
Abstract
Objective:
To identify determinants of meconium aspiration syndrome among neonates admitted to the neonatal intensive care unit at Nigist Eleni Mohammed Memorial Comprehensive Specialized Hospital, South Ethiopia, in 2022.
Method:
A facility-based unmatched case–control study was used to identify meconium aspiration syndrome with a total sample size of 249 from January to April 2022. Data were entered by using EpiData version 3.1 and analyzed using SPSS version 24 software. Descriptive findings were presented by frequency tables and percentages. Multicollinearity was checked and the goodness of fit test was done. To determine the independent determinants associated with meconium aspiration syndrome, bivariate analysis was done and variables with a p value of <0.05 were taken to multivariate logistic regression analysis. Adjusted odds ratio with a 95% confidence interval was calculated, and statistical significance was declared at a p value less than 0.05.
Result:
Two hundred forty-nine (83 cases and 166 controls) mothers with their respective neonates were included in this study and that made the overall response rate 100%. Preeclampsia (adjusted odds ratio: 3.35, 95% confidence interval: 1.02, 10.97), antepartum hemorrhage (adjusted odds ratio: 3.63, 95% confidence interval: 1.50, 8.78), duration of labor (adjusted odds ratio: 4.34, 95% confidence interval: 1.83, 10.30), premature rupture of membrane (adjusted odds ratio: 16.02, 95% confidence interval: 5.66, 45.29), and obstructed labor (adjusted odds ratio: 4.57, 95% confidence interval: 1.42, 14.70) were determinants of meconium aspiration syndrome.
Conclusion:
In this study, preeclampsia, antepartum hemorrhage, duration of labor, premature rupture of membrane, and obstructed labor were determinants of meconium aspiration syndrome. Therefore, to reduce the risk of meconium aspiration syndrome, prevention, early identification, and management of these obstetrical factors may help to reduce meconium aspiration syndrome locally.
Introduction
Meconium is a germ-free, thick, black-green, odorless material that occurs around 12 weeks of gestation in the fetal intestine, and stores in the fetal colon throughout gestation. 1 The passage of meconium occurs within the first 24–48 h after birth. However, the fetus may pass meconium in the amniotic fluid during pregnancy. 2 Meconium aspiration syndrome (MAS), which occurs in about 2%–4% of all deliveries, is the respiratory distress of the newborn secondary to the presence of meconium in the tracheobronchial airways that can cause airway obstruction, atelectasis, and epithelial injury, surfactant inhibition, pneumothorax, pulmonary hypertension, and respiratory failure.3–7 In severe cases, MAS requires critical care in the neonatal intensive care unit (NICU) with respiratory, hemodynamic, and metabolic support. 8 However, the exact etiology of MAS remains unclear.9–11
Globally, MAS remains one of the commonest causes of perinatal asphyxia. 1 Ethiopia has one of the highest neonatal mortality rates worldwide, with nearly 80% of neonatal deaths occurring during the early neonatal period and MAS accounting for a substantial percentage.12,13
The reasons remain unclear and a review of risk factors may help reduce the future incidence of MAS. Therefore, this study aimed to identify the determinant factors of MAS among neonates admitted to the NICU at the Nigist Eleni Mohammed Memorial Comprehensive Specialized Hospital.
Methods and materials
Study area and period
This study was conducted in the Nigist Eleni Mohammed Memorial Comprehensive Specialized Hospital, which is found in Hosanna town of Hadiya zone. There are 31 beds, 10 incubators, and 8 radiators in the NICU and more than 1580 neonates receive care per year. This study was conducted from January to April 2022.
Study design
A facility-based unmatched case–control study design was employed.
Study population
All selected neonates admitted to the NICU at Nigist Eleni Mohammed Memorial Comprehensive Specialized Hospital during the data collection period.
Case definition: Infants admitted to the NICU with a diagnosis of MAS, which was based on clinical features (presence of meconium, tachypnea, respiratory grunting, nasal pillaring, and chest retractions) and radiographic signs on chest x-rays (patchy infiltrates, hyperexpansion).
Control definition: Neonates admitted to NICU in the hospital with a diagnosis other than MAS such as very low birth weight, low birth weight, preterm, sepsis, birth asphyxia, hypothermia, hypoglycemia.
Eligibility criteria
All selected neonates during the study period were included. However, neonates with major congenital malformation were excluded.
Sample size determination
The sample size was determined by using Epi Info version 7 (trademark of the Centers for Disease Control and Prevention in Atlanta, Georgia) by considering the assumptions of 95% confidence level, 80% power, ratio of control to case two to one (2:1), and adjusted odds ratio (AOR) from a previous study. 9 A nonresponse rate of 5% was considered (Table 1).
