
Abstract
Pleuroperitoneal fold abnormalities are thought to be responsible for congenital diaphragmatic hernias. It has also been theorized that pleuroperitoneal fold formation may indirectly result in ciliated foregut cysts by pinching off abnormal buds from the tracheobronchial tree. Although such abnormalities are typically recognized and corrected in infancy, their severity is variable. In some cases, pleuroperitoneal fold abnormalities persist and remain essentially asymptomatic into adulthood. We report a case of suspected pleuroperitoneal fold anomaly. The patient was found to have a thick membranous sac separate from the pleura covering the diaphragm without an associated hernia during thoracotomy for drainage of an unrelated empyema and lung abscess.
Keywords
Case Summary
The patient is a noninsulin-dependent 46-year-old diabetic man who presented with 2 months of right-sided pleuritic chest pain and fevers. His diabetes was poorly controlled due to inability to afford medications. Workup revealed a right middle lobe necrotizing pneumonia with empyema formation. After medical optimization, right thoracotomy with abscess drainage and debridement was performed. Once the right middle lobe had been completely debrided and the lung mobilized, further exploration revealed a thick membrane separate from the pleura, attached to the chest wall, and traversing the major fissure in which a smaller than normal-sized lower lobe was partially encased (Figures 1 and 2). The musculature of the right diaphragm below this shelf of tissue and the lower lobe of the lung appeared normal. After copious irrigation of the chest with warm saline, the membrane was left in place and the chest closed.
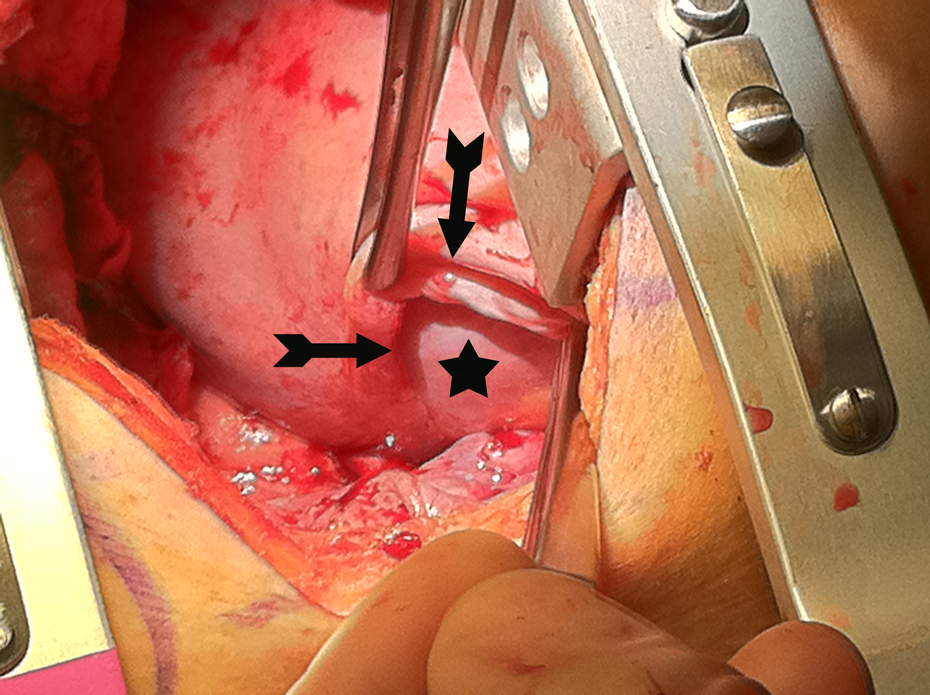
Arrows illustrate the pleuroperitoneal fold as found at the time of thoracotomy. The star marks the right lower lobe of the lung.

Arrows outline the edges of the pleuroperitoneal fold. The arrowhead marks the right lower lobe of the lung. The star illustrates the surface of the diaphragm.
The patient recovered well and was discharged home 1 week later. Chest imaging 4 weeks postoperatively demonstrated complete resolution of the pneumonia and normal expansion of the right lung. Diabetic control has also improved substantially.
Discussion
Normal diaphragm development proceeds in a stepwise manner beginning with folding of the septum transversum into a configuration that partially separates the pleuropericardial cavity from the peritoneum. Next, the pleuropericardial folds fuse with the septum transversum to form the pleuroperitoneal folds (PPFs). Myogenic cells and phrenic axons migrate into the PPFs, and the diaphragm is muscularized and innervated. 1
Several anomalies can occur during this process, and the range of presentations is quite variable. Based on experiments in mice, it has been theorized that malformation of the PPF results in Bochdalek hernia, a posterior (usually left) diaphragmatic hernia. The extreme end of the diaphragm malformation spectrum, eventration, is still poorly understood and likely results from a different pathologic mechanism.
Normal closure of the PPFs is theorized by some authors to be indirectly responsible for infradiaphragmatic bronchogenic cysts. 2 There are few such cases reported in the English-language literature. Bronchogenic cysts form from abnormal buds on the tracheobronchial tree and could be pinched off by PPF formation, trapping the cyst below what will eventually become the diaphragm. 3
Based upon its location and the lack of other anomalies at operation or on imaging, we theorize that the membrane found between the pleura and the diaphragm in our patient represents a remnant of the PPF, part of the primordial diaphragm that never became muscularized nor involuted. 4 We believe this is indicative of a spectrum of PPF anomalies ranging from life-threatening eventration or Bochdalek hernia to asymptomatic hernias and congenital remnants.