
Abstract
Background. Vitamin D deficiency (VDD) is a global health concern affecting people of all ages. The Ethiopian guidelines recommend sun exposure for neonates starting from 2 weeks old, with 15 to 20 minutes per day. However, evidence suggests that the implementation of this recommendation is inconsistent. Most studies conducted in Ethiopia regarding infant sunlight exposure have been limited to health facilities and towns. Objective. this study aimed to assess mothers’ practice, and factors affecting the sunlight exposure of their infants in Adami Tulu Jido Kombolcha district, East Shoa Zone, Oromia Region, Ethiopia, 2022. Method. A community based cross-sectional study design was conducted among 575 mothers with their infant’s from March 11 to 25, 2022. A lottery method sampling technique was employed to select local administrative units and systematic random sampling employed to select study participants. Practices and knowledge were assessed by categorizing mothers based on their responses to practice and knowledge questions, respectively. Mothers who scored above the mean value of 4.5 were classified as having good practice, while those who scored 6.9 or below on the knowledge questions were classified as having poor knowledge. Data were collected through face-to-face interviews using both semi-structured and structured questionnaires. The data were then entered into EPI Data version 3.1 and exported to SPSS version 25 for analysis. The association between variables was analyzed using bivariate and multivariable binary logistic regression and level of significant determined with adjusted odd ratio at 95% CI and P-value less than <.05. Result. All 575 mothers were interviewed and responded 100%. Out of 567 mothers, 55.2% had good practice of infant sunlight exposure. Lack of advice at health facility (AOR = 3.05, 95% CI: 1.08, 8.60), absence of postnatal care follow up (AOR = 2.38, 95% CI: 1.15, 4.94) and poor knowledge about sunlight exposure (AOR = 1.70, 95% CI: 1.15, 2.50) were factors associated with practice of infant sunlight exposure. Conclusions. In this study, more than half of the mothers had good practice of infants’ sunlight exposure. This study highlights the importance of improving maternal knowledge and healthcare practices related to infant sunlight exposure. Key factors affecting these practices include lack of advice at health facilities, absence of postnatal care follow-up, and poor maternal knowledge. To address these issues, healthcare providers, local health offices, and mass media should focus on educational programs and strengthening advice during health visits. Future research should use validated tools and mixed-method approaches to better understand the social and cultural factors at play. Establishing national guidelines and studying infant serum vitamin D levels can further enhance community awareness and promote the benefits of sunlight exposure.
Introduction
Sunlight comprises of 3 major wavelength bands: visible light, ultraviolet radiation (UVR), and infrared radiation. 1 The solar UVR penetrates deeper into the epidermis to induce vitamin D synthesis. 2 Exposure of the skin to solar ultraviolet B radiation is the major source of vitamin D in our body and Vitamin D is essential for the growth of healthy bones.3,4
For babies, exposure to sunlight has several health benefits. It is essential for the synthesis of vitamin D, which helps the body absorb calcium and builds stronger bones, protecting against diseases like osteomalacia in adults and rickets in youngsters. Furthermore, exposure to sunshine may be protective against several types of cancer. 5 Contrary to popular belief, excessive sun exposure does not lead to increased vitamin D levels; instead, it degrades vitamin D into inert photoproducts. Therefore, it is crucial to strike a balance between safe sunlight exposure to reap its benefits without causing harm. 6 Additionally, it’s important to limit sun exposure between 10 a.m. and 4 p.m., especially for infants. 7
Vitamin D deficiency (VDD) is a global health concern affecting people of all ages. Studies have shown that up to 1 billion individuals worldwide may have insufficient vitamin D levels, defined as a serum 25-hydroxyvitamin D (25(OH)D) level below 30 ng/mL. Specifically, among infants, VDD is a significant issue. 8 In Asia, research indicates that a majority of young infants have 25(OH) D levels below 30 nmol/L. For instance, 51% of infants in Turkey, 86% in Iran, 61% in India, and 61% in Pakistan fall into this category. 9 In the USA and African continent, the prevalence of VDD using a cutoff point of 25(OH)D <50 nmol/L is 18% and 34%, respectively.10,11 Unfortunately, in Ethiopia, there are currently no nationally representative data available on the Vitamin D status of the population. 12
Vitamin D insufficiency, which is common in many countries globally, especially in developing nations like India, China, Turkey, Iran, Egypt, and Nigeria, might be caused by poor maternal practices about exposing children to sunshine.13,14 In areas where it is not possible to obtain vitamin D supplements, insufficient exposure to sunshine may cause vitamin D deficiency (VDD). Rickets, skeletal demineralization, cardiovascular disease, cognitive decline, depression, adult-onset diabetes mellitus, osteoporosis, osteoarthritis, growth retardation, autoimmune diseases, and skeletal deformities in children are just a few of the health problems that are linked to VDD. Furthermore, infantile eczema can occur in newborns.15,16