Sample size calculation for determinants of MAS among neonates admitted to neonatal intensive care unit at Nigist Eleni Mohammed Memorial Comprehensive Specialized Hospital, South Ethiopia, 2022.

AOR, adjusted odds ratio; MAS, meconium aspiration syndrome.
From the calculated sample sizes, 249 was the largest and it was the final sample size.
Sampling procedure
Systematic random sampling was applied to identify study participants admitted to the NICU. Based on the total number of infants (528) admitted within the 4-month duration of data collection and the calculated sample size (249), every second neonate was included in the study. The first neonate was selected by lottery method.
Study variable
Dependent variable: MAS.
Independent variables
The independent variables had three subcategories: sociodemographic variables (age, residence, educational status, religion, occupation, and marital status), obstetrics-related factors: (parity, gestational age, antenatal care follow-up, anemia, preeclampsia, antepartum hemorrhage, gestational diabetes mellitus, oligohydramnios, induction of labor, infection, mode of delivery, duration of labor, the premature rupture of membrane, and obstructed labor), and neonatal-related factors (sex of neonates, fetal presentation, birth weight, fetal distress, intrauterine meconium release, Apgar score at 1 and 5 min).
Operational definition
Apgar score assessment: It is carried out in the first minute and resuscitation measures are made (if necessary) to improve and again measured at 5 min. 14
NICU: It is a care unit for neonates in that care is given for neonatal complications.
Data collection instrument and procedure
The tool was developed and modified based on previously published studies.6,14–17 Data were collected using both interview and chart review by three Bachelor of Science degree nurses who were trained for this purpose. Neonates born at this hospital and those born elsewhere who were referred to this hospital were included in the study.
Data quality assurance
Data quality was assured by pretesting instruments on 5% of the total sample size and supervision of data collectors by two senior Bachelor of Science degree nurses. The training was given to data collectors and the investigators about the objective of the study and ways of data collection. The supervisors checked daily for completeness and consistency of the filled questionnaire. Data completeness and consistency were checked before data entry.
Statistical analysis
All data collected were checked and coded before it is fed to the computer database. Data were entered by using EpiData version 3.1 (software solutions development company, Buenos Aires, Distrito Federal, Argentina) and analyzed using SPSS version 24 software (a statistical software suite developed by IBM headquartered in Chicago and incorporated in Delaware). Descriptive findings were presented by frequency tables and percentages. Multicollinearity and goodness of fit test were done using the Hosmer–Lemeshow model goodness fit test. To determine the independent determinants associated with MAS, bivariate analysis was done and variables with a p value of <0.05 were taken to multivariate logistic regression analysis. AOR with 95% confidence interval (CI) was calculated and statistical significance was declared at a p value less or equal to 0.05.
Result
Sociodemographic characteristics of mothers
Two hundred forty-nine (83 cases and 166 controls) mothers with their respective neonates were included in this study and that made the overall response rate 100%. The overall sociodemographic characteristics of mothers are described below (Table 2).
Sociodemographic characteristics of mothers at Nigist Eleni Mohammed Memorial Comprehensive Specialized Hospital, South Ethiopia, 2022.

