
Abstract
Pulmonary hypertension is commonly seen with multiple complex disorders managed in the intensive care unit. Common causes of pulmonary hypertension in critically ill patients include severe hypoxia, sepsis, left ventricular failure, massive pulmonary emboli, drugs, and worsening of chronic pulmonary hypertension, among others. Reversible pulmonary hypertension is rare and it has been reported with mediastinal involvement of sarcoidosis and in critically ill patients with severe acute chest syndrome. We present a 43-year-old male who was admitted with acute-onset shortness of breath. A massive right-sided pleural effusion and left-sided pneumonia was found on chest roentgenogram. Echocardiogram showed severe pulmonary hypertension with normal left ventricular function. Patient was treated for presumptive pneumonia and underwent pleural fluid drainage. An echocardiogram repeated after removal of pleural fluid showed resolution of pulmonary hypertension. We hypothesize that the large pleural effusion produced mechanical compression of mediastinal and pulmonary vessels leading to severe pulmonary hypertension, which reversed upon drainage of pleural effusion. This has both diagnostic and management implications.
Keywords
Case Report
A 43-year-old Hispanic male was admitted to the intensive care unit (ICU) with worsening shortness of breath and decreased exercise tolerance of 2-day duration. He denied cough, fever, or constitutional symptoms. His medical history was remarkable for alcohol-induced liver cirrhosis and hypertension on no medications. Social history was significant only for chronic alcohol use. On examination, the patient was afebrile, tachypneic (respiratory rate of 24/minutes), and hypoxic (oxygen saturation of 80% on ambient air, which improved to 95% with supplemental oxygen). There were decreased breath sounds in the right hemithorax. Cardiovascular and neurological examinations were normal. There was mild ascites on abdominal examination and no extremity edema.
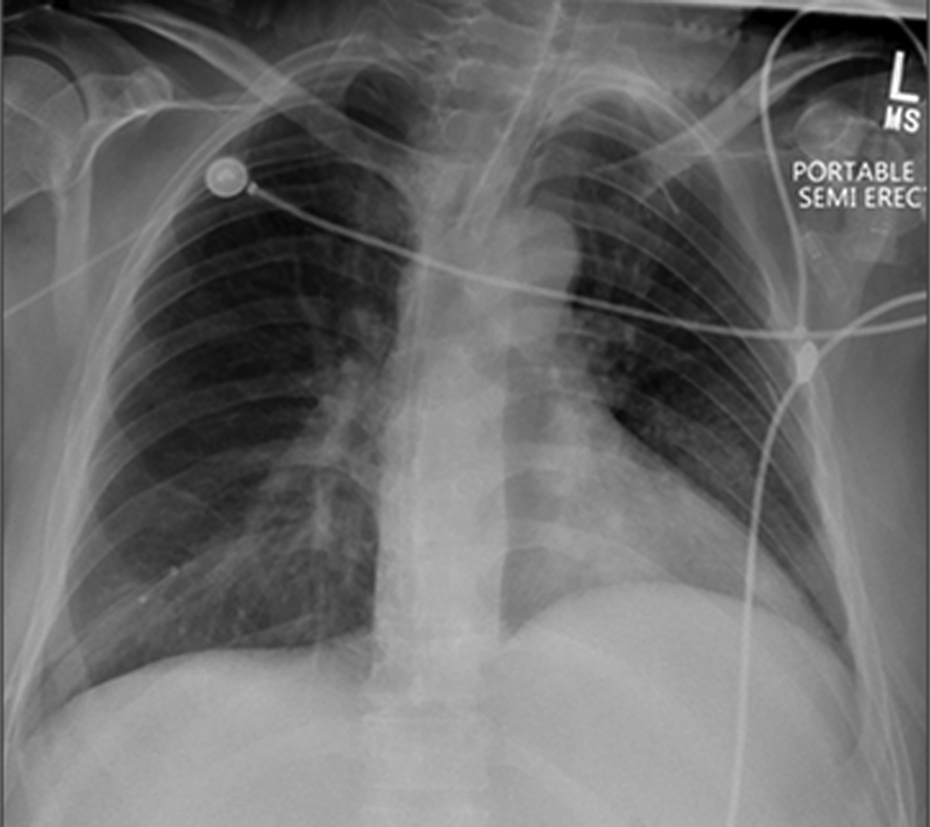
Pertinent laboratory parameters can be seen in Table 1. Chest roentgenogram (CXR) showed complete opacification of the right hemithorax and infiltrates in the left upper lobe (Figure 1). Patient was started on intravenous piperacillin–tazobactam, vancomycin, and doxycycline for pneumonia. In addition, thiamine, folic acid, and multivitamins were added. Thoracentesis of right-sided pleural effusion with pig tail insertion was performed; pleural fluid was consistent with transudative effusion likely due to hepatic hydrothorax. Abdominal paracentesis showed ascitic fluid to be consistent with portal hypertension.
