
Abstract
The Barwon Health Cachexia & Nutrition Support Service (CNSS) is an outpatient service focused on improving clinical outcomes and quality of life for patients with or at high risk of cancer cachexia. Patients see a multidisciplinary team, comprising a palliative medicine physician, physiotherapist, dietitian, and nurse practitioner. This study evaluated the service from patient and carer perspectives. In 2016/17, semistructured interviews were conducted with 12 patients and 9 carers attending the service, focusing on: (1) reflection on experience of the CNSS, and (2) describing how a cachexia-specific service can meet their needs and concerns. Analysis generated 4 superordinate themes: evolving perception of service value, empowerment through person-centered care, communication to patients and carers regarding health/disease information, and the importance of the multidisciplinary team-based approach. Generally, patients and carers reported overall positive experiences with the service, particularly with regard to improved communication and management of the patient. Findings confirmed the patient-centered and individualized approaches were particularly valued. These insights are a critical step in the development of recommendations for future clinical management of cancer cachexia.
Introduction
Cancer cachexia is a complex paraneoplastic syndrome characterized by anorexia, asthenia, progressive weight loss, and skeletal muscle loss in the setting of systemic inflammation (1,2). Cachexia affects approximately 50% of cancer patients, and up to 20% of all cancer deaths are caused directly by cachexia, through immobility, cardiac or respiratory failure (1,3). Overall prevalence of weight loss in cancer patients remains as high as 86% in the last 1 to 2 weeks of life (1).
There have been studies investigating patient and carer experiences of cachexia (4,5), but studies reporting experiences of related services are limited, despite increasing calls for patient voices to shape clinical care (6,7). The Barwon Health Cachexia and Nutrition Support Service (CNSS) was established in 2008 to provide supportive care for cancer patients with cachexia (8). This service was established by a palliative care physician with a special interest in cancer cachexia, hence was located within Community Palliative Care.
Improving quality of life and symptom management for patients with cachexia using multidisciplinary approaches has been recognized as beneficial (9,10); however, there is little advice on how to put this approach into practice. The rationale for the CNSS structure has been discussed previously (8). Briefly, patients referred to CNSS meet a multidisciplinary team to maximize nutritional support, functional muscle strength, and manage cachexia-related symptoms. The initial structure involved patients seeing a palliative medicine physician, physiotherapist, and dietitian consecutively in a 3-hour appointment (8). Significantly, the CNSS includes an emphasis on psychosocial issues arising from cachexia. The CNSS aims to improve patient and carers’ knowledge about the impact of cachexia on social engagement, energy levels, appetite, and nutritional requirements (8), given common themes of family concern leading to tensions, especially relating to dietary intake (4,11). In 2012, a nurse practitioner was introduced to coordinate, streamline, and promote the service. In early-2015, the service transitioned to a “streamlined” format, with patients reviewed by all clinicians simultaneously. Appointments consisted of 80 minutes for new patients and 40 minutes for reviews. This transition was initiated following feedback from patients and carers that 3-hour sequential appointments were too burdensome.
The CNSS uses patient-reported outcome measures with the “European Organisation for Research and treatment of Cancer” and “Functional Assessment Anorexia/Cachexia Treatment” tools, which trigger important care conversations, however does not routinely survey clinical experience (9,10,12).
The CNSS is an evolving service, striving to improve outcomes and quality of life of patients and their families. A rigorous evaluation of patient experience had not previously been undertaken and is essential to inform future service delivery.
Methods
A qualitative interview-based study, approved by the Barwon Health Human Research Ethics Committee, was undertaken with attending patients and carers to evaluate the multidisciplinary service approach. Inclusion/exclusion criteria are outlined in Table 1. All eligible patients, carers or family attending CNSS during the study period were invited to participate. Written consent was obtained from participants before the interviews, which were conducted one-on-one with a single interviewer independent of the service (J.G.). To maximize consistency between interactions, a semistructured interview guide, using open-ended questions developed in-line with clinical experiences, was used by the interviewer (see Table 2), and focused on 2 broad themes:
1. Reflection on experience of the CNSS, and 2. Description of ideal experience or expectation of a cachexia-specific support service.