Obstetric factors
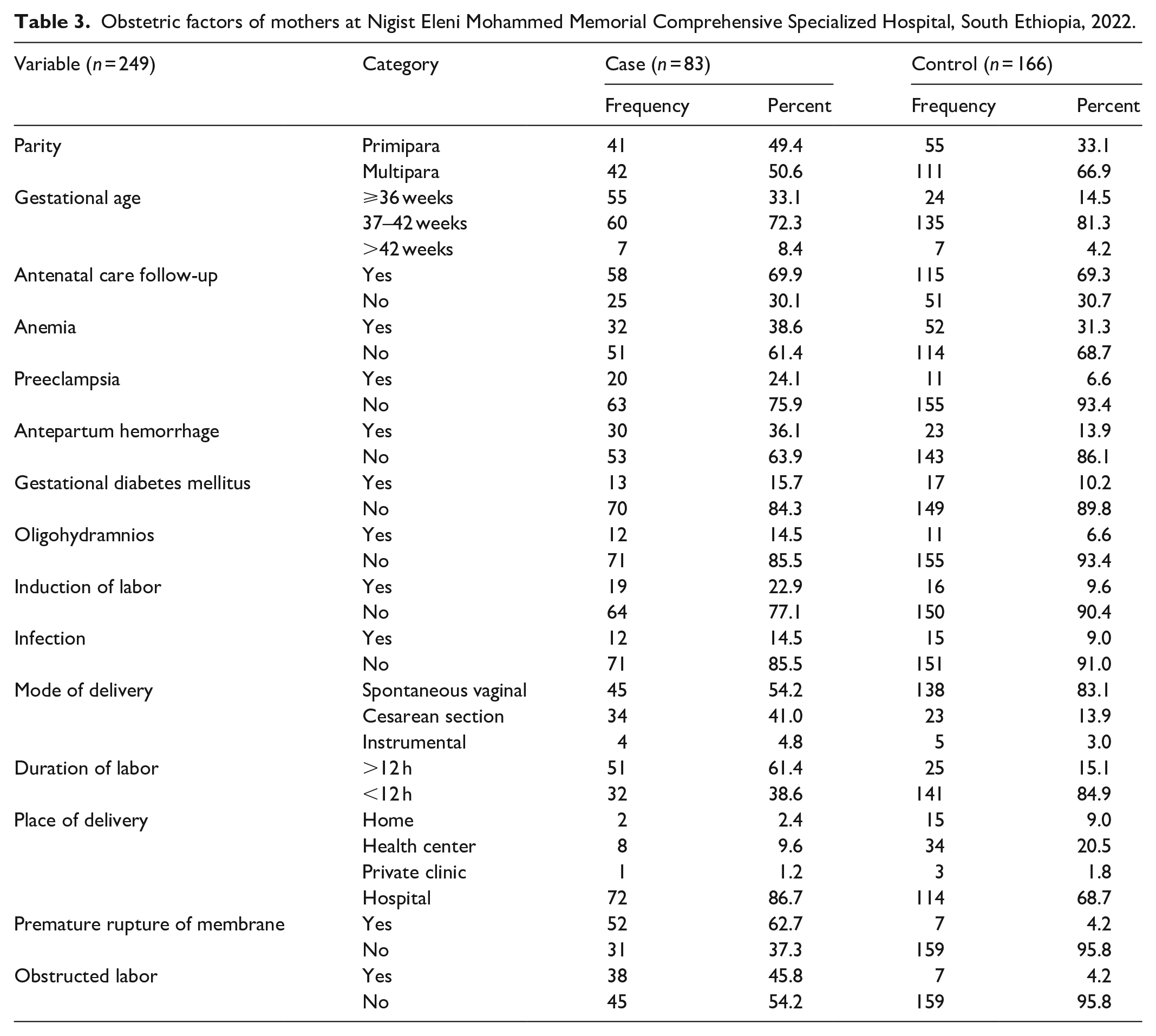
More than half, 42 (50.6%) of cases and 111 (66.9%) of controls were multiparas. Preeclampsia, antepartum hemorrhage, and oligohydramnios were more common in cases than in controls. Duration of labor for 51 (61.4%) cases was greater than or equal to 12 h; however, 141(84.9%) of controls was less than 12 h. The majority of mothers, 72 (86.7%) of cases, and 144 (68.7%) of controls gave birth in hospital. Premature rupture of membrane occurred for 52 (62.7%) of cases; however, it did occur only for 7 (4.2%) of controls. The labor was not obstructed for 45 (54.2%) of cases and 159 (95.8%) of controls (Table 3).
Obstetric factors of mothers at Nigist Eleni Mohammed Memorial Comprehensive Specialized Hospital, South Ethiopia, 2022.