Pertinent Laboratory Parameters.

Abbreviations: proBNP, pro–B-type natriuretic peptide; WBC, white blood cell.

Chest Xray on admission showing massive right pleural effusion and left sided infiltrates.
Echocardiogram performed on hospital admission revealed normal ejection fraction, elevated right atrial pressure (15 mm Hg), and severe pulmonary hypertension (PH) with a right ventricular systolic pressure (RVSP) of 68.88 mm Hg (Figure 2A) and a tricuspid regurgitation (TR) jet velocity of 3.67 m/s. Patient had a pleural fluid drainage of 1 to 1.5 L/d. During admission, cultures obtained using fiberoptic bronchoscopy with bronchoalveolar lavage were negatives for bacterial, fungal, viral infections, and tuberculosis.
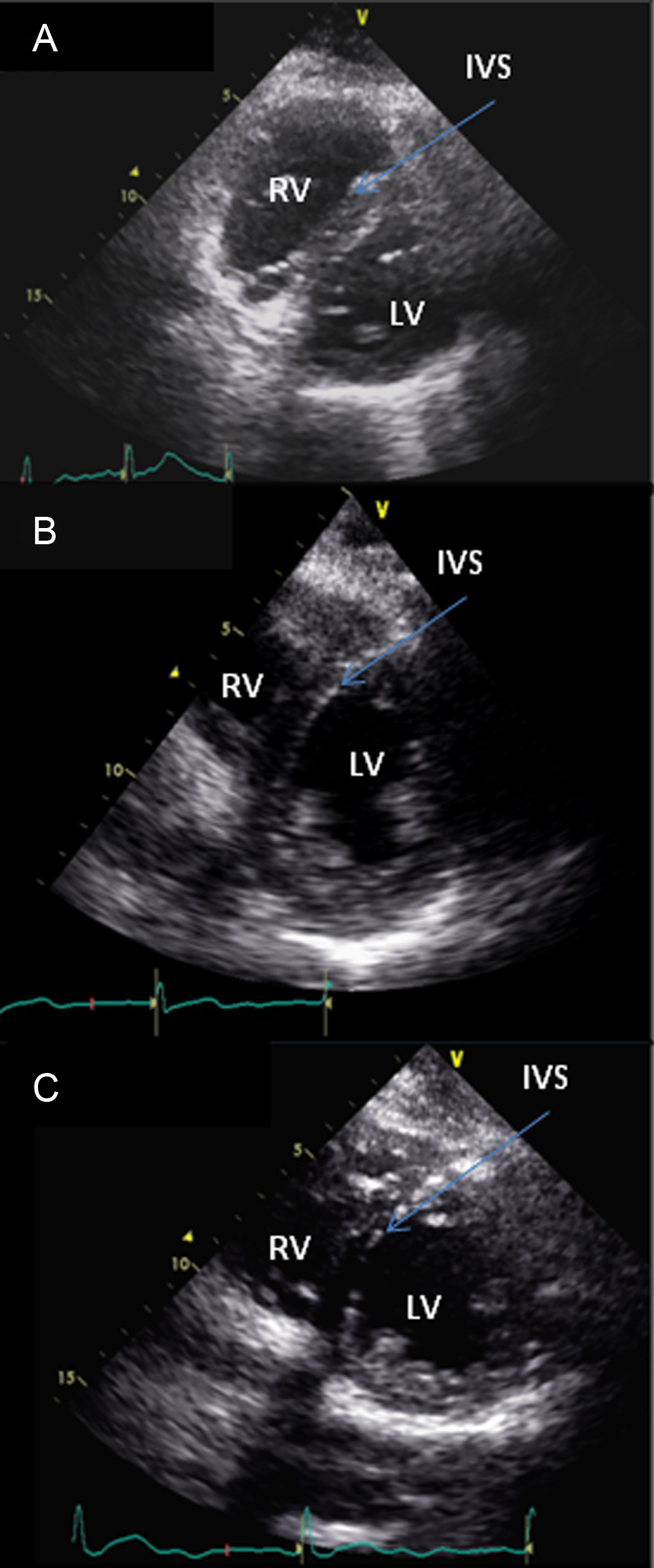
A, Transthoracic echocardiogram, parasternal short-axis view (at admission), showing left ventricle (LV), right ventricle (RV), and D-shaped deviation of interventricular septum (IVS) consistent with RV strain. B, Transthoracic echocardiogram, parasternal short-axis view (done 6 months prior to the admission), showing LV, RV, and IVS. C, Transthoracic echocardiogram, parasternal short-axis view (postdrainage of massive pleural effusion), showing LV, RV, and disappearance of previously seen D-shaped deviation of IVS.