Several studies have emphasized the variables that affect UVR exposure. Maternal age, level of education, size of family, husband’s educational background, marital status, employment status, fear of the evil eye, prenatal care visits, place of delivery, seasonal variations, geographic latitude and altitude, time of day, cloud cover, smog or pollution levels, skin melanin content, prolonged indoor internet activities, and sunscreen use are factors that affect exposure to UVR.17 -22
According to recent studies, getting outside every day is still the safest and most economical way to avoid vitamin D deficiency. 23 In order to prevent vitamin D insufficiency (VDD), it is recommended globally to take supplements of vitamin D, fortify milk or other foods with the vitamin, and make sure you get enough sunshine exposure. 24 Furthermore, in areas where the prevalence of rickets is higher than 1%, public health initiatives like routine vitamin D supplementation for breastfed children ought to be taken into consideration. It’s important to note, that our nation does not currently have such a program in place. 25
The Ethiopian guidelines recommend sun exposure for neonates starting from 2 weeks old, with 15 to 20 minutes per day in the morning time (8:00-10:00 a.m.) for unclothed or 30 minutes clothed daily. 26 However, evidence suggests that the implementation of this recommendation is inconsistent. Most studies conducted in Ethiopia regarding infant sunlight exposure have been limited to health facilities and towns. In contrast, our study focuses on rural areas, which have been less explored in this context. Surprisingly, there are few studies specifically addressing this topic in our study area, as confirmed by an extensive web search. Furthermore, the results of most Ethiopian studies indicate that mothers have inadequate knowledge and practice regarding infant sunlight exposure.19,27,28 Therefore this study aimed to assess mothers practice and factors associated with sunlight exposure of their infant in rural district of the study area.
Methodology
Study Design
A community based cross-sectional study was conducted.
Study Period and Area
The study took place from March 11 to 25, 2022, in the Adami Tulu Jido-Kombolcha district, located in the East Shoa zone of Oromia Regional State. This district is 1 of 10 in the East Shoa zone, central Ethiopia, situated 160 km from Addis Ababa and 115 km from Adama, the zone’s capital. The district comprises forty-three rural local administrative units, with a female population of 109 618, making up 51.15% of the total population. Health services in the district are provided by 7 public health facilities, 43 health posts, one non-governmental organization hospital, and one public hospital in the district. In 2022, 7983 mothers in the district gave birth. At the local administrative unit level, health care is delivered by health extension workers assigned to serve the local community.
Source Population
All mothers with infant who have a child less than 1 year living in the district.
Study Population
All mothers with infant who have child less than 1 year in the selected local administrative unit of the woreda.
Study Unit
Study unit was a randomly selected mother with infant who have child less than 1 year in the selected local administrative units.
Inclusion and Exclusion Criteria
Inclusion criteria
Mothers with infant who are resident (who lived in this local administrative units for greater than 6 months).
Exclusion criteria
Mothers who were unable to communicate and who are severely ill was excluded. Mothers with child less than 2 weeks, mothers with very low birth weight and infants without mothers or caregiver were excluded.
Sample Size Determination and Sample Selection
Sample size for the first specific objective was calculated by
Sample Size Calculation for Factors Associated With Mother’s Practice of Infant Sunlight Exposure, 2022.
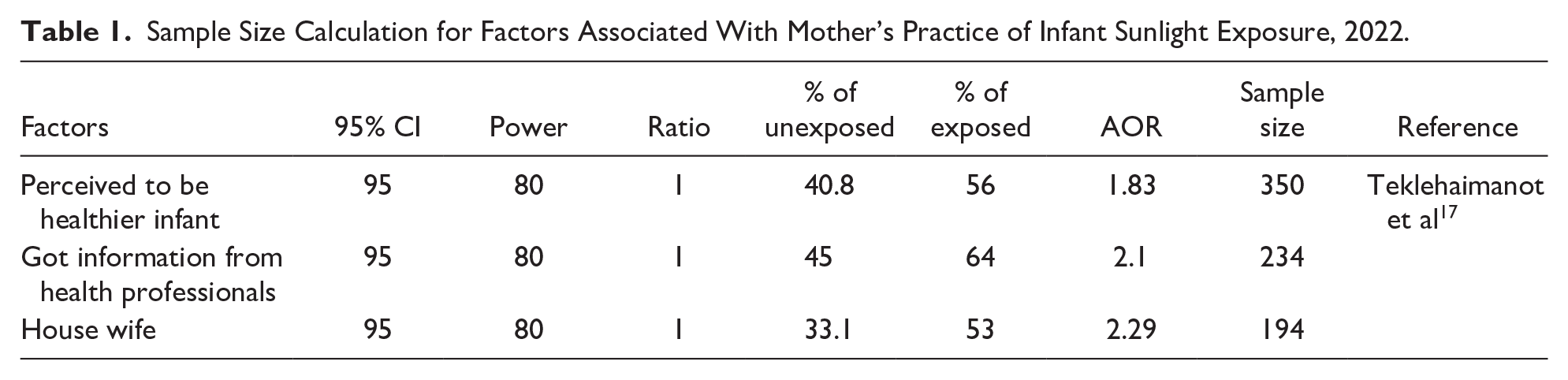
Finally, from the calculated sample size, the largest sample size from the first objective
Sampling Technique
Thirteen local administrative units of the Adami Tulu Jido Kombolcha district were selected by lottery method considering the rule of thumb of 30% coverage of representative of the study population. Based on information on the number of mothers with infants that was available from the family folder of the health extension worker, the sample size was distributed proportionately for each of the chosen local administrative units (Figure 1). After calculating the sampling interval (K = N/n = 2277/575 = 4), participants in each local administrative units were chosen using a systematic random sampling technique. The first home of a mother with an infant was chosen by lottery from these 4 and was placed in each local administrative unit to indicate the starting point of data collection.