Neonatal factors
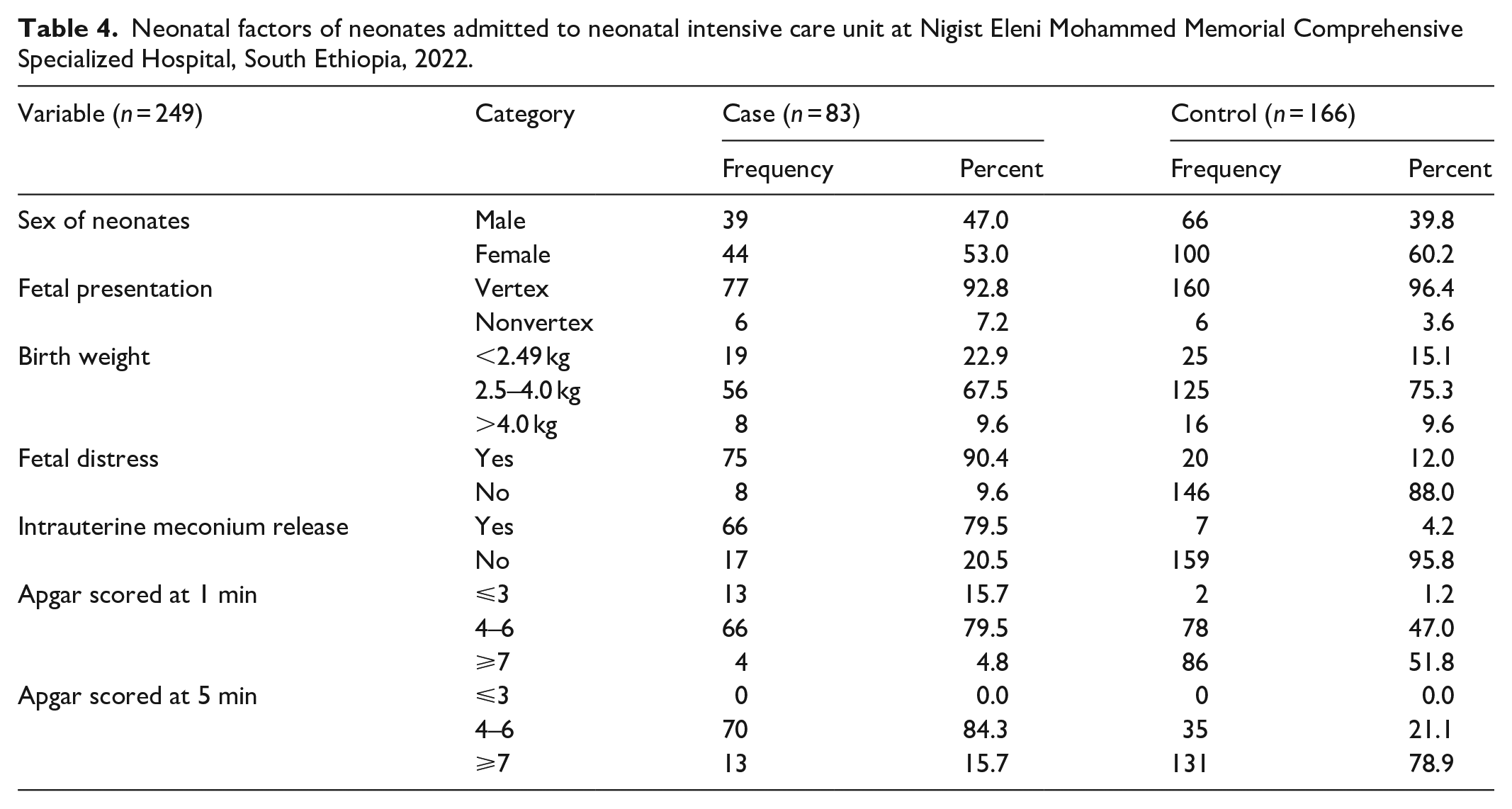
The overall description of neonatal factors is given in Table 4.
Neonatal factors of neonates admitted to neonatal intensive care unit at Nigist Eleni Mohammed Memorial Comprehensive Specialized Hospital, South Ethiopia, 2022.
Determinants associated with MAS
In bivariate logistic regression analysis, parity, preeclampsia, antepartum hemorrhage, oligohydramnios, duration of labor, place of delivery, premature rupture of membrane, and obstructed labor were associated with MAS. Whereas in multivariate logistic regression analysis, preeclampsia (AOR: 3.35, 95% CI: 1.02, 10.97), antepartum hemorrhage (AOR: 3.63, 95% CI: 1.50, 8.78), duration of labor (AOR: 4.34, 95% CI: 1.83, 10.30), premature rupture of membrane (AOR: 16.02, 95% CI: 5.66, 45.29), and obstructed labor (AOR: 4.57, 95% CI: 1.42, 14.70) were associated with MAS (Table 5).
Bivariable and multivariable logistic regression analysis of MAS among neonates admitted to neonatal care unit at Nigist Eleni Mohammed Memorial Comprehensive Specialized Hospital, South Ethiopia, 2022.

1, reference group; AOR, adjusted odds ratio; CI, confidence interval; COR, crude odds ratio; MAS, meconium aspiration syndrome.
p value < 0.05 in adjusted odds ratio.
Discussion
In this study, after controlling for confounding factors, preeclampsia, antepartum hemorrhage, duration of labor, premature rupture of membrane, and obstructed labor were found to be determinant risk factors of MAS.
