants, F(2325) = 4.811, P = .009, also exhibited less fear of missing a serious condition when performing self-wound care. Ethnicity and education level further influenced these anxieties. Malays reported a greater fear of missing a serious condition with self-wound care than other ethnic groups, F(3324) = 3.383, P = .018, while participants with a university education had significantly less fear compared to those with lower education levels, F(4323) = 7.845, P < .001. Interestingly, financial responsibility for medical bills also appeared to be a factor. Those who had their medical bills paid for by family reported a higher fear of missing a serious condition with self-wound care, F(6321) = 2.216, P = .041.
Twenty-five percent of participants expressed fear of improper technique worsening the wound. Additionally, wound infection or contamination was a concern for 21.4% of participants when performing self-wound care. Interestingly, gender and family support played a role in these anxieties. Males were significantly less likely to report concerns about infection or contamination during self-wound care, t(326) = −2.190, P = .029. Notably, those who lacked family support also had less fear of wound infection or contamination when performing self-wound care, t(325) = 2.439, P = .015, suggesting they may be more accustomed to practicing self-care and hygiene due to their situation (refer to Table 2).
Participants’ Responses to Self-Wound Care Hesitancy (n = 328).
Discussion
This study explored the reasons why some patients might be hesitant to perform self-wound care. The findings reveal a complex interplay between factors such as family support, patient demographics, and individual anxieties that can influence this hesitation. The research highlights the importance of family support, educational interventions, and financial considerations in promoting successful self-care practices.
Males exhibit greater boldness in executing medical procedures compared to females. In society, there is a greater inclination to support the female gender, thus leading to the perception that family members are more inclined to assist in the process of dressing wounds. Individuals who are dependent on activities of daily living, and potentially facing health issues, are more cautious and attentive to their well-being. Consequently, they may hesitate to engage in dressing their own wounds due to concerns that the underlying cause may be severe and go undetected. Conversely, individuals in younger age groups possess a heightened awareness and promptly raise concerns if they notice any abnormalities, resulting in a willingness to perform the procedure without fear of overlooking any potential issues. In other words, their heightened awareness enables them to discern when to seek assistance if they identify any irregularities with the wound. This finding aligns with Brown et al 2 who suggest that elderly or disabled patients might struggle with wound care tasks due to lack of access to information resources. 2 This emphasizes the need for tailored educational interventions to empower such individuals for self-care. Those with higher levels of education tend to possess a greater sense of when to seek help. Some participants fear exacerbating the wound through improper techniques thus this underscores the necessity for clear and concise wound care instructions.
Individuals without familial support tend to exhibit greater independence, as they are less concerned about the risk of infection or contamination of their wounds. They displayed increased self-assurance and reduced dependence on family members for assistance, suggesting a heightened level of proficiency in self-care practices. Conversely, individuals who possess strong familial support perceive their family members as being willing to aid them in the dressing procedure and are inclined to solicit their assistance. Thus, the significance of fostering robust familial relationships becomes apparent. Students and national servicemen, who are predominantly younger individuals, reported that family members are willing to assist them in the dressing procedure. These family members are likely parents, who are more inclined to provide aid, as opposed to the reverse scenario of children assisting their parents. The older age group tends to avoid seeking assistance from others, possibly due to cultural pride within Asian families, wherein younger members are not typically sought out for help. This aligns with Brown et al's 2 suggestion that older patients, who may be more comfortable with traditional models where a healthcare professional performs wound dressing, might be less receptive to self-wound care if they perceive themselves as unable to manage the task effectively. 2 Lastly, individuals receiving social assistance often have limited familial and social networks, and may be estranged from their family members thus, they tend to perceive a diminished likelihood of receiving assistance from their relatives.
Limitations
Although there was no participant attrition, the use of convenience sampling may limit the external validity of the results. The unique characteristics of primary healthcare centers, including their clinical practices, protocols, and patient demographics, may influence the observed findings. Therefore, results should be interpreted with caution when applying them to different healthcare settings or populations. Future studies should include self-efficacy, health literacy; and healthcare provider perspectives to provide a more comprehensive understanding of the barriers to self-wound care. This approach, combined with randomized sampling methods, would enhance the representativeness and depth of insights gained from the patient population. Furthermore, adopting a longitudinal design would allow researchers to track changes in patients’ attitudes, behaviors, and psychological factors related to self-wound care over time.
Conclusion
Strong family support emerged as a key factor thus interventions should focus on fostering open communication within families and reducing caregiver burden. Educational programs and workshops addressing proper technique, self-wound care practices, and complication signs are crucial to alleviate patient anxieties. Furthermore, exploring assistance for wound care supplies and broader medical cost reduction for self-wound care are necessary to overcome logistical barriers to increase the take-up rates for self-wound care.
Footnotes
Acknowledgments
We would also like to thank Chief Nurse Lim Voon Hooi, DPCND Chen Yee Chui, and all nurses in NHGP; and Dr Tang and her CRU team for their support in this study.
Author Contributor Statement
Ling Jia Goh and Xiaoli Zhu designed and implement the study. Ling Jia Goh analyzed and wrote the paper with expert advice contributed by Xiaoli Zhu. Ling Jia Goh and Xiaoli Zhu agreed to the contents of the study.
Declaration of Conflicting Interests
All author(s) declared no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Primary Health Care Research and Innovation, a partnership between LKC School of Medicine, NTU, and NHG Singapore for the research grant—Seedcorn Funding (Grant No. CPHCRI 5.2/006).
Ethical Statement
This study is approved by the National Healthcare Group, Domain Specific Review Board (DSRB). DSRB reference no: 2019/01162.