Inclusion/Exclusion Criteria.
Abbreviation: CNSS, Cachexia & Nutrition Support Service.
Semistructured Interview.

Abbreviation: CNSS, Cachexia & Nutrition Support Service.
All interviews were conducted in-person, audio-taped, transcribed verbatim, and deidentified before analysis. Interview transcripts were reviewed to determine whether interviewer drift had occurred.
All transcripts underwent conventional content analysis by 3 investigators (V.C.V., M.H., A.D.; coded in NVivo v12, QSR International), to develop a representative thematic framework (13,14). Categories were developed inductively rather than preconceived. In-depth discussion of emerging themes took place before a final iteration of results was developed. Interrater reliabilities were not calculated (15), as the primary aim was discovery of themes, rather than agreement. Discrepancies in reviewer coding were discussed to consensus.
Saturation was an ongoing, cumulative judgment, determined during the concurrent analysis of transcripts. There is always potential for new themes to emerge; therefore, the study may not fully encapsulate theoretical completeness, and nuance may be lacking.
The number of participants commenting on particular themes was not deemed representative of the views of the whole sample. Nevertheless, when an issue was raised frequently, weight was attributed to this as reflecting an important element of experience.
Results
Twelve patients and 9 carers were interviewed before reaching data saturation. Participant characteristics are included in Table 3. The sample included 6 male and 6 female patients aged 56 to 86 (median: 72 years). The carers included 3 males and 6 females (6 spouses, 2 daughters, and 1 friend). One patient and 2 carers withdrew consent before interview. A further patient consented but was unable to be contacted for interview. All participants attended at least one consultation, with appointments ranging from 1 to 6 consultations (median: 3.5 consults).
Characteristics of Study Participants.

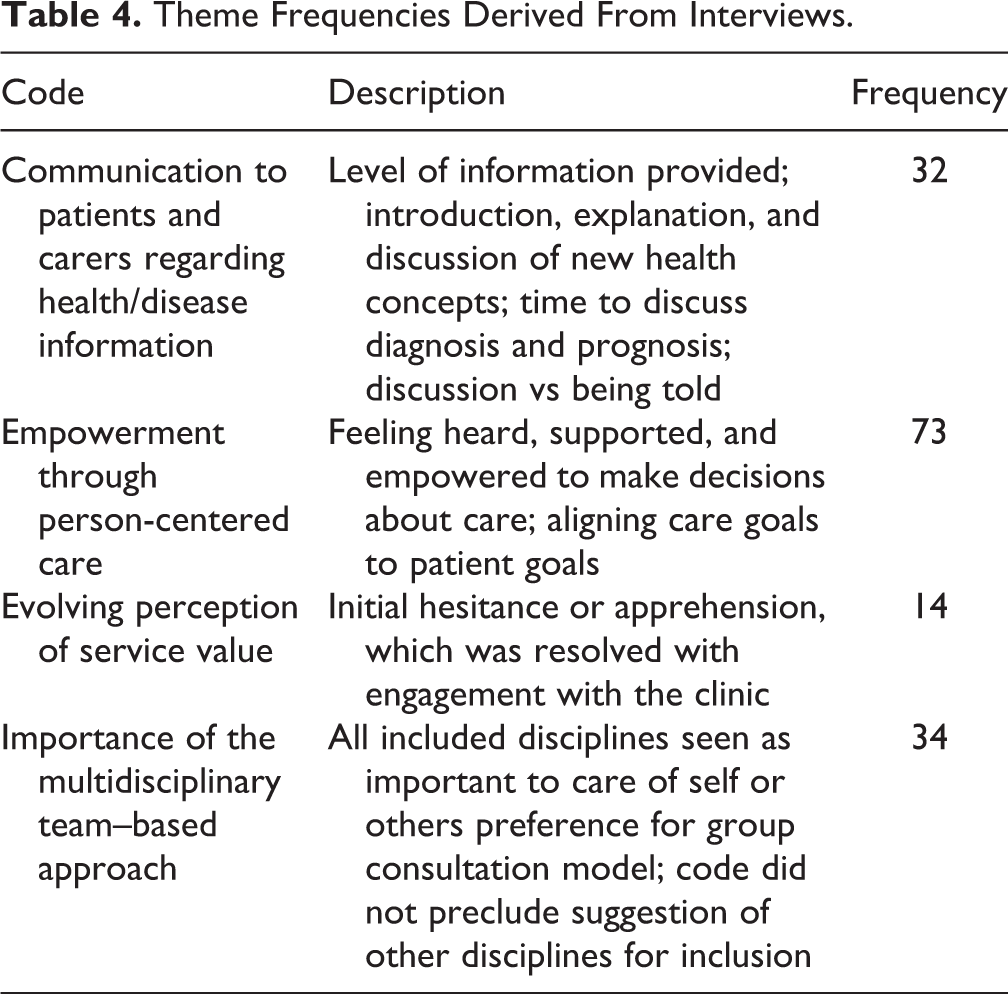
During analysis, 4 overarching themes emerged (see Table 4): evolution of perception of value of the service, empowerment through person-centered care, communication regarding health/disease information, and the importance of the multidisciplinary team approach. Overall perceptions of the service and areas for improvement were also identified.
Theme Frequencies Derived From Interviews.
Overall Perceptions of the Service
Generally, participants reported overall positive experiences with the service, particularly regarding communication with and empowerment of the patient. Several people commented that the name was confusing or confronting, with “support” implying group discussions with other patients, causing initial feelings of trepidation. Colocation with palliative care was also a source of concern, with “palliative care” associated with end of life rather than supportive care. “I got a message to say that we should go to the palliative care and I just felt I’m not ready for that yet, and I was going to say no, I’m not ready I might come later on.” (Carer 7) “I expected that I was going to walk in with say twenty other people or something and in a big room and anyway it was nothing like that, it was just four people and me.” (Patient 13)