This study indicated that preeclampsia plays a significant role in the occurrence of MAS among neonates. The odds of MAS increased about 3.35 times more comparing neonates whose mothers had preeclampsia during pregnancy to those neonates whose mothers did not have preeclampsia during pregnancy. This finding was supported by another study that indicated the odds of MAS increased about 1.7 times more likely among neonates whose mothers had pregnancy-induced hypertension compared to neonates whose mothers did not have pregnancy-induced hypertension. 18 Other studies also revealed that meconium aspiration was statistically associated with mothers who had a hypertensive disorder in pregnancy.10,11,19–21 On the other hand, the relationship between pregnancy hypertensive disorders and meconium aspiration had not been found in other studies.22,23 This might be due to the natural property of the diseases and the similarity in management protocol across various nations. It also might be due to differences in sample size and study design as others used retrospective cohort study design.
The odds of MAS increased about 3.63 times more comparing neonates whose mothers had antepartum hemorrhage during pregnancy to those mothers who did not have antepartum hemorrhage during pregnancy. This was supported by a study that stated antepartum hemorrhage is a risk factor for MAS. 20 In another study, respiratory tract infections and anemia during pregnancy were explained as risk factors for MAS10,24 but, not showed significance in this study.
The odds of MAS increased about 4.34 times more comparing neonates whose labor duration was greater than or equal to 12 h to those whose neonates duration of labor was less than 12 h. Another study indicated that the duration of the first and second labor stages had a statistical association with MAS. 10 The likely cause of meconium passage is the result of transient stimulation of parasympathetic nerves due to cord compression. 25 In another study, the passage of meconium in utero is considered a sign of fetal distress. 6 Prolonged labor is also stated as a risk factor for MAS.16,26–28 This is due to the risk that the fetus can have a high possibility to aspirate the amniotic fluid.
The odds of MAS increased about 16 times more comparing neonates whose mothers had premature rupture of the membrane to those mothers who did not have the premature rupture of membrane. Other studies indicated that premature rupture of the membrane to delivery interval had a statistical association with MAS.10,25,26 This might be due to the reason that a fetus can have a high possibility to swallow the amniotic fluid when the membrane is ruptured before labor.
The odds of MAS increased about 4.57 times more comparing neonates whose labor was obstructed to those whose labor did not obstruct. This was supported by another study that indicated labor dystocia was found to be a highly statistically significant factor of MAS. 29 This might be due to the reason that during obstructed labor, both rupture of membranes and intrauterine release of meconium can occur, which could lead to fetal inhalation of meconium.
However, this study did not identify some variables such as maternal age, parity, induction of labor, sex of neonate, and antenatal care9,10,12,30 that were significantly associated in other studies. This variation might be due to differences in sample size and the nature of the design used.
Limitation of the study
Geographically, the study was limited to a single institution. In addition, there can be typical biases of retrospective studies including the possibility of misclassification of MAS, and this study did not explore MAS and did not link the severity of MAS risk factors to outcomes such as survival, neonatal morbidity, and stay in NICU.
Conclusion
In this study, preeclampsia, antepartum hemorrhage, prolonged duration of labor, premature rupture of membranes, and obstructed labor were correlated with admission for MAS at the NICU in Nigist Eleni Mohammed Memorial Comprehensive Specialized Hospital. Prevention, early identification, and appropriate management of these conditions may lead to a reduction in MAS but further prospective studies are required.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221124693 – Supplemental material for Determinants of meconium aspiration syndrome among neonates admitted to neonatal intensive care unit at Nigist Eleni Mohammed Memorial Comprehensive Specialized Hospital, South Ethiopia: Unmatched case–control study
Supplemental material, sj-docx-1-smo-10.1177_20503121221124693 for Determinants of meconium aspiration syndrome among neonates admitted to neonatal intensive care unit at Nigist Eleni Mohammed Memorial Comprehensive Specialized Hospital, South Ethiopia: Unmatched case–control study by Seifu Awgchew and Elias Ezo in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to thank data collectors, supervisors, and study participants for their openness to participate kindly provision of the necessary information and scarification of their valuable time. We also thank Wachemo University for funding this research.
Author contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all areas; took part in drafting, revising, and critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Availability of data
The data used for analysis are available on secure and reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical consideration
Ethical approval letters were obtained from Wachemo University’s ethical review committee WURCSVPO546/2014. A permission letter was also secured from the Nigist Eleni Mohammed Memorial Comprehensive Specialized Hospital.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received funding from Wachemo University for this study.
Informed consent
Oral informed consent was obtained from each neonate’s mother and the overall process was reviewed and approved by the ethical review committee of Wachemo University. The information obtained from them would not have been disclosed was informed. Coding was used to eliminate respondents’ names and other personal identification to ensure anonymity, privacy, and confidentiality.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.