Schematic representation of sampling procedure 2022.
In case where 2 infant of different mothers found in one household, only the mother of one infant was selected by lottery method. Additionally, if eligible respondents are not available after 3 visits during the survey, the next house with infants will be substituted, and the interval will continue from the previous house
Data Collection Instrument
Data were collected by using semi-structured and structured questionnaire with face-to-face interview. The data collection tools were adapted from different literatures.17,19,20,28,29,30 The questionnaire was first developed in English and translated into Afan Oromo versions and re-translated back into English by language experts to assure its consistency. The tools have 5 parts like socio-demographic factors, practice of mothers about infant sunlight exposure, health service utilization related factors, knowledge of mothers about sunlight exposure and attitude of mothers toward infant sunlight exposure.
Data Collection Procedures
Data collection was carried out through face-to-face interview. Six diploma nurse data collectors and 2 BSc nurse supervisors were involved. Data collectors were closely monitored and guided by supervisors. One-day training was given about data collection procedure for data collectors and supervisors regarding the study purpose, on how to conduct the interview, how to administer questionnaire, how to take consent, keep confidentiality and respect the right of the participant. The collected data was checked by the supervisor daily for completeness and finally the principal investigator evaluated the overall quality of data collection.
Study Variables
Dependent variable
Practice of infant sunlight exposure
Independent variables
Socio-demographic factors: age of the mother, marital status, educational status of mother, educational status of husband, occupation of mother, and family size.
Health service utilization related factors: ANC follow-up, Place of delivery, PNC follow-up
Knowledge of mothers about sunlight exposure: Source of information, time to expose infants to sunlight, benefits of sunlight exposure and harms of sunlight exposure
Attitude of mothers toward sunlight exposure: Believe about advantage of sunlight exposure, opinion about sunlight exposure, fear of exposing to sunlight and believe of effect on skin
Operational Definitions
Sunlight exposure Practice: Mothers’ activity in relation to sunlight exposure of infants.
Good versus poor practice: Mothers who answered the practice questions and scored above the mean value of 4.5 (as determined in this study) were classified as having good practice, whereas those who scored 4.5 or below were classified as having poor practice.17,19
Good versus poor knowledge: Mothers who answered the knowledge questions and scored above the mean value of 6.9 (as determined in this study) were classified as having good knowledge, whereas those who scored 6.9 or below were classified as having poor knowledge.20,31
Good versus poor attitude: Mothers who answered the attitude questions and scored above the mean value of 21.91 (as determined in this study) were classified as having good attitude, whereas those who scored 21.91 or below were classified as having poor attitude. 20
Data Quality Control
Pretest on 5% of the sample size (29 mothers) among mothers in korme Bujure in Adami Tulu Jido Kombolcha, which was not selected for the actual study was conducted. Pretest was done to assess questionnaire’s completeness, clarity, skip patterns and correctness of filled questionnaires. Besides this 1 day training was given for data collectors. The training focused on how to complete the questionnaire, proper interview techniques, and proper asking was given for data collectors and supervisors before data collection. In addition, check for completeness and quality of data collection was made on daily bases by the supervisors and detailed feedback was provided to data collectors and correction was given by principal investigator next morning if any inconsistency and incompleteness was observed.
Data Analysis Plan
Data were checked for completeness and consistency. Then, coded and entered into EPI Data version 3.1 and analyzed by using SPSS Software version 25. The data were cleaned for inconsistencies and missing values. Then, descriptive statistics such as proportion, frequencies, cross tabulation, and measure of central tendency were calculated and presented by tables and figures.
Bivariate analysis was used to see the association between each independent variable & the outcome variable, and all variables with P-value < .25 was taken into the multivariable analysis to control for all possible confounders. Then, multivariable logistic regression analysis with 95% confidence interval was calculated for statistical significance after Hosmer and Lemeshow checked for model fitness. Multi-collinearity test was used to identify correlation between independent variables. Those variables with p-value less than 0.05 were considered statistically significant and the results were reported with adjusted Odds Ratio and 95% CI.