Echocardiogram done 6 months prior to admission was normal with no evidence of elevated right-sided pressures (Figure 2B). Repeat echocardiogram after removal of around 8 L of pleural fluid showed resolution of PH with an RVSP of 29.89 mm Hg and a TR velocity of 2.23 m/s (Figure 2C). Repeated CXR showed complete resolution of the right-sided pleural effusion (Figure 3). Oxygen requirement during his ICU stay ranged from 0.35% to 0.45% to maintain a Pa
Chest Xray showing resolution of right pleural effusion and pigtail catheter.
His hospital course was complicated with acute respiratory failure requiring mechanical ventilation, acute renal failure, and septic shock due to Acinetobacter pneumonia. As per family wishes, palliative care was instituted and the patient died 37 days after admission.
Discussion
There are multiple causes of PH in critically ill patients. 1 The most common etiologies are left ventricular dysfunction or left ventricular failure due to congestive heart failure, myocardial infarct, severe valvular disease, or new-onset or worsening of previous PH. Acute respiratory distress syndrome, sepsis, drugs, and massive pulmonary emboli have also been implicated.
Hypoxia-producing hypoxic pulmonary vasoconstriction is a well-described phenomenon. Dorrington et al studied the patients exposed to hypoxia in a hyperbaric chamber while measuring their pulmonary vascular resistance (PVR) with a pulmonary vascular catheter. They found more than 2-fold increase in PVR within few hours of hypoxic exposure, which reversed on normoxia. 2 Our patient had transient hypoxia, which was rapidly corrected, so it will not explain the severe PH.
Sepsis causing PH in critically ill patients is not unusual. 3 Sibbald et al found increased pulmonary pressures in patients with sepsis compared with control, and the likelihood increased with prolonged and uncontrolled sepsis. Our patient developed sepsis with septic shock later during the hospital course, and at that time, his echocardiogram was normal.
Reversible PH has been reported secondary to acute chest syndrome, cocaine use, thiamine, and deficiency of vitamin C and iron. 4 -6 Mekontso Dessap et al reported PH in 60% of patients with acute chest syndrome, which resolved with resolution of the crisis. Reduced nitric oxide availability due to hemolysis has been postulated as mechanism of the sickle cell vasculopathy. 7
Pulmonary hypertension and right-sided heart failure secondary to thiamine deficiency, which resolved after therapeutic trial of thiamine for 2 weeks, have been reported. This was likely due to elevated left ventricular end-diastolic pressure. 4 Although thiamine deficiency might have been coexistent in our patient, he had no signs of left ventricular dysfunction, making thiamine deficiency unlikely. There are cases of vitamin C deficiency with iron deficiency associated with reversible PH. 5 The mechanism for PH in patients with deficiency of vitamin C and iron is pulmonary vasoconstriction due to uncontrolled hypoxia-inducible factor (HIF), which controls the body response to hypoxia; HIF activity depends on oxygen-dependent prolyl hydroxylases. Prolyl hydroxylase requires vitamin C and iron as cofactors. Our patient had normal iron levels, no evidence of cocaine use, and no indication of vitamin C deficiency.
Portopulmonary hypertension develops in patients with cirrhosis due to shear stress of pulmonary vasculature, leading to obstructive vasculopathy. 8 Pulmonary hypertension is found in 1% to 6% of patients with portal hypertension and is associated with high mortality. 9 Our patient had advanced liver cirrhosis, but he had a normal echocardiogram 6 months prior to admission and the PH resolved, making portopulmonary hypertension an unlikely etiology for the transient PH.
Extrinsic compression of pulmonary vessels leading to PH has been reported only in sarcoidosis. 10,11 These reports suggest that granulomatous inflammation of mediastinal lymph nodes and fibrosis causes extrinsic compression of major pulmonary artery causing PH.
Several studies have shown the impact of pleural effusion on the right side of the heart. Patients with large pleural effusion (right or left) can present with signs and symptoms of pericardial tamponade due to the transmission of the elevated pleural pressure to the heart. 12 Chidambaram et al reported echocardiogram evaluation of 40 patients with large pleural effusions before and after thoracentesis. Respiratory flow velocity variations typical of cardiac tamponade were detected in 85% of patients. Good mediastinal compliance or variations in volume of interventricular compartments were thought to be the mechanism to prevent development of tamponade physiology. 13 Animal studies showed that large bilateral pleural effusion in the presence of an otherwise insignificant pericardial effusion could result in right ventricular diastolic collapse and elevated pulmonary pressures. 14
In our patient, we hypothesize that the massive right-sided pleural effusion resulted in extrinsic mechanical compression of the lung parenchyma and major pulmonary artery leading to elevated pulmonary pressures.
Conclusion
Extrinsic compression from massive right-sided pleural effusion may lead to reversible PH. In patients with liver cirrhosis and large hepatic hydrothorax, the presence of PH can be erroneously attributed to portopulmonary hypertension, which carries a grim prognosis. We suggest to evaluate for reversible causes of PH and to repeat the echocardiogram after pleural fluid drainage. This approach could minimize extensive workup and avoid attributing the PH to liver disease. This has prognostic as well as management implications.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.