Patients expressed that they would recommend the service to others going through a similar experience, referencing feelings of hope, confidence, and empowerment.
“I think it gives you strength and confidence and you realise that it’s not just, well it is a dead-end road, but there’s hope of improving your quality-of-life.” (Patient 11)
“Well, I think the biggest thing that I have noticed was the amount of support that [patient’s] getting and the way that she has responded to the support and to the care that they are showing. To be faced in at the stage of our life with a horrific thing like [patient] was faced with and the lack of hope that was given by the doctors, to be taken into a room with professionals that have one goal in mind and that is to improve her standard of life and to care for her more than what she is capable for caring for herself or on the other hand what I can provide, the amount of encouragement that she has received is unbelievable. I’ve got nothing but accolades.” (Carer 12)
“They saved my life, simple” (Patient 6)
Evolution of Perception of Value of the Service
Before initial attendance, many participants were apprehensive about the goals or benefits of the service. However, most reported finding the service helpful. Some patients and carers identified that the number of clinicians could be daunting initially, having anticipated seeing one clinician, or progressing through a series of appointments. However, most also reflected that the model had benefit, with appointments being quicker, and everyone being “on the same page” about issues and management without the requirement to repeat things multiple times.
“I found it rather daunting [at first] because you walk in and are expecting just one person there and we had five […] but once you get in there you get past it and its fine.” (Patient 1)
“With the four of them in there together, everyone that’s concerned with you knows the others, where you are at with the other person as well.” (Carer 7)
A few patients mentioned that they were upset at their first appointment, realizing how their condition had deteriorated and concerned that the program may be too much to endure. However, these patients also described improvement in their health from attending the service, which led to an increased perception of value of the CNSS to their quality of life and feeling of well-being. “I thought “Oh I don’t know about this” the first time in there. Then when the physio gave me exercises and I found I had no strength, that was a bit hard to take […] The next time I went it was easier. I want to get better and get stronger” (Patient 2)
Empowerment Through Person-Centred Care
All participants expressed feeling supported by the clinicians. Patients felt supported and motivated to make choices about their care, including determining levels of intervention appropriate to their goals. This approach to shared decision-making and negotiation of treatment plans between patients and clinicians may play a key role in facilitating adherence to their individualized program and would benefit from further exploration.