Results
Socio-Demographic Characteristics of Respondents
All the required 575 study participants were interviewed and responded, resulting in 100% response rate. The mean age (±SD) of the participants was 27.3 (±5.4) years. Three hundred eighty-seven (67.3%) mothers had infants less than or equal to 6 months old. One hundred eighty-nine (32.9%) mothers had an age range of 25 to 29 years old. The majority (567; 98.6%) of mothers were married, 338 (58.8%) mothers had reached grade 1 to 8 in their educational status, and 554 (96.3%) of mothers were housewife in their occupation. Three hundred thirteen (54.4%) mothers had 4 to 6 family members. Only 6 husbands had degree and above in their educational status (Table 2).
Socio-Demographic Characteristics of Study Participants, 2022.

Health Service Utilization Related Factors to Sunlight Exposure
In this study the majority of respondents 540 (93.9%) had ANC follow-up. Out of 540 mothers who had ANC, 53.5% of mothers had good practice of infant sunlight exposure. But only 36 (6.7%) of 540 mothers were advised to expose their infant to sunlight. However out of 63 mothers who had PNC follow-up, 45 (71.4%) of mothers had good practice of infant sunlight exposure and 26 (41.3%) of mothers had advised about sunning of their infant. Moreover from 471 (81.9%) mothers who had delivered in the health facility, 54.6% of mothers had good practice of infant sunlight exposure and only 34 (7.2%) were advised about sunning of their infants (Table 3). Although mothers visited health facilities and received advice, the findings suggest that they may have forgotten parts of the discussion. This indicates that the advice was likely given but not fully remembered by the mothers. Therefore, it is important to communicate the advice in more effective ways to ensure it is retained.
Health Service Utilization by Mothers, 2022.

Knowledge of Mothers About Sunlight Exposure
Out of all the respondents, 98.3% of mothers indicated that they were aware of infant sunlight exposure. Out of these 196 (34.7%) heard information from health professionals and 550 (97.3%) of mothers heard from elders and neighbors. Five hundred sixty-four (99.8%) of mothers mentioned that infant sunlight exposure is beneficial and 244 (43.3%) of them mention that it is beneficial to strengthen bone. All of the respondents had knowledge of good time to expose infant in the morning 100%. Forty-nine (8.7%) had knowledge of harmful effect of sunlight exposure and 31 (63.3%) of these mothers said that sunlight exposure exposes infant to sickness. Three hundred eighty-seven (68.5%) had knowledge of infants should be exposed to sunlight between 2 and 4 weeks (Table 4).
Knowledge of Mothers About Sunlight Exposure, 2022.

From the above 8 knowledge questions, the mean score value of mothers who had knowledge about sunlight exposure of infants was calculated and it was 6.89. Out of 565 respondents 260 (46%) of the respondents were scored less than this mean value. Therefore, about 46% of mothers had poor knowledge about infant sunlight exposure while 56% had good knowledge toward sunlight exposure.
Attitude of Mothers Towards Sunlight Exposure
Among all respondents 374 (65.0%) of mothers agree that sunlight exposure is advantageous to child’s health and 69 (12%) of mothers strongly disagree that sunlight exposure has bad effect on child’s skin. Out of total respondents 176 (30.6%) and 316 (55.0%) strongly agree on believe that exposure to sunlight helps child to become healthy and strong respectively. Moreover 373 (64.9%) of participants strongly disagree that exposure to sunlight prevents child from sleeping well. Likewise 181 (31.5%), 234 (407%) of mothers strongly disagree that sunlight exposes child to cold/pneumonia and sickness respectively. Out of 575 mothers, 371 (64.5%) strongly disagree that fear of evil eye in exposing infants to sunlight (Table 5).
Attitude of Mothers Related Factors About Sunlight Exposure, 2022.

From the above 8 attitude questions, the mean value was calculated and it was 21.91. Out of 575 respondents 236(41%) of the respondents were scored less than this mean value. Therefore, about 41% of mothers had poor attitude toward infant sunlight exposure while 58.96% mothers had good practice (Figure 2).

Level of mother’s attitude toward infant sunlight exposure, 2022.
Practice of Mothers About Sunlight Exposure of Their Infants
In this study, out of 575 participants almost all (567; 98.6%) mothers intentionally expose their infant to direct sunlight. Two hundred seventy-nine (49.2%) of mothers start to expose their infants within 2 to 4 weeks old and 85 (15%) of mothers exposes their infants daily. furthermore, 337 (59.4%) exposes their infants between 2 and 4 hours in the morning and 283 (49.9%) exposes for 16 to 30 minutes. Moreover 540 (95.2%) of mothers exposes their infants unclothed and 543 (95.8%) mothers exposes outdoor. Regarding application of lubricants 564 (99.5%) of mothers apply lubricants and only 43 (7.6%) of mothers apply after sunlight exposure (Table 6).