“The biggest thing I think I like with the clinic is they listen. […] they ask you questions, they listen to what you say and then they work around that. And that from the very first time that I went I thought these people care about me.” (Patient 6)
“I was going 4-weekly […] now they have cut me down to the 8-weekly, but it was my wish […] I have come a long way since I first started there and keeping up the exercises and that has helped me a lot I think.” (Patient 2)
The explicit invitation to bring an advocate or support person to consultations was highly valued, with the shared experience helping to reduce feelings of helplessness that carers often identified. As well a family member lending support to the patient, it provided an opportunity to reframe conversations around eating, fatigue, and social conflict/withdrawal, which are common themes that emerge during the progression of cachexia (16).
“[The physician] spent time talking with [Carer]. Because invariably in these things people always feel sorry for the people who have got it. But they overlook the demands and the toll its taking on the partner. [The physician] addressed that and spoke to [Carer] in a on-on-one.” (Patient 11)
“I feel it was important for me to go to each appointment with [patient]. That was our thing. We were doing this together.” (Carer 11)
“Everyone [in family] wants to get involved, wants to know they’re doing the right thing. You know, not telling one thing and doing another.” (Patient 9)
Communication Regarding Health Literacy/Education
The CNSS was developed with a focus on enabling patients to be active participants in their own care, providing appropriate information to ensure patients can make informed decisions about their management. The majority of participants were satisfied with the information supplied during consultations and were comfortable asking for additional explanations.
Common areas of improved health literacy included nutritional awareness and enhanced recognition of the importance of physical activity. Most participants were not familiar with the term cachexia before attending the service but had identified problems with eating, weight loss, and fatigue.
“[Carer] asked most of the questions, I didn’t want to ask, I didn’t understand. And then it was still all explained to us, writing down the medical terms, what it meant. Couldn’t ask for anything more.” (Patient 9)
“They told me to eat just about anything to try and get some weight on because I was eating properly but nothing that would put any weight on […] Since then they gave me exercises and each time I have gone back everything has been a bit better.” (Patient 6)
Some participants did not feel that their concerns about lack of appetite and loss of weight had been fully addressed by oncology or general practice.
“We had no idea what [cachexia] was before we came…[She] was losing such a lot of weight and there had been nothing” (Carer 3)
“They sort of explained a hell of a lot more, […] not about what he’s got but the effects and everything that can happen from it […] not where it is but what will happen” (Carer 10)
Patients recognized that the oncology team focus was on treating cancer and the CNSS focused more on symptom management and quality of life.
“I was sort of whinging a bit and saying you’re giving me chemotherapy and doing everything else but I am starting to disappear […] eventually between my GP and the oncologist they got me onto this program and I have been really happy with it” (Patient 1)
Importance of the Multidisciplinary Team–Based Approach
Most participants identified benefit from each discipline and that all played an important role in perceived improved outcomes.
“That is probably the most efficient way of dealing with the issues that need to be dealt with […] when there are so many different aspects of the care being given to be able to do it in one swoop” (Carer 12)
“I can’t see any way they could improve on the way they’re going about it now because they are covering the physical, the nutritional, the medical sort of aspects already” (Patient 7)
Patient 1 commented that “everyone has the same goal” and when asked how the service could be improved stated, “if it ain’t broke don’t fix it.” One carer did not agree with nutritional advice and lack of alternative medicine, and one carer believed their spouse was too weak to benefit from the physiotherapist’s physical activity intervention but acknowledged the importance of their role in the team. These were the only instances patient and carer perspectives appeared to differ. Comparisons by gender or cancer type/stage were unable to be completed due to the small number of participants, however would be a valuable addition to future studies.
Discussion
The patient experience is an essential but often underreported consideration in ongoing development of supportive care service models. The current study provided our patients and families a voice in the ongoing conversation around appropriate approaches to multidisciplinary cachexia care.