Mothers Practice of Infant Sunlight Exposure, 2022.

From the above (Table 6) 9 practice questions those questions with more than 2 category were re-coded in to 2 category before doing computation by giving “1” value for the correct practice category and “0” for others. After computation, normality of the computed total practice was checked and it was normal. The mean score value of mothers who had practice of sunlight exposure of infants was calculated and it was 4.54. Two hundred fifty-four (44.8%) of the respondents were scored less than this mean value. Therefore, about 55.2% of mothers had good practice about infant sunlight exposure (Figure 3).
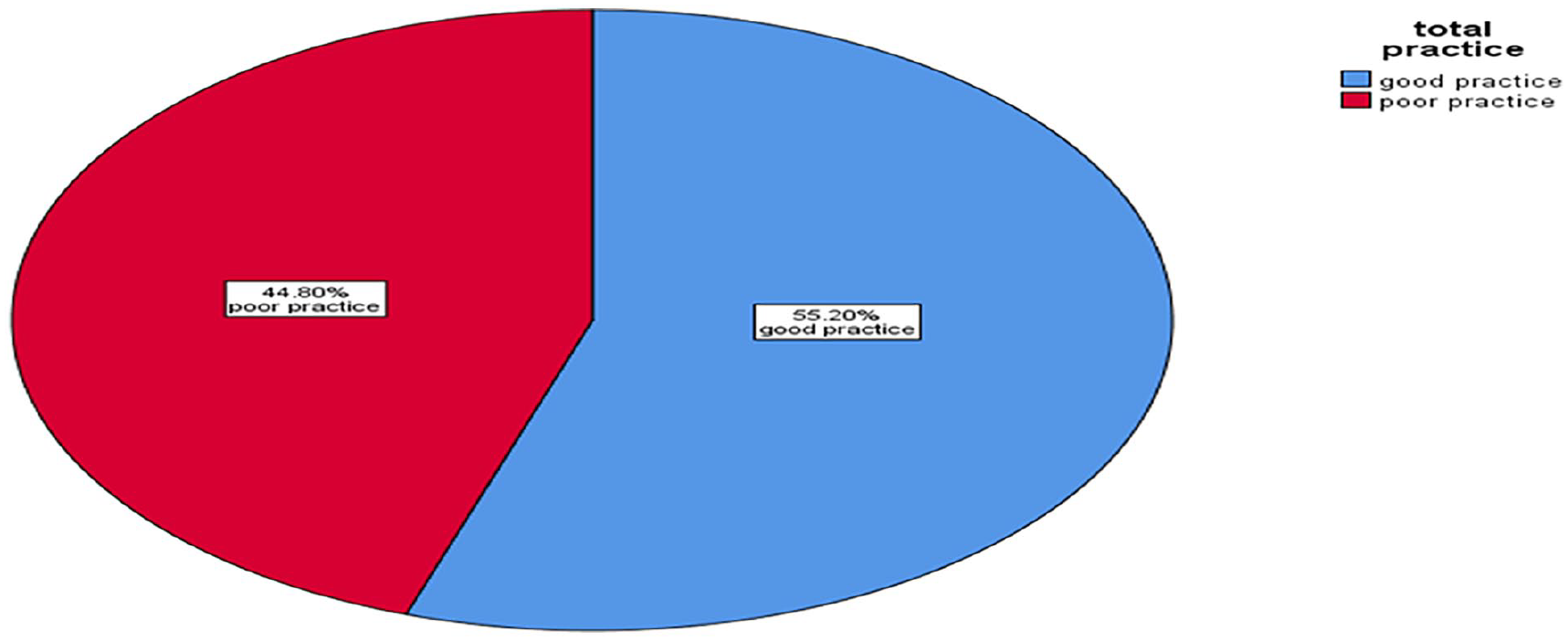
Practice of infant sunlight exposure among mothers 2022.
Factors Associated With Practice of Infant Sunlight Exposure
In bivariate analysis, ANC and PNC follow-up, getting advice during ANC and PNC follow-up, getting advice at health facility on the day of delivery and knowledge of mothers were associated significantly at P value < .25 and selected as a candidate for multivariable logistic regression. Then after checking for auto-collinearity one variable namely did you have ANC follow-up was discarded from multivariable analysis. Again from the 6 variables, a variable have you had advised during PNC visit has many system missing so that it doesn’t entered in multivariable analysis. Enter method was applied to enter variables in the multivariable analysis. Hosmer and Lemeshow test was checked and it was 0.65.