Participants reported that the streamlined approach brought together the multidisciplinary management of cachexia, and they appreciated input from individual clinicians and the impact each had on improving their understanding of cachexia and its management. The disadvantage of the streamlined approach was that patients were initially overwhelmed by the number of people in the room. However, this evolved into a recognition of the value of having 4 health professionals involved in their care simultaneously, negating the need to repeat themselves regarding their illness and symptoms.
This improved communication around cachexia issues was one of the key benefits reported during this study. While patients reported cachexia was often not addressed by their oncologist or general practitioner, referrals to the CNSS from these clinicians indicate a level of collaboration with the CNSS. Other clinicians may have less time or resources available for a multidisciplinary assessment and integrated plan to focus on these cachexia-specific issues (rather than disease modification). This highlights a potential gap in cancer supportive care that can be addressed with services like the CNSS. It has been suggested that introducing supportive interventions, including information about cachexia for patients and carers, may provide peace of mind, reduce cachexia-related distress, and assist with coping with cachexia (17). This study supports the assertion that the CNSS is addressing 3 of the critical issues that patients and carers have previously identified as desiring from health professionals: acknowledgment of weight loss concerns, information about what is happening and why, and interventions to address these concerns (17).
Room for Improvement
Although some patients were very happy with the experience and did not identify a need for changes, other patients and carers provided considered suggestions, some of which were able to be readily implemented. For example, several patients noted better briefing on the service’s purpose and format before the initial appointment would reduce hesitancy and confusion. The nurse practitioner now ensures this occurs when scheduling the initial appointment. The feasibility of some suggestions was limited by the availability of resources but should be considered for future development, including patient support groups, space to complete exercise prescription while waiting for appointments, and larger consulting rooms to accommodate the service.
Limitations
The current study was developed as a formative tool to shape the future of the clinic in response to user feedback, rather than a summative evaluation of the service. While the participants involved provided a representative subsection of the patients typically seen by the clinic, the generalizability is limited due to the small sample size, and as such comparisons are unable to be made to the broader population. The heterogeneity of participants also limits conclusions that may be drawn, with the study insufficiently powered to detect gender differences in responses, which is also true of cancer types or staging. A follow-up powered to detect disparate perspectives would provide useful information to tailor the care model.
Future Directions
The CNSS is continually evolving, and future research will include extending on this informative evaluation from patients and carers perspective with more emphasis on objective patient outcome and experience measures in improving overall quality of life (18). Expanding this evaluation would also include perspectives of stakeholders who refer patients to this service. The CNSS is more than a multidisciplinary clinic, and reviewing and justifying components of the service from economic perspectives will be prudent. Further analysis is currently underway on the efficiency of the model, and early results indicate that a more concise model may be justified.
Conclusion
The current study confirmed that participation in a cachexia-specific service was viewed as having a positive impact on quality of life and well-being by patients and carers. A person-centered and individualized approach by the multidisciplinary team, in particular, was of importance to those interviewed. It’s essential that people are not overwhelmed by the number of clinicians present or the amount of information presented. This approach may benefit patients due to reduced time burden, opportunities for discussion, and having the team “on the same page.” These insights are a critical step in development of recommendations for future clinical management of cachexia.
Footnotes
Authors’ Note
Removed from Methods section- Approved by the Barwon Health Human Research Ethics Committee (Reference BH-15.202) and the word Barwon Health from manuscript.
Acknowledgments
The team would like to thank the patients and families for sharing their experiences, Barwon Health volunteers who assisted with the project, and James Goonan, who conducted the interviews. The team would also like to thank Prof Trisha Dunning for sharing her qualitative study expertise while developing the protocol.
Declaration on Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: There may be a conflict of interest from Peter Martin and Meg Harrison, who are both clinicians in the Cachexia & Nutrition Support Service. Removed from Methods section- Approved by the Barwon Health Human Research Ethics Committee (Reference BH-15.202) and the word Barwon Health from manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.