Those mothers who have advised in the health facility on the day of delivery about infant sunlight exposure were 3.05 times (AOR = 3.05, 95% CI: 1.08, 8.60) more likely to have good practice toward infant sunlight exposure than those who did not got advised. Again, those mothers who have PNC follow-up were 2.38 times (AOR = 2.38, 95% CI: 1.15, 4.94) more likely to have good practice toward infant sunlight exposure than who haven’t PNC follow-up. Moreover, the result of this study showed that those mothers who have good knowledge regarding infant sunlight exposure were 1.70 times (AOR = 1.70, 95% CI: 1.15, 2.50) more likely to have good practice infant sunlight exposure than those who have poor knowledge (Table 7).
Bivariate and Multivariable Analysis of Factors Associated With Mothers’ Practice of Infant Sunlight Exposure, 2022.
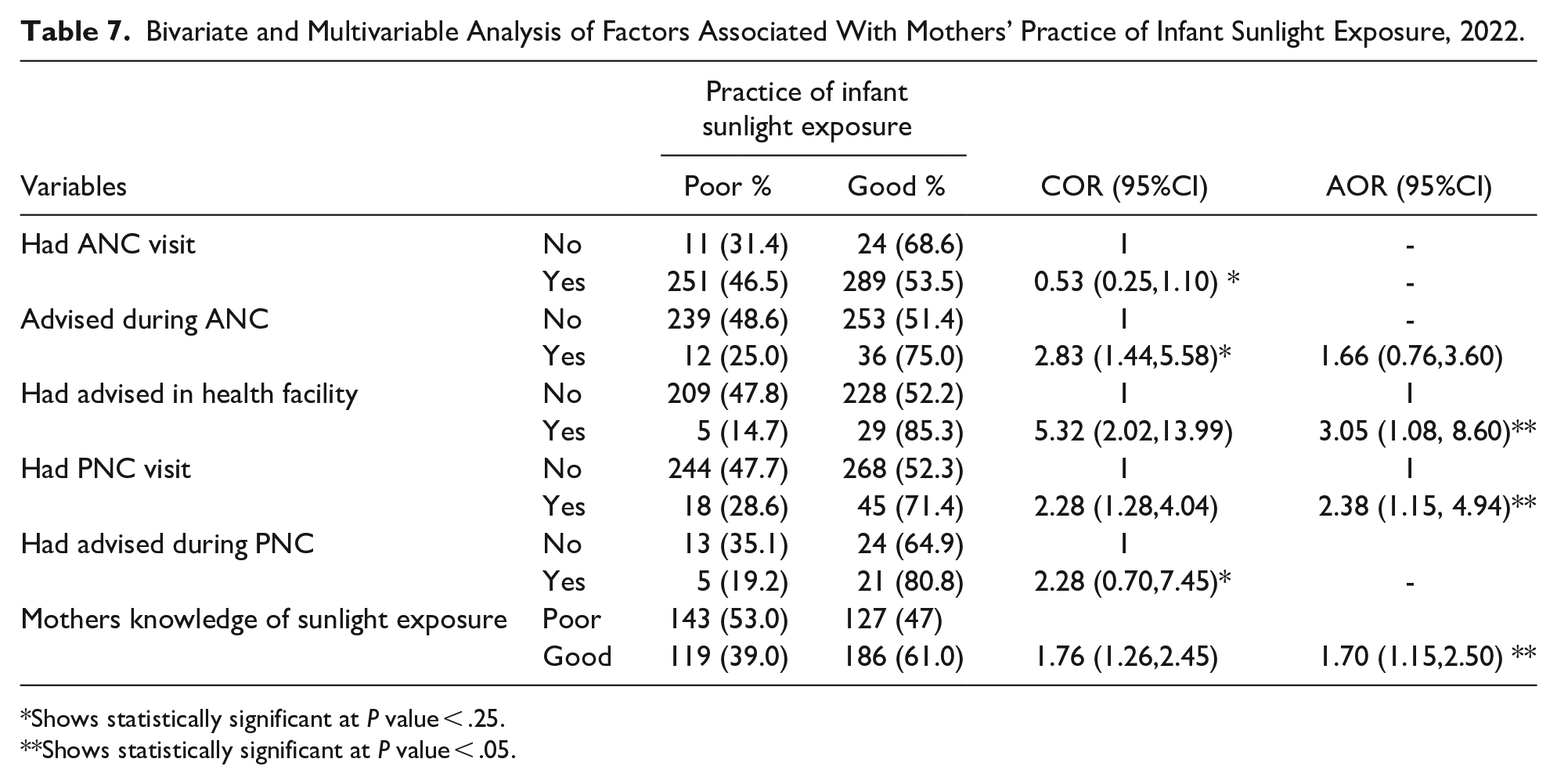
Shows statistically significant at P value < .25.
Shows statistically significant at P value < .05.
Discussions
This study was carried out to assess practice of mothers and associated factors concerning sunlight exposure of their infants in Adami Tulu Jido Kombolcha, East Shoa Zone, Oromia region, Ethiopia. In this study the finding of good practice of infant sunlight exposure was 55.2%. This finding is in line with the study conducted in Yirgalem Hospital 18 which showed 54.5% had good practice. But it lower than the result of study done in Debra Berhan town which shows 65.7% of mothers had good practice. 17 This difference might be due to the study setting. This study was done on those residing in rural area while that of Debra Berhan town was considers those residing in town. Another reason for this discrepancy was the source of information and the coverage of advice given for mothers with infants during ANC, PNC and on the day of delivery in the facility was much lower than the result of Debra Berhan.
About 70.5% of mothers in Debra Berhan town heard information from health professionals and 45.9% of mothers got advice in the health facility on the day of delivery, 17 but in this study only 34.7% of mothers heard information from health professionals and only 7.2% of mothers got advice in the health facility on the day of delivery . In contrast to this the finding of this study is good as compared to the finding of similar study done in Debra Markos town which was 55.4% of mothers had poor practice of infant sunlight exposure. 19 This discrepancy might be due to climatic condition. This study area is in a hot area in rift valley land while that of Debra Markos town was cold.
The finding of this study showed that 98.6% of mothers did intentionally expose their infant to direct sunlight. This result is similar with the finding of similar study done in Debra Berhan town which was 99.1%, 17 but it is higher than the result of study done in Aleta Wondo Health Center 30 and Yirgalem Hospital 18 in Sidama region of Ethiopia which shows 80.1% and 84.7% respectively. This discrepancy might be due to difference in cultural factors like fear of cold/pneumonia, fear of evil eyes and level of appropriate information concerning of infant sunlight exposure.
In this study the result showed about 279 (49.2%) of mothers started exposing of their infants within 2 to 4 weeks. This finding was higher than that of the result of study done in Debra Markos town, 19 Debra Berhan town 17 and that of Paul’s hospital 32 which was 31.8%, 12.6%, and 41.4%, respectively. This difference might be due to cultural difference and respondent’s source of information. Similarly, the finding of this study revealed that 543(95.8%) of mothers exposed their infants outdoor. This finding was slightly higher than the result of study done in Debra Markos which was 89.4%. 19
This study revealed that out of 567 mothers those who expose their infants to direct sunlight exposure intentionally, only 85 (15%) of mothers exposes their infants daily. This finding is lower than the result of study done in South Gondar Zone which was 45.7% 28 as well as lower than the study done in Debra Berhan town which was 61.3%. 17 This difference might be due to the difference in setting of the study. This study considers those residing in rural area and community based, while that of Debra Berhan considered those in the town where access to health care is good than rural and that of south Gondar zone also done health facility based. The finding of this study showed that 165 (29.1%) of mothers exposed their infants for 15 to 20 minutes time duration. This is one evidence of poor practice of infant sunlight exposure as Ethiopian guidelines recommends every infants should be exposed to sunlight for 15 to 20 minute duration. 26
The finding of this study shows that 540 (95.2%) of mothers exposes their infant unclothed. This is too much higher than the study done in South Gondar zone which was only 25% of mothers uncovered their infants. 28 This might be due to 55.7% of mothers in South Gondar zone covered their infants to prevent from evil eye. However this result is slightly comparable with the result of study done in Aleta Wondo health center which was 90.0% (35). Moreover, the present study shows that only 10 (1.8%) of mothers exposes their infants with diapers and eye protection. This is incongruent with the result of study done Debra Berhan which shows 55.2% of mothers were exposing their infants with diapers. 17 This disparity might be due to more of the source of information of sunlight exposure in Debra Berhan town was from health professional and 45.6% of mothers who delivered in health facility were advised about sunlight exposure.
The present study revealed that 337 (59.4%) of mothers were exposing their infants to sunlight between 2 and 4 hour a.m. This is lower than the finding of study done at Aleta Wondo health center which was 90.0%. 30 Regarding application of lubricants on the infant’s body, 564 (99.5%) of mothers apply lubricants on their infant’s body. Out of those who apply lubricants 471 (83.5%) of mothers apply during the time of sunlight exposure. This finding is not in agreement with the result of study done in Debra Markos town which was (98.4%) of mothers applied lubricants for their infants and 70.6% of those applied lubricants were during the time of sunlight exposure. 19 The possible reason behind this might be that the difference in mothers traditional practice. However the result of this study which shows only 7.6% of mothers had applied lubricants after sunlight exposure was lower than the result of study done at Aleta Wondo health center which was 38.7%. 30 This indicates that it is very important to increase the awareness of communities regarding appropriate practice of infant sunlight exposure so that enough amount of cutaneous production of vitamin D will be there.
The study found that mothers who received advice about infant sunlight exposure at the health facility on the day of delivery were 3.05 times more likely to practice proper infant sunlight exposure compared to those who did not receive such advice. This highlights the importance of providing guidance on infant sunlight exposure to mothers at the health facility on the day of delivery.
The study also found that mothers who attended postnatal care (PNC) follow-ups were 2.38 times more likely to practice proper infant sunlight exposure compared to those who did not attend PNC follow-ups. This could be because PNC visits provide mothers with sufficient and adequate knowledge, enabling them to practice good sunlight exposure for their infants.
The study revealed that mothers with good knowledge about infant sunlight exposure were 1.70 times more likely to practice proper infant sunlight exposure compared to those with poor knowledge. This finding aligns with a study conducted in Addis Ababa on neonatal sunlight exposure, which also showed that having good knowledge about infant sunlight exposure was associated with better practice. 29
The study was used primary data and conducted using community-based design which would help to know the mothers practice to sunlight exposure at the community level. However, the information was self-reported and no experience of the mother was observed. Due to this there might be social desirability bias and respondents might respond what they did not experience. In addition, the tool for this study is not validated tool and it’s was adapted from the different literatures. Additionally, study not used mixed design (qualitative and quantitative) to address social and cultural issue. Furthermore, there are no established national guidelines or precise criteria for operationalizing practice, knowledge, and attitude. Instead, the study relied on various literature sources to inform the assessment.
Conclusions and Recommendations
According to the result of this study about 55.2% demonstrated good practice in infant sunlight exposure. Getting an advice in the health facility on the day of delivery, having postnatal care follow-up and having good knowledge about sunlight exposure had significant association with mothers’ practice about sunlight exposure of infants in multivariable analysis. However, there are still gaps in sunlight exposure practices. These gaps may be due to issues related to the timing of starting sunlight exposure, duration of exposure, and application of lubricants and shortage of the number of days compared to the recommended duration.
Mass media, local administrative unit health office, district health office, and healthcare providers should focus on improving maternal knowledge about the importance and benefits of infant sunlight exposure through educational programs and informational materials. It is crucial for healthcare professionals to offer and strengthen advice on infant sunlight exposure during health facility visits. Furthermore, promoting regular postnatal care follow-up can help reinforce good practices related to infant sunlight exposure.
Future studies should use validated tools to ensure the reliability and accuracy of the data collected. Incorporating both qualitative and quantitative methods in future research can provide a more comprehensive understanding of the social and cultural factors influencing maternal practices. Additionally, establishing national guidelines or precise criteria for assessing practices, knowledge, and attitudes related to infant sunlight exposure would standardize the evaluation process. Furthermore, study on determining infant’s serum vitamin D level among infants who are adequately exposed and poorly exposed to sunlight were recommended for researcher so that the community will understand more about the benefits of sunlight exposure.
Footnotes
Acknowledgements
The authors would like to thank the Hawassa University College of Medicine and Health Science and School of Public Heath for cooperation and invited the version of this manuscript presentation as a thesis, Oromia regional health office, East Shoa zone health office, Adami Tulu Jido Kombolcha woreda health bureau and administrative office, Woreda health extension worker, data collectors, supervisors and study participants for their cooperation in the study.
Abbreviations and Acronyms
AOR Adjusted Odds Ratio
BSc Bachelor of Science
CI Confidence Interval
COR Crude Odds Ratio
HEW Health Extension Worker
25(OH)D 25-hydroxyvitamin D
IRB Institutional Review Board
PNC Postnatal Care
SPSS Statistical Package for Social Science
UVB Ultraviolet B
UVR Ultraviolet Radiation
VDD Vitamin D deficiency
Authors’ Contributions
AHH, AHM, and WTK conceptualized the study, developed the tool, conducted the research, carried out the statistical analysis, and wrote manuscript. ELS, BFW, FYJ, and AAD participated in the design of the study and tool development, performed statistical analysis, and drafted the manuscript. All authors read and approved the final manuscript.
Data Availability Statement
Data availability for this article is available up on request for principal investigators. Additionally, the local language versions of the survey tool are available from the authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statements
Ethical clearance was obtained from Institutional Review Board (IRB) of Hawassa University College of Medicine and Health Science with IERC protocol number (Ref.No_HUCIB/IRB/082/14). Official support letter from the school of public health was written to Oromia regional health bureau. Again the Oromia regional health bureau was wrote a supportive letter to East Shoa zone health bureau. Then East Shoa zone health bureau also wrote for us a supportive letter to Jido Kombolcha woreda health bureau. Then the woreda health bureau wrote a permission and supportive letter to each selected kebeles administration and health extension worker. An approved oral informed consent by ethical committee was obtained from respondents after explaining the study’s purpose and objectives. To ensure confidentiality, respondents’ names were replaced with code numbers. Participants were given the opportunity to ask any questions about the study and were free to refuse or stop the interview at any time.
Trial Registration Number/Date
Not applicable.
Other Journal Specific Statements
Not applicable.